
Abstract
With ongoing earlier enrollment on and rapid scale-up of antiretroviral therapy (ART) in Cameroon, there are increasing risks of transmitted HIV drug resistance (HIVDR) at population levels. We, therefore, evaluated the threshold of HIVDR in a population initiating ART, to inform on the effectiveness of first-line regimens, considering HIV-1 diversity, plasma viral load (PVL), and CD4-based disease progression. A total of 53 adults [median (interquartile range, IQR) CD4: 162 cell/mm3 (48–284); median (IQR) PVL: 5.34 log10 RNA (4.17–6.42) copies/ml] initiating ART in 2014 at the Yaoundé Central Hospital were enrolled for HIV-1 protease–reverse transcriptase sequencing. Drug resistance mutations (DRMs) were interpreted using the 2009 World Health Organization (WHO) list versus the Stanford HIVdb algorithm version 7.0. Level of DRMs was low (3.77%) versus moderate (7.55%), respectively, following the WHO list (T69D, K103N) versus Stanford HIVdb (T69D, A98G, K103N, K238T), respectively. Prevailing clade was CRF02_AG (71.70%). Based on Stanford HIVdb, a slightly higher proportion of patients with DRMs were found among ones infected with CRF02_AG than in those non-CRF02_AG infected (7.89% vs. 6.67%, p = 1.000), with lower PVL (7.69% <5.5 vs. 0% ≥5.5 log10 RNA copies/ml, p = .488) and with higher CD4 counts (9.52% CD4 ≥200 vs. 3.33% CD4 <200 cells/mm3, p = .749). Thresholds of DRMs suggest that standard first-line regimens currently used in Cameroon may remain effective at population levels, despite scale-up of ART in the country, pending adherence, and closed virological monitoring. With an intent-to-diagnose approach, the discrepant levels of DRMs support using Stanford HIVdb to evaluate initial ART, while revising the WHO list for surveillance.
O
Any major drug resistance mutation (DRM), detected before initiating ART, serves as a well-defined clinical prognosis of poor response to the related treatment. 5 Thus, wherever possible, genotypic resistance testing (GRT) is considered as state of the art in managing patients initiating ART. In contrast to the Western world, practicability of GRT remains clinically unaffordable in LMICs, thereby supporting population-based HIVDR surveillance to raise awareness and to inform on potentially active first-line regimens for LMICs. 4,5
As earlier enrollment on and rapid scale-up of ART (10.3% increase in national coverage from 2013 to 2014, with a total of 145,038 treated individuals) are underway in Cameroon, 6 we sought to ascertain the threshold of HIVDR in populations initiating ART (prevalence <5%, 5%–15%, >15%, respectively, indicates low-, moderate-, and high-level resistance 4 ) for evidence-based policy on the effectiveness of commonly used first-line ART [EFV + tenofovir (TDF) + FTC or 3TC as preferred combination, followed by NVP + zidovudine (AZT) +3TC], considering HIV-1 diversity, plasma viral load (PVL), and CD4-based disease progression.
We conducted a prospective study among HIV-infected adults (ART naive or with ≥3 months ART interruption) initiating ART from January to March 2014 at the Yaoundé Central Hospital in Cameroon, evaluating DRMs as per current WHO recommendations.
7
The study was institutionally approved by the Chantal BIYA International Reference Centre (CIRCB) for research on HIV/AIDS prevention and management in Cameroon (Ref. No. 68 PTA CIRCB-2014), all patients were consented before enrollment, and confidentiality was ensured. Sociodemographic and clinical data were recorded, including CD4 T-cell count and PVL. HIV-1 protease (PR)–reverse transcriptase (RT) genotyping was performed using an in-house sequencing assay at the Sequencing and Bioinformatics unit of the CIRCB, as previously described.
