
Abstract
The aim of this study was to evaluate the impact of HIV-1 very low-level viremia (<50 copies/ml) on the 2-year risk of virological failure. A retrospective analysis including HIV-positive patients presenting two consecutive HIV RNA below 50 copies/ml (outpatient clinic in Italy, first semester of 2010) was performed. HIV RNA was measured through real time polymerase chain reaction (PCR) assay CAP/CTM HIV-1 version 2.0 (detection limit: 20 copies/ml) and stratified as undetectable RNA (“Target Not Detected”, TND), <20 copies/ml, 20–50 copies/ml. After 96 weeks virological failure was defined as two consecutive viral loads above 50 copies/ml. Log-rank tests and a multivariate Cox proportional hazard model were used for univariate and multivariate analysis. A total of 1,055 patients (71.4% male, 87.4% white, aged 46.7 years) were included: nadir and current CD4 cell counts were 203 cells/mm3 (106–292) and 554 cells/mm3 (413–713.5). HIV RNA was undetectable in 781 patients (74%), <20 copies/ml in 190 patients (18%) and 20–50 copies/ml in 84 patients (8%). Virological failure was observed in 81 patients (7.7%); at multivariate analysis detectable RNA at baseline (p=0.017), HCV infection (p=0.020), more than three pills in the regimen (p=0.003), and duration of HIV RNA <50 copies/ml below 2 years (p<0.001) were independently associated with virological failure. In 14 patients newly selected resistance-associated mutations were observed. Undetectable HIV RNA by real-time PCR is significantly associated with a lower 2-year risk of virological failure along with Ab HCV negativity, longer viral control, and lower pill burden. Studies investigating the management of residual viremia under antiretroviral treatment are warranted.
Introduction
H
Although the exact impact of vLLV in the long-term management of HIV is poorly understood, two aspects have been studied. Both the presence of low-level replication and the aforementioned associated factors have been linked to higher levels of immune activation, proinflammatory cytokines, and microbial translocation. 11 Moreover, the possible role of vLLV in predicting later virological rebounds has been investigated in a few heterogeneous studies 1,12 –18 : with one exception 18 all found that having higher levels of residual HIV RNA was associated with an increased risk of further virological rebound. In the first published study, 17 commercial real-time polymerase chain reaction (PCR) with a cut off of 48 copies/ml was used, but commercial assays with lower HIV RNA cut off values are currently available in the clinical setting.
Therefore, we investigated the determinants and the virological outcome of patients with very low-level viremia measured by a commercial assay with a limit of quantification of 20 copies/ml in the clinical setting.
The primary objective of this study was to evaluate the impact of very low-level viremia (HIV RNA below 50 copies/ml) on the 2-year risk of virological failure in HAART-effectively treated patients. Secondary objectives were the analysis of determinants of undetectable RNA at baseline and the evaluation of virological consequences after virological failure.
Materials and Methods
Study design
A retrospective analysis was performed on all patients followed at a large outpatient clinic in Italy (Unit of Infectious Diseases, Department of Medical Sciences, University of Torino, Ospedale Amedeo di Savoia, ASLTO2) presenting two consecutive HIV RNA below 50 copies/ml in the first part of 2010; the more recent one was considered as baseline viral load. Patients with at least 6 months of regular follow-up were included. This retrospective study was approved by the local Ethics Committee and written informed consent was obtained from patients currently in care. Data are routinely collected every 3 months and treatment switches were made according to clinicians' independent decision.
Virological analysis
HIV RNA was measured through the real time PCR assay CAP/CTM HIV-1 vs. 2.0 (CAP/CTM, Roche Molecular System, Branchburg, NJ, detection limit: 20 copies/ml of HIV-1 RNA). Patients' viremia levels were stratified according to three different intervals: undetectable RNA (“Target Not Detected”, TND), <20 copies/ml, and 20–50 copies/ml. The result of the HIV RNA measurement below 50 copies/ml was available to clinicians. The Genotypic Sensitivity Score (GSS) was calculated using cumulative genotypic resistance tests and through the Stanford algorithm. 19 GSS was considered equal to the number of administered antiretrovirals in patients with unavailable genotypic resistance tests and no history of virological failures.
