
Abstract
Chronic hepatitis C virus (HCV) infection is associated with lower serum concentration of low-density lipoprotein (LDL-C), the primary cholesterol metabolite targeted pharmaceutically to modulate cardiovascular risk. Chronic infection with human immunodeficiency virus (HIV) and treatment with antiretrovirals (ARVs) are associated with dyslipidemia and increased risk of cardiovascular disease. In subjects coinfected with HIV and HCV, lipid abnormalities associated with either infection alone are often attenuated. Treatment of chronic HCV infection in HIV/HCV-coinfected subjects is now possible with interferon (IFN)-free regimens composed of directly acting antivirals (DAAs). We previously observed a marked increase in serum LDL-C in HCV-monoinfected subjects treated with sofosbuvir and ribavirin (SOF/RBV) that correlated with viral decline in serum, suggesting a direct influence of HCV clearance on serum cholesterol. In the present study, we assessed longitudinal changes in cholesterol in HIV/HCV-coinfected subjects during treatment of HCV genotype-1 (GT1) infection with combination DAA therapy. We report a rapid increase in LDL-C and LDL particle size by week 2 of treatment that was sustained during and after treatment in HIV/HCV-coinfected subjects. No change in serum LDL-C was observed at day 3 of treatment, in spite of a marked reduction in serum HCV viral load, suggesting LDL-C increases do not directly reflect HCV clearance as measured in peripheral blood. After effective DAA therapy for HCV, an increase in LDL should be anticipated in HIV/HCV-coinfected subjects.
Introduction
C
With the advent of combination antiretroviral (ARV) therapy for HIV infection, mortality due to complications of AIDS has declined, while mortality associated with liver and cardiovascular disease has increased. 3,24 –26 Chronic HIV infection and treatment with ARVs are both associated with dyslipidemia, and cardiovascular risk is often modulated by the administration of LDL-lowering statin therapy. 1,2,4,27,28 Interestingly, the phenotypes of low LDL associated with HCV and hypercholesterolemia associated with HIV are often attenuated in the setting of HIV/HCV coinfection. 5 –8,10
Treatment of chronic HCV infection is now possible with interferon (IFN)-free regimens composed of directly acting antiviral (DAA) agents that directly inhibit viral proteins. 11 Marked advances in IFN-free DAA treatment of HCV infection in HIV/HCV-coinfected subjects have also been reported, 29,30 such that HCV disease will be increasingly eradicated in this population.
How lipid profiles are altered after sustained virologic response (SVR) is achieved with DAA therapy for HCV in HIV/HCV-coinfected patients is unknown. We recently observed a rapid and sustained increase in LDL concentration in HCV, GT1-monoinfected subjects treated for 24 weeks with SOF/RBV. 31 LDL changes were sustained posttreatment in subjects achieving SVR, while LDL declined to pretreatment levels in subjects who experienced treatment relapse. 31 In the present study, we preformed longitudinal lipid analyses in HIV/HCV-coinfected subjects who achieved SVR with combination DAA therapy and compared the findings to HCV-monoinfected subjects treated with similar regimens. 29,32
Materials and Methods
Study design
Clinical data and serum samples from 90 chronically infected, treatment-naive HCV GT-1 (n = 50 HIV/HCV-coinfected, n = 40 HCV-monoinfected) subjects were considered for analysis. All 90 subjects were enrolled in phase 2, single-center, prospective, community-based clinical trials that evaluated all-oral DAA treatment at the National Institute of Allergy and Infectious Diseases, National Institutes of Health in Bethesda, MD.