8
DRMs were interpreted for nucleoside RT inhibitors (NRTI), non-NRTI (NNRTI), and PR inhibitors (PI), using the following two recommended methods: (a) the 2009 WHO surveillance DRM list (WHO list) as described by Bennett et al., in 2009
4
and (b) the Stanford HIVDR Database (HIVdb) version 7.0, where DRMs were defined as those conferring a genotypic susceptibility score with high-, intermediate-, or low-level resistance to ARVs (updated June 22, 2013) based on mutation penalty scores (
Fisher's exact test was used to evaluate association between DRMs and the following variables: HIV-1 subtype, range of PVL, disease progression based on CD4 T-cell count. p-Values <.05 were considered as statistically significant. 9
Fifty-three patients were enrolled: 58.49% of them were female, with a median (interquartile range, IQR) age of 38 (31–44) years, median (IQR) CD4 T-cell count of 162 (48–284) cell/mm3, and a median (IQR) PVL: 5.34 log10 RNA (4.17–6.42) copies/ml. Among these patients, 49 were ART-naive, while 4 were reinitiating first-line ART [AZT +3TC + NVP, 1 case; AZT +3TC + EFV, 2 cases; AZT + D4T (AZT) + EFV, 1 case; ART duration (min-max): 7–14 months] after a prolonged interruption [median (min-max): 19 (8–32) months].
Based on the WHO list, a low level of HIVDR (3.77%; 2/53) was reported, due to the presence of mutations T69D (intermediate resistance to didanosine) and K103N (high resistance to both NVP and EFV). Based on HIVdb, a moderate level of HIVDR (7.55%; 4/53) was reported, due to the presence of the following mutations: T69D (intermediate resistance to didanosine), A98G (intermediate resistance to NVP), K103N (high resistance to both NVP and EFV), and K238T (high resistance to NVP and intermediate resistance to EFV). In addition, HIVdb reported other RT mutations (T69N, V90I, V106I, E138A) with little or no effects on RT inhibitor susceptibility unless they emerge concomitantly with a major DRM (Table 1). In the PR region, the following PI minor mutations were found using HIVdb: K20I (42/53, 79.25%), known as a consensus amino acid in CRF02_AG and subtype G with no effect on PI susceptibility, and L10I/V (13/53, 24.53%), known as PI-selected polymorphisms. Interestingly, these PI polymorphisms are also known to have no effect on RT inhibitor susceptibility. Patients previously exposed to ART had no relevant DRMs.