Genotypic resistance testing was performed in all virological failures using the standard direct full-population sequencing from plasma samples ViroSeq HIV-1 genotyping (Abbott, IL). Briefly, after nucleic acid extraction with the semiautomatic NucliSENS easyMAG platform (BioMerieux, Marcy l'Etoile, France) from 1 ml of plasma, sequences of HIV-1 protease (P) and reverse transcriptase (RT) regions were constructed for each sample with seven different primers targeting the majority of HIV-1 P and RT genes. To enhance the sensitivity for samples with HIV-RNA <1000 copies/ml, the standard ViroSeq HIV-1 protocol was modified in that a nested PCR step was introduced. Three Amplicons generated from PCR were visualized on 1% agarose gel and sequenced on the ABI PRISM 3100 Genetic Analyzer (Applied Biosystems, Foster City, CA) according to the manufacturer's instructions.
20
Sequence data were assembled and analyzed with the ViroSeq HIV-1 Genotyping System software 2.7 for the identification of drug resistance mutations. The Stanford Drug Resistance Database (
Definition of failure
Virological failure was defined as two consecutive viral loads above 50 copies/ml (at least 7 days apart) or one value above 50 copies/ml in patients lost to follow-up.
Statistical analysis
Normally distributed variables were described with means (±standard deviation, SD) and analyzed with parametric testing while not normally distributed ones were described with medians (interquartile ranges, IQR) and analyzed with nonparametric tests. Kaplan–Meier analysis was used to estimate the cumulative incidence of virologic failure, stratified according to three different exposure statuses: TND, <20 copies/ml, and 20–50 copies/ml.
The impact of variables on the risk of virological failure was estimated through log-rank tests and the multivariate Cox proportional hazard model. This analysis was performed separately in patients who maintained the same regimen for the 2-year observation period (“nonswitchers”) as well as in all included patients: this was done with the aim of controlling for possible treatment switches guided by the presence of low-level HIV RNA. The association of determinants with undetectable baseline RNA was estimated through univariate tests (Chi-square, Mann–Whitney) and a multivariate binary logistic regression analysis. All multivariate models included variables with p values below 0.10 at univariate analysis and backward elimination (variables included in the model are detailed in the text). Data analysis was performed using SPSS software for Macintosh (version 20.0, IBM Corp.).
Results
Baseline characteristics
A total of 1,055 patients were included in the study: baseline demographic, immunovirological, and therapeutic characteristics are described in Table 1. Most of the patients were male (753, 71.4%), white (922, 87.4%), with a median age of 46.7 years (41.3–53.1); coinfection with HCV was present in 295 subjects (28%). The median durations of current antiretroviral treatment (ART) and of viral load suppression were 23.7 months (14–40.6) and 39.7 months (20.3–73.1), respectively; HIV RNA was constantly below 50 copies/ml for at least 2 years in 705 (66.8%) subjects. The current CD4 cell count was 554 cells/mm3 (413–713.5); 513 (48,6%) patients had a nadir below 200 CD4/mm3.
NRTI, nucleos(t)ide reverse transcriptase inhibitor; PI, protease inhibitor; NNRTI, nonnucleoside reverse transcriptase inhibitor; GSS, Genotypic Sensitivity Score.
Antiretroviral regimens were mostly (85.2%) based on the association of two NRTIs plus either a PI [433 patients, 41%: mostly atazanavir/ritonavir (220, 50.8%) followed by lopinavir/ritonavir (114, 26.3%) and darunavir/ritonavir (35, 8%)], an NNRTI [424 patients (40.2%), mostly efavirenz (238, 56.1%) and nevirapine (150, 35.4%)], or raltegravir (42 patients, 4%). Tenofovir disoproxil fumarate was the most commonly administered NRTI (751, 71.2%, in 706 patients coformulated with emtricitabine). Most of the patients were treatment experienced (940 patients, 89%): genotypic resistance tests were available for 371 subjects (35.1%) and they were used to obtain GSS scores [(≥3 in 815 patients (77.3%)].
