
Abstract
Heightened inflammation and immune activation are associated with lower bone mineral density (BMD) and lean body mass (LBM) among HIV-infected persons. We hypothesized that a reduction in inflammation with rosuvastatin would be associated with improvements in BMD and LBM. HIV-infected participants on stable antiretroviral therapy without statin indication and with heightened immune activation (≥19% CD8+CD38+HLA-DR+ T cells) or inflammation (hsCRP ≥2 mg/liter) were randomized to rosuvastatin 10 mg daily or placebo for 96 weeks. Among 72 participants randomized to rosuvastatin and 75 to placebo, there were no significant differences in the relative changes in BMD (p > 0.29) or in fat (p ≥ 0.19). A trend toward increased LBM (p = 0.059) was seen in the rosuvastatin arm without differences in creatinine kinase or self-reported physical activity (p ≥ 0.10). In a multivariable regression model, rosuvastatin was associated with a significant positive effect on LBM after adjusting for age, sex, race, smoking status, and detectable HIV-1 viral load. Higher baseline sCD163 correlated with increases in LBM from weeks 0 to 96 (p = 0.023); greater changes in total and leg lean mass were seen among statin users with higher compared to lower baseline IP-10 levels (LBM 1.8 vs. −0.3%; p = 0.028 and leg lean mass 2.9 vs. −1.7%; p = 0.012). Rosuvastatin is associated with an absence of toxicity on BMD and a potential benefit on LBM over 96 weeks of therapy. The preservation of LBM in the rosuvastatin arm over the 2 years of the study is of major clinical relevance in delaying loss of muscle mass with aging.
Introduction
D
Materials and Methods
Study design and participants
The SATURN-HIV (Stopping Atherosclerosis and Treating Unhealthy bone with RosuvastatiN in HIV) study is a randomized, double-blinded, placebo-controlled trial designed to measure the impact of daily rosuvastatin at 10 mg on cardiovascular disease and skeletal health, as previously described. 5,13 –15 This report details the results of the completed BMD, fat, and LBM changes from baseline to week 96. Enrollment occurred between March 2011 and August 2012. Eligible participants were HIV-infected adults ≥18 years of age with a fasting low-density lipoprotein (LDL) cholesterol of ≤3.37 mmol/liter (130 mg/dl) and either a high sensitivity C-reactive protein (hsCRP) level of ≥19.05 nmol/liter (2 mg/liter) and/or ≥19% activated CD8+ T cells (CD8+CD38+HLA-DR+). Additional eligibility criteria included receipt of stable ART for ≥12 weeks with cumulative ART duration of ≥6 months, HIV-1 RNA ≤1,000 copies/ml, and no history of fragility fractures. Participants were excluded for an active or chronic inflammatory condition (besides HIV), prior myocardial infarction, pregnancy/lactation, receipt of systemic chemotherapy or steroids, diabetes mellitus or uncontrolled thyroid disease, or use of anabolic agents, growth hormone, >81 mg aspirin daily, bisphosphonates, or teriparatide. Supplements including vitamin D were permitted, but participants were instructed not to change supplement doses or frequency. The study is registered on clinicaltrials.gov (NCT01218802) and was approved by the Institutional Review Board of University Hospitals Case Medical Center (Cleveland, OH). Written informed consent was provided by all participants.