(a) 2009 WHO SDRM list; (b) Stanford HIVdb algorithm version 7.0.
ART, antiretroviral therapy; NA, not applicable; SDRM, surveillance drug resistance mutation; WHO, World Health Organization.
Of the 53 sequences, subtyping revealed CRF02_AG as the most prevalent clade (71.70%), followed by subtypes A1 (5.66%), G (3.77%), CRF01_AE (3.77%), CRF09_cpx (3.77%), and single pure subtypes or recombinants (D, F1, CRF13_cpx, CRF18_cpx, CRF02_AG.CRF22_01A1), (Fig. 1); which in turns supports previous findings in the same country (8,10).
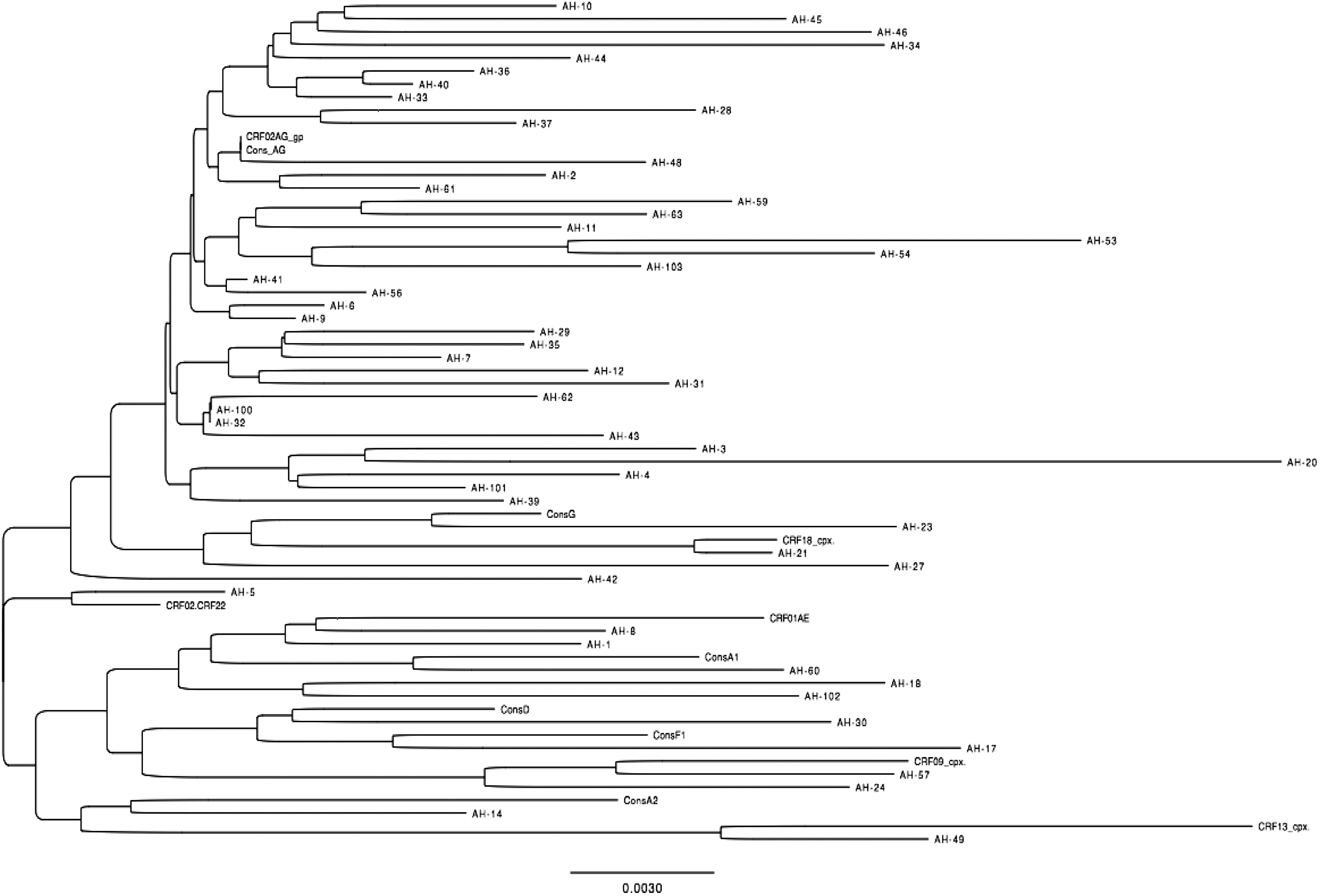
Phylogenetic tree of evolutionary relationships among HIV-1 sequences from 53 HIV-infected adults initiating antiretroviral therapy at the Yaoundé Central Hospital in Cameroon. The evolutionary history was inferred using the Neighbor-Joining method. The optimal tree with the sum of branch length = 0.50207645 is shown. The percentage of replicate trees in which the associated taxa clustered together in the bootstrap test (1,000 replicates) is shown next to the branches. The tree is drawn to scale, with branch lengths in the same units as those of the evolutionary distances used to infer the phylogenetic tree. The evolutionary distances were computed using the Kimura 2-parameter method and are in the units of the number of base substitutions per site. The rate variation among sites was modeled with a gamma distribution (shape parameter = 1). The analysis involved 65 nucleotide sequences (53 sequences from the study population and 12 reference sequences). Codon positions included were 1st +2nd +3rd+Noncoding. All positions containing gaps and missing data were eliminated. There were a total of 595 positions in the final data set. Evolutionary analyses were conducted in MEGA6.
Based on HIVdb, the prevalence of DRMs was slightly higher in patients infected with CRF02_AG [7.89% (3/38) vs. 6.67% (1/15) in non-CRF02_AG infected patients; p = 1.000], with PVL <5.5 log10 RNA copies/ml [7.69% (2/26) vs. 0.00% (0/25) in patients with PVL ≥5.5 log10 RNA copies/ml; p = .490], or with CD4 cell count ≥200 cells/mm3 [9.52% (2/21) vs. 3.33% (1/30) in patients with CD4 <200 cells/mm3; p = .561].