Baseline viral strata and associated factors
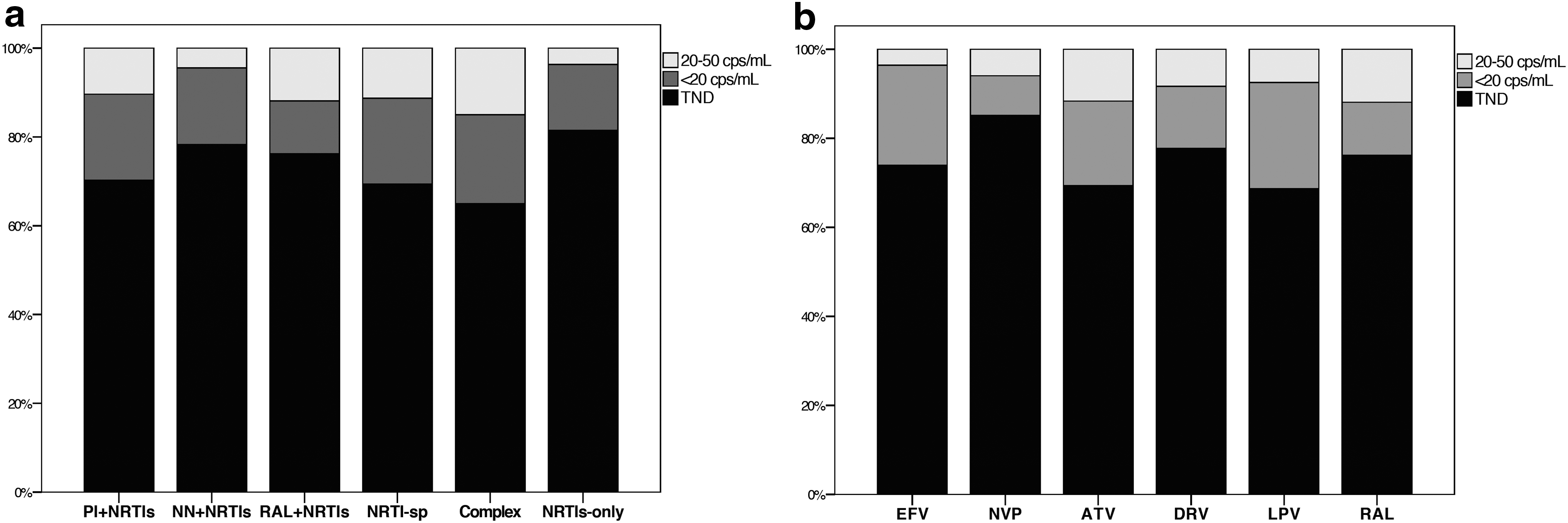
HIV RNA was undetectable in 781 patients (74%), below 20 copies/ml in 190 patients (18%), and between 20 and 50 copies/ml in 84 patients (8%).
The prevalence of baseline viral load strata according to antiretroviral regimen (all patients) and to third compound (in patients receiving two NRTIs plus a third drug, n=865) is depicted in Fig. 1a and b. Paired comparisons highlighted a significantly higher TND prevalence in patients receiving NRTIs-only or NN-based regimens as compared to PI recipients (p=0.007) but not to raltegravir recipients (p=0.75); nevirapine recipients showed the highest prevalence (85.1%). Using ANOVA tests several significant differences were noted among regimen groups as to CD4 cell count, CD4 cell nadir, duration of HIV infection, and duration of controlled viremia (for instance NNRTIs and NRTIs-only recipients had the highest duration of HIV RNA suppression).
At univariate analysis, variables associated with TND were age (for 10 years increase, p=0.049), female gender (p=0.003), nadir CD4 above 200 cells/mm3 (p=0.002), duration of viral suppression above 2 years (p=0.039), the use of ARV regimens consisting of less than four pills (p=0.03), and the use of NNRTIs or raltegravir (p=0.007).
At multivariate logistic regression analysis (including age, pill count, and NNRTI or raltegravir use) female gender (p=0.002, aOR 1.68, 95% CI 1.20–2.35), nadir CD4 cell count above 200/mm3 (p=0.002, aOR 1.56, 95% CI 1.18–2.08), and viral suppression above 2 years (p=0.026, aOR 1.40, 95% CI 1.04–1.89) were independently associated with TND.
Virological outcome and associated factors
After 24 months of follow-up, 102 patients were lost, but for 94 (92.2%) of them the last available viral load was below 50 copies/ml. A total of 860 subjects (81.5%) were still receiving the same baseline antiretroviral regimen (“nonswitchers”); reasons for treatment switches are available for a minority of subjects only. Virological failure was observed in 81 patients (7.7%) with a median HIV-RNA of 1,057 (98–25,552) copies/ml; HIV-RNA at failure was between 50 and 200 copies/ml or above 200 copies/ml in 31 and 50 patients, respectively. In the nonswitcher group 23 patients presented virological failure (11.8%); HIV-RNA was undetectable in 632 patients (59.9%), <20 copies/ml in 240 patients (22.7%), and 20–50 copies/ml in 182 patients (17.3%). The 2-year median CD4 cell count was 572 cells/mm3 (IQR 419–736).