Fifty GT1, HCV treatment-naive HIV/HCV-coinfected subjects were treated on the NIH/NIAID ERADICATE (NCT01878799) protocol with the fixed dose combination of ledipasvir (LDV, 90 mg) combined with SOF (400 mg) once daily for 12 weeks. 29 Thirty-seven subjects were virally suppressed with ARVs while 13 subjects were not receiving ARVs. 29 Study approved ARVs included emtricitabine/tenofovir combined with efavirenz, raltegravir, or rilpivirine. Subjects not on ARVs had a stable CD4 T-lymphocyte count ≥500 cells/mm3 (n = 2) or a stable CD4 count with an HIV viral load <500 copies/ml at baseline (i.e., elite controllers, n = 11). Forty GT1, treatment-naive, HCV-monoinfected subjects were treated on the NIH/NIAID SYNERGY (NCT01805882) protocol with SOF/LDV combined with the investigational NS3/4A inhibitor GS-9451 (80 mg) or the allosteric NS5B inhibitor GS-9669 (500 mg) once daily for 6 weeks. 32 Data were analyzed only from subjects achieving SVR. All subjects provided written or oral informed consent approved by the NIAID/NIH Institutional Review Board, and the study protocols conformed to the ethical guidelines of the Declaration of Helsinki.
Serum cholesterol measurements
Measurements for total serum cholesterol content, cholesterol content of HDL (HDL-C) and LDL (LDL-C), and triglycerides were performed in the NIH Clinical Research Center laboratory on the day of collection. Subjects were not instructed to fast prior to blood draws. Subjects who recently started or had a dose modification of statin therapy during HCV treatment were excluded from analysis. Subjects on stably dosed, long-standing lipid-modulating drugs or metformin therapy for diabetes were included.
The Vantera Clinical Nuclear Magnetic Resonance (NMR) Analyzer was used to identify and quantify lipoprotein particle distribution and generate an NMR LipoProfile using stored patient serum, as previously described. 12,33 The NMR Analyzer detects specific lipoproteins by subjecting patient serum to radio frequency energy within a magnetic field, with determination of particle lipid composition by proprietary Vantera Clinical Analyzer software.
In HIV/HCV-coinfected subjects treated for 12 weeks, clinical serum lipids were measured pretreatment and at weeks 2, 4, 12 (end of treatment), and 24 (SVR12). Data are reported from 45 of 50 treated patients, with five patients excluded due to missing data, initiation of lipid modulating therapy during study, or relapse. Serum from a subset of 34 HIV/HCV-coinfected subjects (n = 22 on ARVs, n = 12 untreated) was selected for NMR LipoProfile analysis based on availability. NMR LipoProfile data were measured at baseline, day 3, week 2, and week 12. In HCV-monoinfected subjects treated for 6 weeks, clinical serum lipids were measured pretreatment and at weeks 4, 14 (SVR8), and 30 (SVR24). Three patients did not have week 30 data collected, and subsequent data collected at week 42 were used for analysis. Data are reported from 31 of 40 treated patients, with nine patients excluded for the aforementioned reasons.
Statistical analysis
Baseline demographics were compared using the Mann–Whitney test for continuous outcomes and Fisher's exact t-test for binary outcomes. Clinical serum lipids and NMR data were analyzed by ANOVA relative to pretreatment values with a multiple test correction. Prism 6.0 (GraphPad Software Inc., La Jolla, CA) was used for statistical analysis and data presentation. Subjects with a missing time point for select components of the LipoProfile analyses were not included.
Results
In these two phase 2 clinical trials, 88 out of 90 subjects (98%) achieved SVR with undetectable HCV RNA 12 weeks after treatment, and as such, analysis was restricted to subjects achieving SVR. 29,32 A summary of baseline patient demographics is shown in Table 1. One HIV/HCV-coinfected patient treated with SOF/LDV for 12 weeks and one HCV-monoinfected patient treated with SOF/LDV/GS-9669 for 6 weeks relapsed within 4 weeks of completing treatment.
Steatosis was graded on liver biopsy only where available (n = 81/83).
Two Eradicate patients were classified as genotype 1 without a subtype.
Continuous variables are shown as median (with interquartile range, IQR) with analysis by the Mann–Whitney test or mean (with standard deviation, SD) with analysis by unpaired t-test. Categorical variables are expressed as number of patients (no.) with frequencies (%), with analysis by the Fisher's exact t-test. Race was self-reported. Body mass index is the weight in kilograms divided by the height in meters. Advanced liver disease (HAI-fibrosis 3–4) was determined by pretreatment biopsy (n = 83) or Fibrosure (n = 8) IFNL4 genotype was determined using the rs368234815 dinucleotide variant.
HVC, hepatitis C virus.