Clinical assessments
Demographics and medical and HIV treatment history were obtained by self-report and confirmed by medical records. The targeted physical examination included height and weight measurements; body mass index (BMI) was calculated as kg/m2. Blood samples were collected after a 12-h fasting period. Minutes per 2 weeks of physical activity was collected by the AIDS Clinical Trials Group Physical Activity Assessment. 16
Dual-energy X-ray absorptiometry
Dual-energy X-ray absorptiometry (DXA) of the whole body, lumbar spine (L1–4), and left hip was performed in an anteroposterior view using the Lunar Prodigy Advance machine (GE Healthcare, Madison, WI). Peripheral fat depot (limb fat) and central fat depots (trunk fat) from whole body DXA were used in the analysis. Total LBM was defined as fat-free, bone-free mass as measured by DXA, with leg LBM that in the lower extremities only. Technicians used the same machine on the same subject throughout the study. DXA scans were read at Case Medical Center by an experienced radiologist blinded to study information. Osteopenia was defined by a t-score ≤ −1 and osteoporosis by a t-score ≤ −2.5 at either the total hip or lumbar spine. 17
Measurement of soluble markers in plasma and serum
Concentrations of interleukin-6 (IL-6), interferon gamma-inducible protein 10 (IP-10 or CXCL10), soluble tumor necrosis factor receptor (sTNFR)-1 and 2, soluble vascular cell adhesion molecule-1 (sVCAM), and intracellular adhesion molecule-1 (sICAM) were determined by quantitative sandwich ELISAs (R&D Systems, Minneapolis, MN). Plasma lipoprotein-associated phospholipase A2 (Lp-PLA2) concentrations were measured with an ELISA (PLAC Test; diaDexus, South San Francisco, CA). Hs-CRP concentration was determined by particle enhanced immunonepholometric assays on a BNII nephelometer (Siemens, Munich, Germany). Serum levels of soluble (s) CD14 and sCD163 were measured as markers of monocyte immune activation using Quantikine ELISA kits (R&D Systems). The interassay and intraassay coefficients of variance were <5% and <9%, respectively.
Statistical analysis
This was a prespecified, preplanned analysis to assess changes from baseline to 96 weeks in BMD, fat, and LBM and was powered accordingly for change in spine BMD. Continuous measures were described by medians and interquartile ranges and nominal variables with frequencies and percentages. Nominal variables were compared using χ2 analysis or Fisher's exact test. For between-group and within-group comparisons (at baseline and baseline to 48 week changes), normally distributed variables were compared using the t test or paired t test, respectively; nonnormally distributed variables were compared using the Wilcoxon rank-sum test or the signed-rank test, respectively. Correlations were assessed using Spearman's nonparametric rho. A multivariable linear regression model including age, sex, race, smoking status, and HIV-1 RNA above/below the limit of detection was constructed to examine the effect of covariates on the association between statin and relative LBM change. No adjustments were made for multiple analyses. Analyses were performed with SAS version 9.2 and 9.4 (SAS Institute, Cary, NC).
Results
One-hundred and forty-seven HIV-infected persons enrolled and were assigned to receive rosuvastatin (72 participants) or placebo (75 participants). The median age was 47 years, the median BMI was 26.7 kg/m2, and the majority of participants were male, African American, smokers, and taking tenofovir-containing ART regimens. The treatment and placebo groups were similar in demographic and clinical characteristics (all p ≥ 0.18; Table 1).
Values presented as median (25th, 75th percentile) or number (%).
Twenty-eight participants withdrew prior to the week 96 analysis, including nine in the rosuvastatin arm and 19 in the placebo arm. Eleven subjects were lost to follow-up; two moved from the area and two were incarcerated: these participants could not be evaluated for safety evaluations. Participants who withdrew or were lost to follow-up were more likely to be female (p = 0.013); other baseline characteristics were not significantly different. Twenty (71%) were smokers and 23 (82%) were taking tenofovir-containing ART regimens. Three cases of myalgias without rhabdomyolysis (two placebo, one rosuvastatin) were reported within the first 48 weeks 12 ; no further cases occurred between week 48 and 96.
Relative changes in BMD from baseline to week 96 were not significantly different between the rosuvastatin and placebo arms at any site including total hip (p = 0.52), femoral neck (p = 0.68), trochanter (p = 0.29), or lumbar spine BMD (p = 0.89; Fig. 1A). Total body, trunk, and limb fat increased in both the rosuvastatin and placebo arm from weeks 0 to 96; these changes were not significantly different between groups (p = 0.28, 0.19, and 0.41, respectively; Fig. 1B).