At univariate analysis detectable RNA at baseline (p=0.003), female gender (p=0.043), hepatitis C virus (HCV) infection (p=0.004), GSS score below 3 (p=0.007), more than three pills (p<0.001), current use of PI-based regimens (p=0.002), and duration of viral suppression below 2 years (p<0.001) were associated with virological rebound. At multivariate analysis (including gender, GSS below 3, PI use) detectable RNA at baseline (p=0.017, aOR 1.71, 95% CI 1.10–2.68), HCV infection (p=0.020, aOR 1.69, 95% CI 1.08–2.62), more than three pills (p=0.003, aOR 1.97, 95% CI 1.26–3.06), and duration of viral suppression below 2 years (p<0.001, aOR 2.47, 95% CI 1.58–3.86) were independently associated with virological failure. Kaplan–Meier curves according to baseline factors are represented in Fig. 2a–d.

In nonswitchers the same variables were identified as independent predictors of virological failure: HCV infection (p=0.03, aOR 2.19, 95% CI 1.30–3.68), more than three pills (p=0.003, aOR 1.79, 95 IC 1.21–2.65), duration of viral suppression below 2 years (p<0.001, aOR 2.99, 95% CI 1.75–5.10), and detectable RNA at baseline (p=0.018, aOR 1.91, 95% CI 1.12–2.65).
We assigned an arbitrary score of 1 to the significant predictors of virological failure: a score from 0 to 4 was therefore calculated. Stratifying patients with low scores (0–1) and high scores (2–4) was significantly associated with the rate of virological failure during follow-up (log rank p<0.001) (Fig. 3a and b): the absolute risk of virological rebound was 4.5% vs. 13.7% in the low-risk and high-risk groups.

Virological outcome at rebound
Among 73 patients not lost to follow-up, 23 patients (31.5%) reported a self-performed treatment interruption (Table 2). In 37 (out of 50, 74%) adherent subjects in care at the end of follow-up genotype resistance testing was successful; median (and interquartile range) HIV RNA was slightly lower than in those with an unsuccessful genotype test [88 copies/ml (63–440) vs. 1497 copies/ml (76–5,112), Mann–Whitney p=0.10].

RAMs, resistance-associated mutations.
Fourteen patients (28%) selected new resistance-associated mutations. Characteristics both at baseline and at virological failure are summarized in Table 3: most of the newly selected mutations were in the reverse transcriptase gene (10/14) or in the integrase gene (four out of six raltegravir recipients). In two patients (out of two treated with maraviroc-containing regimens) a switch to X4-tropic viruses was observed.
Coformulated drugs are separated by slash (“/”); boosted protease inhibitors are defined by “/r.”
BL, baseline; RT, retrotranscriptase; RAMs, resistance-associated mutations; PI, protease inhibitors; INSTI, integrase strand transfer inhibitors; dd, days from baseline; TND, target not detected; TDF, tenofovir disoproxil fumarate; FTC, emtricitabine; RAL, raltegravir; ETV, etravirine; MVC, maraviroc; fAPV, fosamprenavir; AZT, zidovudine; 3TC, lamivudine; ABC, abacavir; DRV, darunavir; NVP, nevirapine; ATV, atazanavir; EFV, efavirenz; N.A., not available.
Discussion
Our retrospective analysis on a large sample of HIV-positive patients confirms that the undetectability of HIV RNA is associated with a lower risk of virological rebound in the following 2 years of follow-up as compared to the other two degrees of low-level viremia (less than 20 copies/ml and between 20 and 50 copies/ml). In addition to this virological marker a durable control of viral replication (above 2 years), the absence of HCV coinfection, and a limited number of pills may lower the risk of virological failures. Although seven papers have been published on the subject our research may add to the current knowledge the use of a low but commercially available threshold, the inclusion of patients on raltegravir-containing regimens, the analysis of other factors associated with outcome, and the characterization of resistance-associated mutations at failure. 1,12,14 –18
Some limitations should be highlighted: the retrospective design, the absence of a formal evaluation of adherence, and the already reported variability in HIV RNA quantification at low viremia. 21,22 However, the use of commercial assays with high sensitivity and a low limit of detection (20 copies/ml in this study) is widespread and the “target not detected” output (suggesting HIV RNA undetectability) may be relevant in the long-term management of HIV-positive patients.