In HIV/HCV-coinfected subjects treated with SOF/LDV for 12 weeks, total serum cholesterol content increased by week 2 of treatment (153 ± 5 to 182 ± 6 mg/dl, p < 0.0001), the first on-treatment time point assessed, a change sustained during therapy at week 4 (189 ± 5 mg/dl, p < 0.0001), week 12 (end-of-treatment) (177 ± 5 mg/dl, p < 0.0001), and week 24 (174 ± 5 mg/dl, p < 0.0001) (Fig. 1A). Serum LDL-C also increased by week 2 of treatment (82 ± 5 to 108 ± 5 mg/dl, p < 0.0001), a change sustained through week 4 (113 ± 5 mg/dl, p < 0.0001), week 12 (105 ± 5 mg/dl, p < 0.0001), and week 24 (101 ± 5 mg/dl, p < 0.0001) (Fig. 1B). HDL-C increased only slightly at week 4 (47 ± 3 to 52 ± 3 mg/dl, p = 0.0013) and week 24 (52 ± 3 mg/dl, p = 0.043) (Fig. 1C), while there was no significant change in triglyceride concentration (Fig. 1D). No differences in lipid measurements at baseline or during treatment were observed between subjects treated or untreated with ARVs, and the results did not change significantly when patients on stable lipid-modulating therapy were excluded (data not shown).
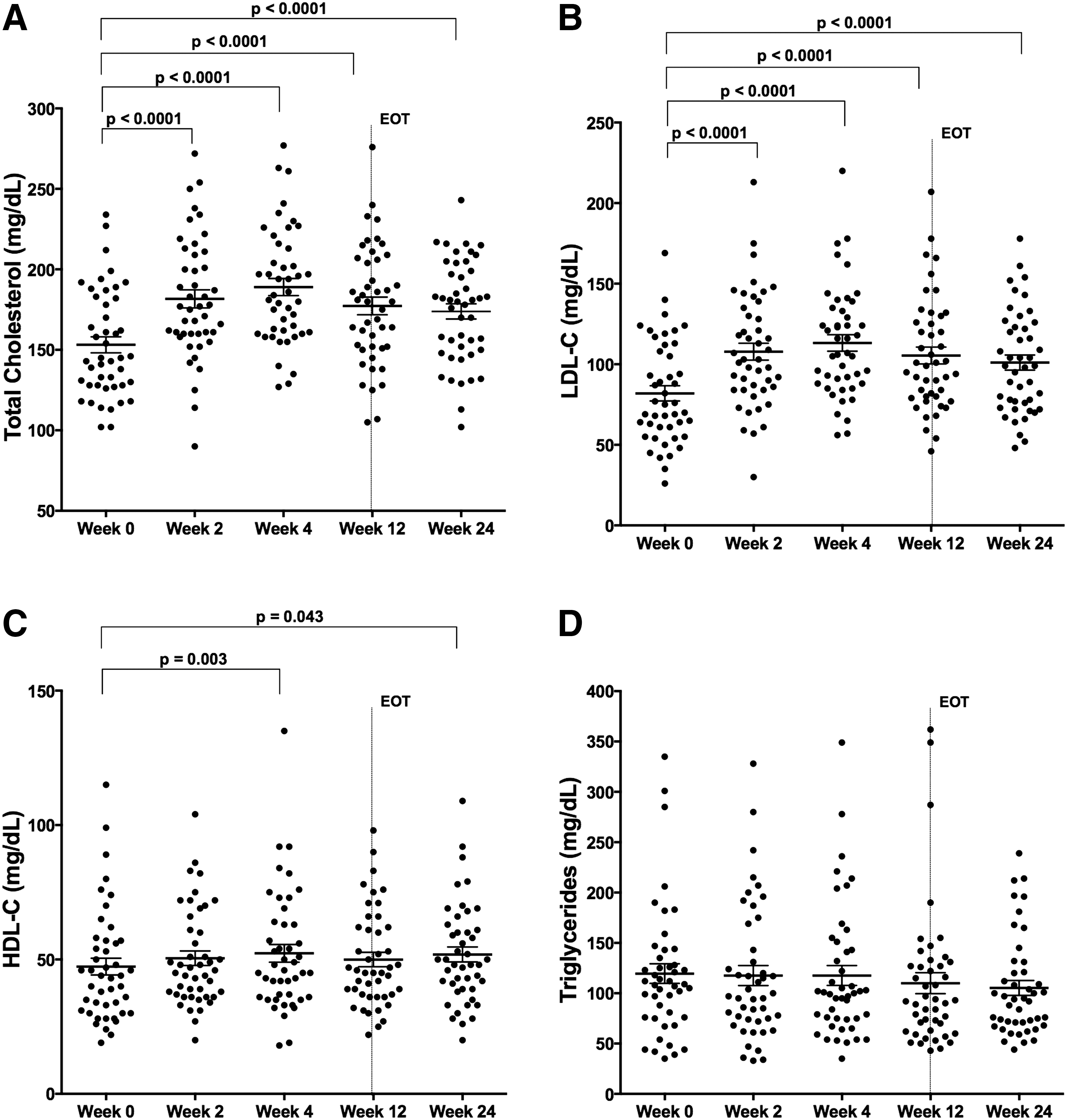
Low-density lipoprotein (LDL)-C cholesterol concentration increases on therapy in HIV/hepatitis C virus (HCV)-coinfected subjects. Total cholesterol and serum LDL-C concentrations change on HCV therapy with sofosbuvir/ledipasvir (SOF/LDV) for 12 weeks in HIV/HCV-coinfected subjects
