
Abstract

A 51-
In addition to lung cancer, her past medical history was notable for HIV. She had been living with HIV infection for over 10 years and had never taken antiretroviral therapy, except briefly while pregnant 8 years earlier. Previous HIV viral loads were always low level (<1,000 copies/ml) without antiretroviral therapy (ART), and the CD4 count remained high (>500 cells/mm3). The CD4 and viral load check at the time of cancer diagnosis were 560 cells/mm3 and 470 copies/ml, respectively. ART was not initiated at the time of the cancer diagnosis due to poor prognosis.
On arrival to the inpatient unit, the temperature was 36.4°C, pulse 106, blood pressure 125/85, respiratory rate 35, and pulse oximetry 90% on room air. The general examination was notable for intact mental status and mild distress. The oropharynx revealed new thrush. The cardiovascular evaluation confirmed tachycardia, with no murmurs, gallops, or rubs. The pulmonary examination was notable for tachypnea and decreased breath sounds in all lung fields, but no rhonchi or crackles. There was no peripheral edema. The neurologic examination was nonfocal.
Laboratory studies were notable for a white blood cell count of 13.7 with 37% segmented neutrophils, 55% bands, and 3% lymphocytes. The CD4 count and viral load were now 255 cells/mm3 (29%) and 460,000 copies/ml, respectively. A computed tomography (CT) scan of the chest showed extensive cavitary lesions in all five lobes, accompanied by panlobular tree-in-bud opacities, pneumomediastinum, a slight decrease in the primary right upper lobe mass, but progressive metastatic disease (Fig. 1). Empiric therapy was initiated with meropenem, levofloxacin, linezolid, and trimethoprim/sulfamethoxazole.
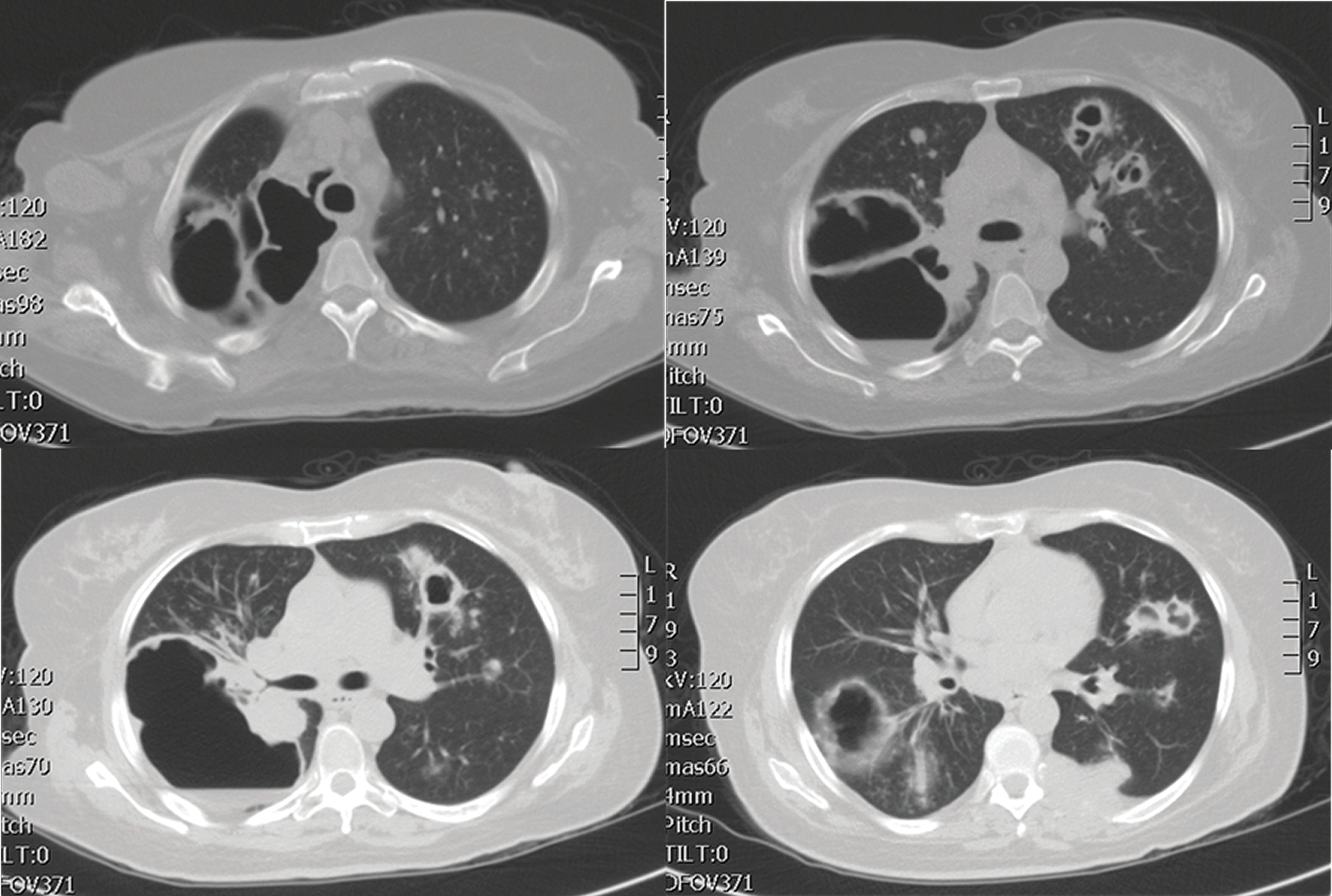
Representative images from the computed tomography (CT) scan of the thorax, demonstrating extensive cavitary lesions and tree-inbud opacities, new in comparison to a previous CT scan 3 months prior. Malignant masses are visible near the hilum on the left lower image and posteriorly on the right lower image.
Bronchoscopy demonstrated hyperemic airways with thick purulent secretions in the right upper lobe. On cytology, silver stain identified Pneumocystis jirovecii (data not shown). Therapy was optimized to trimethoprim-sulfamethoxazole and prednisone for Pneumocystis carinii pneumonia (PCP). ART with tenofovir/emtricitabine and dolutegravir were initiated for HIV on day 5.
The patient responded well to therapy and was discharged on day 7 on room air. By week 4 of ART, the viral load decreased to 430 copies/ml treatment. One month later she decided to return to hospice care due to progressive cancer.
Lung cancer is a devastating non-AIDS-defining cancer for patients with HIV infection. 1 However, chemotherapy can be beneficial and well tolerated; multiple studies have demonstrated preservation of virologic and immunologic control of HIV despite aggressive antineoplastic therapies when using ART. 2 However, studies from the pre-ART era document chemotherapy-induced loss of virologic control; for example, treatment with CHOP caused a 0.6–2 log increase in viral load in one cohort, while EPOCH caused a 0.86 log increase in another series. 3,4 ART initiation and prophylaxis for opportunistic infections may have protected the patient from severe PCP infection.
Footnotes
Author Disclosure Statement
No competing financial interests exist.