The main objective of this study was to assess the impact of the level of viremia below 50 copies/ml on the risk of virological rebound after 2 years of follow-up: 7.7% of the included subjects had a confirmed elevation of plasma viral load. We observed that patients presenting a TND at baseline had the lowest incidence of viral rebound in follow-up. The observation that patients with the lowest residual viremia had the lowest risk of subsequent virological failures has already been reported in several studies. 1,12 –17 However, some differences are worthy of being mentioned. The study by Doyle et al. is the only one using the “target not detected” output and they showed that this was the group with the best virological outcome. 12 Furthermore, differences in follow-up (from 12 to 30 months), definition of low level viremia (persistent versus nonpersistent), different HIV RNA cut offs (50, 48, 40, 27, and 3 copies/ml), and methodological issues are noteworthy. 23 –25 The aforementioned technical differences may partially explain some of the observed differences in study outcomes: the CAP/CTM assay vs. 2.0 was associated with a better estimation of low-level viremia as compared to the Abbott Real Time assay. 22,26 Two reports were not concordant with these observations: one had a short follow-up and the extended study showed a roughly 4-fold risk of viral failure among patients with residual viremia. 15,16 The second study by Charpentier et al. using the CAP/CTM vs. 2.0 assay reported an association of persistent low-level viremia with a higher blip ratio but not on the risk of virological rebound. 18
Other factors have been identified as being independently associated with virological rebound: HCV coinfection, a short (less than 2 years) HIV RNA suppression, and the use of antiretroviral regimens containing more than three pills. Patients coinfected with HCV may have multiple comorbidities and polypharmacy, immune dysfunction, and possibly incomplete adherence to medications 27 ; however, a detrimental effect of HCV infection on the durability of HIV control has seldom being reported. 28 A prolonged control of HIV replication may be beneficial in decreasing reservoir size as well as immune activation and it has been suggested as one of the possible factors associated with virological rebound after switching to a boosted protease inhibitor regimen. 29 Despite the fact that residual viremia may persist even after 7 years of successful antiretroviral treatment, the risk of viral failure declines with the duration of suppression regardless of patients' adherence. 2
One critical issue would be measuring patients' adherence to medications and it has been recently reported 30 : even if this was not available in this study we used pill number as a surrogate marker for adherence, although previous studies showed mixed results. 31 It has been shown that higher degrees of compliance to medications are obtained in patients receiving easy regimens composed of few pills and possibly once a day: in this scenario the use of a single tablet regimen has been associated with optimal efficacy results as well as less hospitalization and mortality. 32 Regimens including four or more pills were associated with a higher risk of virological rebound. In addition to worse adherence to complex therapies other reasons might explain this finding since PI-containing regimens include at least three pills: they are associated with worse tolerability, less forgiveness (given their short half-lives), and are usually administered to patients harboring pretreated viruses. No difference in virological failure was observed between QD and BID treatments: despite discordant results a recent large randomized trial suggested that a twice-daily administered but excellently tolerated regimen was superior to once-daily PI-based combinations. 33
In the whole cohort newly selected mutations have been observed in 14 patients only (out of 50 patients with virological failure and successful viral genotype). The characteristics of the 14 patients losing future treatment options are described in Table 3 and they confirm the chance of selecting RAMs in patients treated with drugs with a low (NNRTIs or raltegravir) or undefined (maraviroc) genetic barrier to resistance. 34
Combining these factors into a simple score (arbitrarily assigning 1 point to each of these variables and also taking into account the similarities in adjusted odds ratio of the multivariate model) may provide a clinically useful model. Stratifying patients according to the presence of 0 or 1 factor (low risk) or 2 or more (high-risk) factors was associated with a significant ability to differentiate patients with a low or high chance of ensuing viral rebound (4.5% vs. 13.7%). Once confirmed in prospective independent cohorts this score may be relevant for allocating patients to less frequent monitoring or less drug regimens. 35
These data may suggest that the optimal target of antiretroviral treatment may be lowered (as happened in the past with the availability of more sensitive tests) to the achievement of undetectable RNA. Nevertheless the management of low-level viremia is currently unknown and it deserves prospective clinical studies. Intensification studies of conventional HAART to determine the contribution of ongoing viral replication to residual viremia have shown heterogeneous results: while Yukl et al. found a decrease of unspliced HIV RNA in the ileum (but not in plasma, PBMCs, duodenum, colon, or rectum), 36 other authors found no effect. 37 –46
It is noteworthy that none of these studies included the use of nevirapine: the drug has been associated with the lowest residual viremia in two studies 8,9 and with long-term control of HIV viremia in a dual therapy with raltegravir. 47 Despite some unfavorable characteristics (hepatotoxicity, skin rashes, low genetic barrier to resistance) that placed nevirapine among alternative regimens in international guidelines, favorable pharmacokinetic features and tolerability may support prospective switch studies using nevirapine-containing regimens.