As noted in these and most DAA trials, there is a precipitous drop in HCV serum viral load with initiation of DAA therapy. 32 In representative studies, baseline HCV RNA ranging from 6.2 to 6.8 log10 IU/ml dropped to <25 IU/ml by week 2 of treatment in 81–93% of subjects. 34 –36 HCV circulates in lipoviral particles, and clearance of HCV could directly impact cholesterol levels and account for the observed changes in Fig. 1. To assess the relationship between serum LDL changes and viral load decline, an in depth NMR LipoProfile analysis was performed on serum from 34 HIV/HCV-coinfected subjects early in therapy on pretreatment, day 3, week 2, and week 12 samples to enumerate LDL particle size and number. Interestingly, LDL particle size (LDL-Z) did not significantly change early in therapy at day 3 (21.0 ± 0.13 to 21.0 ± 0.13 nm, p = 0.96) but had changed notably by week 2 (21.3 ± 0.13 nm, p = 0.0002), a change sustained through week 12 (21.3 ± 0.12 nm, p = 0.0006) and accounted for by an increase in large LDL particle count (LDL-P) (Fig. 2A and B). In contrast, early changes in particle size of VLDL (VLDL-Z) and HDL (HDL-Z) were not observed, other than a marginal reduction in VLDL-Z by week 12 of therapy with no change in particle count (HDL-P and VLDL-P) (Fig. 2C–F). While viral load had dropped >3.5 log10 IU/ml by day 3 (5.89 ± 0.14 to 2.33 ± 0.15 log10 IU/ml, p < 0.0001), there was no significant difference from baseline in serum LDL-C (90.2 ± 5.3 to 90.8 ± 5.8 mg/dl, p = 0.99) (Fig. 3), indicating that the changes in serum LDL-C do not directly correlate with peripheral HCV clearance measured in serum.