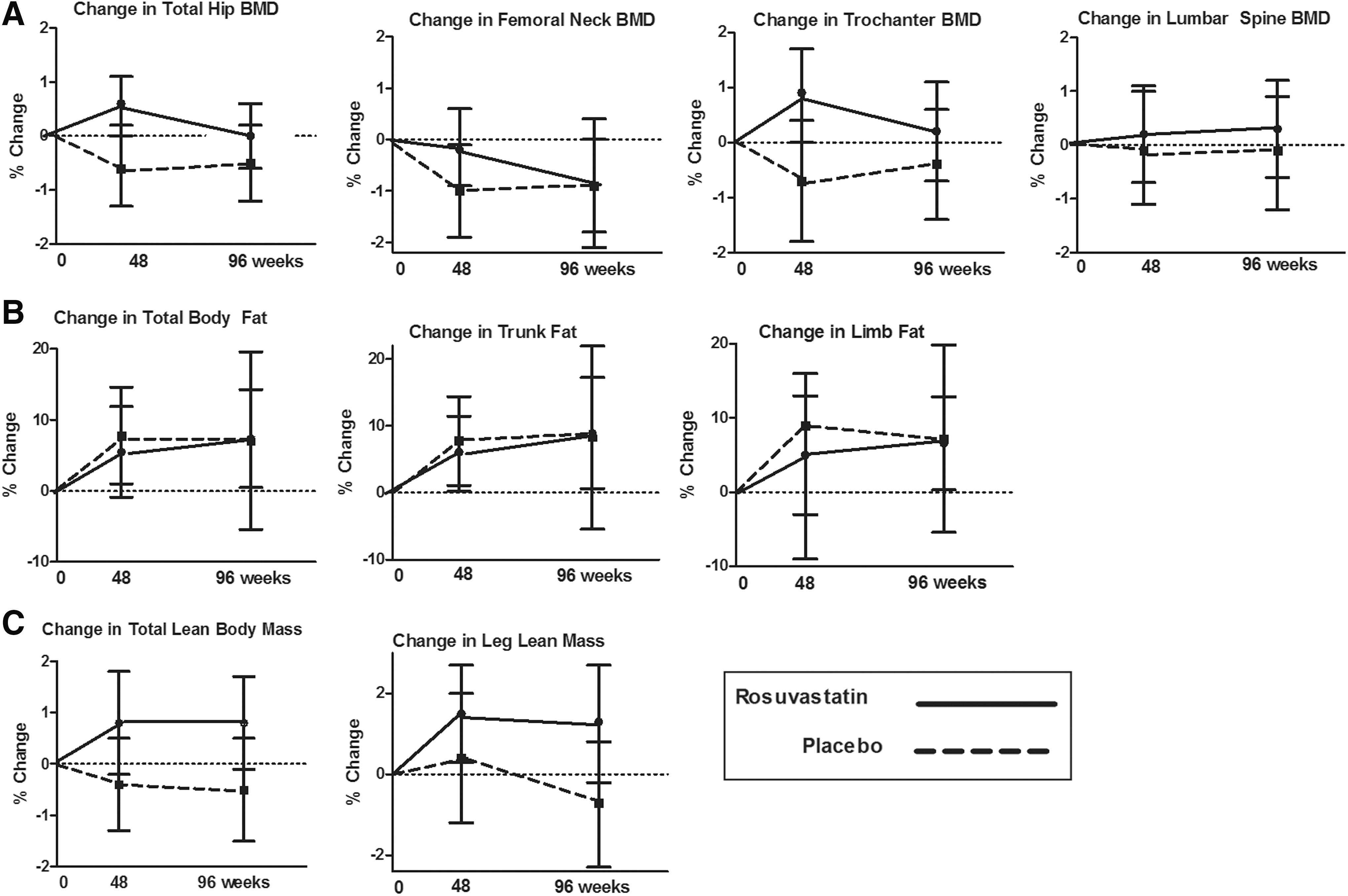
Relative changes in bone mineral density (BMD) and the total hip, femoral neck, trochanter, and lumbar spine
The mean LBM increased by 0.8% (95% CI 0.5, 0.9%; p = 0.091) in the rosuvastatin arm and decreased slightly in the placebo arm (−0.5%; −1.5, 0.5%; p = 0.35); differences between arms did not reach statistical significance (p = 0.059; Fig. 1C). Changes in leg LBM were also not significantly different between groups (p = 0.12; Fig. 1C). No significant correlation was detected between changes in weeks 48 or 96 leg LBM and changes in total hip BMD (all r ≤ 0.11, all p ≥ 0.26). CPK increased by 23.5% (−8.5, 55.6%; p = 0.15) in the rosuvastatin arm compared to 11.9% (−3.4, 27.3%; p = 0.15) in the placebo arm; between-group differences were not significant (p = 0.91). Both the rosuvastatin (187.1%; 152.4, 218.0%) and placebo (248.2%; 135.5, 360.8%) arms had significant increases in self-reported physical activity (p = 0.017 and <0.0001, respectively), but no significant difference was observed between groups (p = 0.10).
The effects of rosuvastatin on 96 week LBM changes were further investigated in a multivariable linear regression model including age, sex, race, smoking status, and detectable HIV-1 viral load. As shown in Table 2, rosuvastatin was associated with a significant gain in LBM (p = 0.026) and African American race was associated with a loss in LBM (p = 0.014).
Lastly, we explored whether the change in LBM was explained by the baseline levels of inflammation and immune activation. Higher baseline levels of sCD163 and a trend toward higher baseline sTNFR-1 correlated with increases in LBM from weeks 0 to 96 (r = 0.21; p = 0.023 and r = 0.16; p = 0.089, respectively) (Table 3). When restricted only to the statin arm, significantly greater changes in total LBM (1.8%; 0.6, 3.0%; p = 0.028) and leg lean mass (2.9%; 0.7, 5.1%; p = 0.012) were seen among participants with higher baseline IP-10 levels (above the median) compared to lower levels (LBM −0.3%; −1.7%, 1.1% and leg mass −0.3%; −2.2, 1.5%).
IL-6, interleukin 6; Lp-PLA2, plasma lipoprotein-associated phospholipase A2; IP-10, interferon gamma-inducible protein 10; sTNFR, soluble tumor necrosis factor receptor; sVCAM, soluble vascular cell adhesion molecule; sICAM, soluble intracellular cell adhesion molecule; hsCRP, high sensitivity C-reactive protein.