Trends of HIVDR among ART initiators are currently of great asset to inform LMIC policy-makers on three distinct public health considerations as follows: (a) switching first-line ART from NNRTI-based to PI-based regimens, (b) introducing individual pre-ART genotyping to guide therapy wherever feasible, or (c) intensifying viral load monitoring within the first 12 months following ART initiation. 2 –4,7
With low (WHO list) and moderate (HIVdb) levels, HIVDR among ART initiators is not yet at the high level (<15%); this suggests continuing ART with current first-line regimens and reinforcing PVL monitoring, while confirming these findings on a larger population. 4 Similar discrepancies were reported in Spain with different context-specific implications. 10 Further discrepancies in our study are due to detection by HIVdb of E138 mutation (affecting second-generation NNRTIs) and other mutations known to possibly jeopardize future treatments; the case of K238T warrants additional data to confirm/infirm reduced susceptibility to both first- and second-generation NNRTIs. 11 Nonetheless, an intent-to-diagnose approach supports the use of HIVdb algorithm in assessing DRMs among ART initiators, due to its regular updates, broad HIV-1 diversity (B and non-B subtypes), wide range of treatment scenarios, and availability of clinically relevant genotypic susceptibility scores. Indeed, because our methodological approach follows the 2014-updated recommendation from the WHO to assess DRMs among naive populations, we believe that our findings would be contextually suitable and could help in the further selection of the appropriate algorithm to study DRMs in pretreated populations (which are generally chronically infected), who might have different DRMs profile compared to DRMs from recently infected populations. Revising the WHO list, in the frame of HIVDR surveillance components (i.e., for use either among recently infected or ARV-pretreated individuals), might be considerable.
Absence of DRMs, among previously treated patients, suggests reinitiating first-line ART under close PVL monitoring for possible DRM(s) in sanctuaries/minority quasispecies, as well as the poor forgiveness of nonadherence with NNRTIs. 10,12 Pending larger surveys, it therefore seems commendable to continue with current first-line ART (consistent with tenofovir-containing NNRTI-based regimens as preferred first-line ART, in an era of stavudine phasing out), 11 while intensifying adherence support, PVL monitoring, and performing GRT following virological failure. 11,13 Although nonsignificant, trends of HIVDR according to virological and immunological profile are consistent with previous reports, excepting data from Free State. 5,11,14 Moreover, ensuring adherence and continuous drug supply would support ART effectiveness, while data on transmitted HIVDR among recently infected populations would be complementary. 15,16
Conclusively, based on the WHO threshold, the low (WHO list) and moderate (Stanford HIVdb) levels of DRMs suggest maintaining current first-line ART and intensifying virological monitoring, despite scale-up of ART in the country. With an intent-to-diagnose approach, HIVdb appears more informative in assessing the effectiveness of first-line ART among initiators. Enlarged population-based HIVDR surveillance studies would provide a wider representativeness of resistance and its peculiarities across geographical settings, viral diversity, and disease stages in LMICs facing similar programmatic challenges.
Footnotes
Acknowledgments
This study was financially supported by the CIRCB for research on HIV/AIDS prevention and management, under the approved 2014 annual work plan, both for laboratory analysis and for Joseph Fokam's participation to the symposium on new guidelines for the surveillance of HIVDR, organized by the WHO at AFRAVIH 2014.
The Poverty Related Diseases College and HIV Research Trust supported capacity development on the virological interpretation of antiretroviral drug-resistant mutations in Italy and in the United States.
Haniel Akonie Ze gained research experience for his MD thesis at the Faculty of Medicine and Biomedical Sciences, under the lead supervision of Alexis Ndjolo.
This work is dedicated to late Marcel Monny Lobe, former Administrator of the CIRCB for research on HIV/AIDS prevention and management and by then Senior Lecturer at the Faculty of Medicine and Biomedical Sciences, for his effort at the start-up phase of CIRCB.
Author Disclosure Statement
No competing financial interests exist.