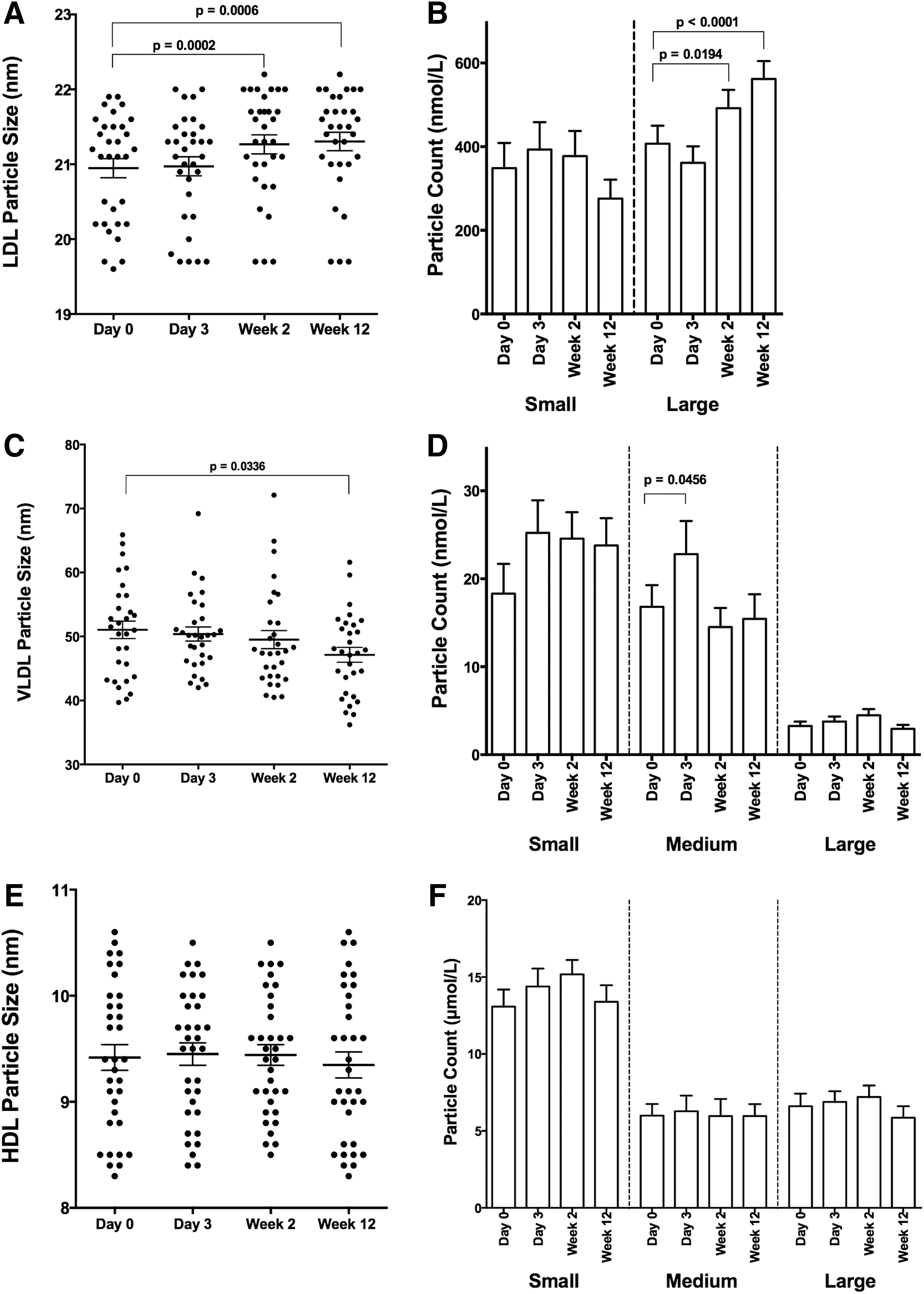
LDL-Z and VLDL-Z change dynamically on therapy in HIV/HCV-coinfected subjects. Serum from 34 HIV/HCV-coinfected subjects achieving sustained virologic response (SVR) was analyzed using NMR LipoProfile. Particle size and count for LDL

Increase in serum LDL-C lags behind treatment-induced HCV viral decline. Viral load and LDL-C concentration from 34 HIV/HCV-coinfected subjects treated with 12 weeks of ledipasvir and sofosbuvir HCV therapy. Shown are means and standard errors. LLOQ, lower limit of quantitation using the Abbott Real-Time HCV Assay.