Discussion
Here, we present the final results from a 96-week randomized placebo-controlled trial of rosuvastatin to assess its impact on BMD, fat, and LBM among treated HIV-infected adults with normal LDL cholesterol and increased levels of inflammation or immune activation. In contrast to the small, but significantly greater BMD at the hip and trochanter that we previously reported after 48 weeks, 7 the BMD in the rosuvastatin arm trended back toward baseline between weeks 48 and 96, and differences were no longer significant between study arms by week 96. Outside of a trend for increased LBM in the rosuvastatin arm, we were unable to detect significant differences in peripheral or central fat, CK, or physical activity between rosuvastatin and placebo.
On first glance, the results are disappointing. When considering the detrimental reported effects of statins, including myalgias and rhabdomyolysis, cognitive impairment, aminotransferase elevations, and insulin resistance, 12,18 however, our results provide reassurance that rosuvastatin did not appear to exacerbate the impairments in BMD, fat distribution, or LBM in HIV-infected persons. Despite the negative BMD results, a few findings are noteworthy. First, the initial increase in BMD at 48 weeks and then stabilization or decline suggests a mechanistic pathway through inflammation and immune activation, as it mirrored the initial decline and then stabilization in several inflammation and immune activation markers. 12,19
Second is the association between rosuvastatin and increased 96-week LBM. A recent qualitative review of 25 longitudinal, observation studies of middle-aged to older, HIV-uninfected adults reported a median LBM loss of 0.5% per year in men and 0.4% per year in women 20 ; similar, aged-expected declines were observed in our placebo arm. Although the differences between rosuvastatin and placebo did not reach clinical significance, rosuvastatin was a significant predictor of LBM decline after adjusting for covariates in the multivariable model; the preservation of LBM in the rosuvastatin arm over the 2 years of the study could be of major clinical relevance in delaying loss of muscle mass with aging.