One of the secondary objectives of this study was the analysis of the variables associated with HIV RNA undetectability (TND) using the Taqman 2.0 test: 74% of long-term efficaciously treated HIV-positive patients presented an undetectable HIV RNA. We found that female gender, high nadir CD4 cell count, and durable HIV RNA suppression were independently associated with TND. While gender differences have not been definitively demonstrated 48,49 both CD4 nadir and durable viral replication control have been associated with low reservoir size, less residual viremia, and less immune activation. 50 –52
At univariate analysis we also found that both NNRTI-based and raltegravir-based regimens had the highest prevalence of TND as compared to PI-based, NRTI-sparing, and complex regimens; surprisingly, 81.5% of patients taking three or four NRTIs (with no other antiretrovirals) had not detectable RNA. The groups of patients with different antiretroviral regimens showed significant differences in CD4 nadir and HIV RNA suppression and the treatment-related effect disappeared at the multivariate analysis: these baseline disparities as well as the inclusion of the number of pills (indirectly linked to patients' adherence to medication) may explain this observation. However, in patients under “conventional regimens,” i.e., those receiving two NRTIs plus a third drug, nevirapine and raltegravir recipients showed the highest rates of TND: while the favorable association between nevirapine use and low residual viremia has already been reported 8,9 such a raltegravir effect is a novel observation.
Raltegravir's mechanism of action, activity in macrophages, and very fast viral decay as well as the long-term excellent efficacy and tolerability may explain this finding. 53 The discovery of other possible reservoirs (such as CD4-associated) 54 –56 or lymph nodes 57 –59 remains essential for the goal of an HIV functional cure: the pharmacological properties of antiretroviral compounds may justify some of these observations (and favor drugs with a higher tissue distribution such as nevirapine). 23
In conclusion, having an undetectable RNA, more than 2 years of HIV RNA below 50 copies/ml, being HCV free, and being treated with less than four pills were associated with a lower 2-year risk of virological rebound in the following 2 years of follow-up. The majority (74%) of patients with confirmed HIV-1 RNA below 50 copies/ml present no detectable RNA using a 20 copies/ml commercially available real-time PCR assay. Female gender, nadir CD4 cell count above 200/mm3, and viral suppression above 2 years were independently associated with TND at baseline.
These data warrant further investigation in the context of the management of low-level viremia in HIV-positive treated patients.
Footnotes
Acknowledgments
This study was presented at the 14th European AIDS Conference (EACS), October 16–19, 2013, Brussels, Belgium, EU. PS7/4.
A.C., S.B., V.G., and G.D.P. contributed to the study design, data collection, interpretation of data, and statistical analysis. S.L.R. and I.M. contributed to data collection. A.C., S.B., V.G., and I.M. drafted the first version of the manuscript and finalized the manuscript. G.D.P. contributed to the study design, supervision, and critical revision of the manuscript for intellectual content. All authors read and approved the final manuscript.
This work was supported by internal funding. A. Calcagno and I. Motta contributed equally to this work.
Author Disclosure Statement
A.C. has received travel grants or speaker's honoraria from Abbott, Gilead, ViiV, Bristol-Myers Squibb (BMS), Merck Sharp & Dome (MSD), and Janssen-Cilag. S.B. has received grants, travel grants, and consultancy fees from Abbott, Boehringer-Inghelheim, BMS, Gilead-Sciences, GSK, MSD, Pfizer, and Janssen-Cilag. G.D.P. has received grants, travel grants, and consultancy fees from Abbott, Boehringer-Inghelheim, BMS, Gilead-Sciences, GSK, MSD, Pfizer, Roche, and Tibotec (Johnson & Johnson).