To compare changes in HCV-monoinfected subjects treated with similar IFN-free, RBV-free combination DAA therapy, we measured longitudinal cholesterol levels in subjects treated with SOF/LDV combined with GS-9451 or GS-9669 for 6 weeks. 32 No differences in baseline lipid parameters were observed relative to the HIV/HCV-coinfected cohort (Table 1). Similar to HIV/HCV-coinfected subjects, in HCV-monoinfected subjects total serum cholesterol content increased by week 4 of treatment (156 ± 8 to 182 ± 8 mg/dl, p < 0.0001), the first on-treatment time point assessed in this trial (Fig. 4A). This increase was sustained posttreatment at week 14 (SVR8) (172 ± 6 mg/dl, p = 0.039) and week 30 (172 ± 7 mg/dl, p = 0.026) (Fig. 4A). Serum LDL-C also increased by week 4 of treatment (82 ± 7 to 111 ± 7 mg/dl, p < 0.0001), which was sustained posttreatment at week 14 (100 ± 5 mg/dl, p = 0.01) and week 30 (95 ± 6 mg/dl, p = 0.07) (Fig. 4B). No significant changes in HDL-C or triglyceride concentration were observed (Fig. 4C and D).
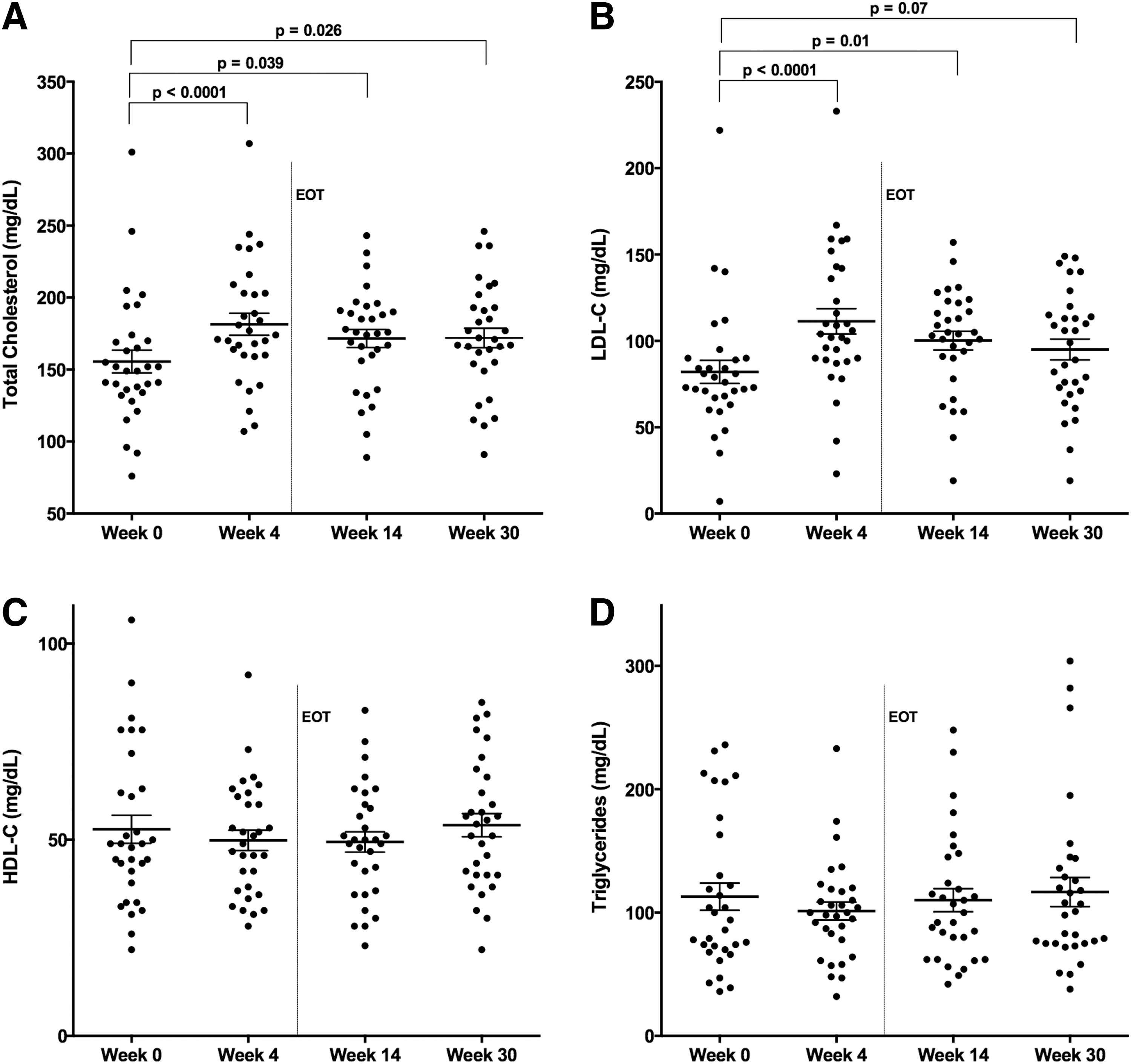
LDL-C cholesterol concentration increases on therapy in HCV-monoinfected subjects. Total cholesterol and serum LDL-C concentrations change during HCV therapy with SOF/LDV combined with GS-9541 or GS-9669 for 6 weeks in HCV-monoinfected subjects
Discussion
In this study, we observed a rapid and sustained increase in serum LDL-C in HCV-monoinfected and HIV/HCV-coinfected patients during and following successful treatment of HCV infection with IFN-free DAA therapy. The increase in serum LDL-C during HCV therapy was independent of the type of HCV therapy, and is likely reflective of the host's response to HCV suppression. These findings are consistent with increases in cholesterol observed during IFN-free treatment of HCV-monoinfected individuals, 12 and suggest that HIV coinfection does not substantially modulate the HCV-induced perturbation in serum cholesterol and the host response to HCV clearance. As HCV is eradicated with increasing frequency in HIV/HCV-coinfected subjects, these findings are significant in a climate where serum LDL is commonly used to prognosticate and pharmaceutically modulate cardiovascular risk.
The consistent observation that chronic HCV infection is associated with reduced serum LDL concentrations but increased cardiovascular risk reflects a distinction from traditional use of serum LDL for cardiovascular risk assessment. 15,16,37 The relative impact of the observed increase in LDL concentration associated with HCV clearance, shown here and in other studies, with the decrease observed in other biomarkers of cardiovascular disease observed with HCV clearance on subsequent risk for cardiovascular events requires prospective evaluation. 38
We also demonstrate that an LDL increase occurs with slower kinetics than the decline in HCV viral load in serum during treatment (Fig. 3), suggesting cholesterol changes are not directly due to clearance of lipoviral particles containing HCV. Interestingly, a recent study examining viral kinetics in serum and liver during treatment with telaprevir/IFN/RBV revealed a slower HCV RNA decline in the liver compared to plasma. 39 Given the estimated 7-day half-life of infected hepatocytes, 40 a persistent burden of intrahepatic HCV is likely still present at day 3 of treatment in this trial, but has likely declined significantly by week 2. Thus, changes in serum LDL-C may be a reflection of intrahepatic HCV burden and direct intracellular viral modulation of cholesterol metabolism. This difference could also reflect a delay in intrahepatic lipid biosynthesis and/or exocytosis relative to suppression of HCV replication.
One limitation of this study is that fasting was not requested prior to serum blood draws, which could result in variability in lipid measurements, in particular triglyceride and VLDL-C concentrations, known to be more affected by nonfasting. 41 In addition, the durability of the observed changes in lipids should be assessed prospectively posttreatment, as cholesterol values could change over time as the host reestablishes metabolic homeostasis in the absence of HCV.
In conclusion, there is a sustained increase in LDL-C levels in patients who achieve SVR with DAA therapy irrespective of HIV coinfection. Whether HCV clearance and changes in LDL will impact the higher rates of cardiovascular events associated with chronic HCV infection, and observed in some studies of HIV/HCV-coinfected relative to HIV-monoinfected subjects, will require prospective study in large patient cohorts. 16,37 In HIV-infected subjects receiving IFN-free treatment for HCV, lipids should be monitored posttreatment for cardiovascular risk assessment and determining indications for lipid-modulating therapy.
Footnotes
Acknowledgments
This study was funded by the Intramural Research Programs of the National Institute of Allergy and Infectious Diseases, the Critical Care Medicine Department, and the Clinical Research Center of the National Institutes of Health.
Data were presented in part at the HIV and Liver Disease Meeting, Jackson Hole, Wyoming, September 18–20, 2014.
Author Disclosure Statement
Anu Osinusi is an employee of Gilead Sciences. For all other authors no competing financial interests exist.