As has been shown in the Health, Aging, and Body Composition study, among older, HIV-uninfected adults, the loss of strength was approximately three times that of the loss in muscle mass. 21 As heightened inflammation is a strong predictor for the loss of muscle mass and muscle function, 22 those with the greatest inflammation prior to statin would presumably benefit the most. Indeed, participants in the rosuvastatin arm with the highest IP-10 at baseline had the greatest increase in LBM while on therapy. IP-10 is a Th1 chemokine with a pivotal role in inflammatory muscle diseases; IP-10 secretion is induced by tumor necrosis factor (TNF)-α, and further exaggerated by IL-6, both key cytokines in the regulation of muscle mass and function. 23
Two rodent studies utilizing a cancer 24 or motor neuron disease model 25 provide support for the relationship between inflammation and LBM response to statins: compared to placebo, simvastatin and atorvastatin, respectively, were associated with an increase in total body weight, muscle weight, and muscle fiber diameter among diseased rodents; no statin-related changes were seen among healthy rodents. In older adults, statin use was associated with less decline in lower extremity strength among the oldest women in the Women's Health Initiative, 10 better chair rise performance among statin-using older veterans, 26 and less impairment in gait speed or on a standard performance battery among statin users with peripheral artery disease. 11,27 Even among relatively healthy older adults, statin use was associated with improved lower-extremity blood flow 28 and greater gain in lean body mass with initiation of resistance exercise training. 29 Although we did not obtain an objective measure of muscle function, the changes in LBM suggest that rosuvastatin has a positive effect on muscle function. Whether the effect would continue over the often long-term duration of statin therapy remains clinically important but an unanswered question.
In routine clinical practice and in randomized studies, statins are more often recognized for deleterious effects on muscle, with reported myalgia or weakness occurring in approximately 5–15% of patients, and resulting rarely in rhabdomyolysis. 30 Outside of the occurrence of myopathy, however, the effects on muscle mass and physical function are less clear. A large (N = 420) randomized, placebo-controlled trial of high-dose atorvastatin was associated with muscle complaints and decreased physical activity, but no objective change in strength or performance. 31,32 In contrast, some observational studies have found lower strength, 33 lean mass, 33,34 and self-reported or objectively measured physical activity 35 among statin users compared to nonusers. A small (N = 37) randomized, but nonblinded trial of overweight or obese adults randomized to exercise training with or without high-dose simvastatin demonstrated a blunted improvement in cardiovascular fitness and skeletal muscle citrate synthase activity, a marker of mitochondrial content, but greater gain in LBM among the participants randomized to high-dose simvastatin with exercise training versus exercise training alone. 36 Rosuvastatin was well-tolerated in our study, with similar complaints of myalgias between the rosuvastatin (n = 1) and placebo (n = 2) arms. The muscle safety of rosuvastatin in our study was further substantiated by the lack of statistically significant differences in CK or self-reported physical activity between study arms.
Our study is relatively small and limited in generalizability. First, the effects of different statins can differ considerably, thus our results should be considered specific for rosuvastatin and may not be generalizable to other statins. The majority of participants were less than 50 years of age, male, African American, on stable ART, and with a healthier phenotype (without diabetes, and with normal BMD and normal LDL cholesterol), which may have underestimated the effect of statins. Similarly, some inflammatory markers may be higher in women, and the correlations between inflammation and LBM may have been, in part, confounded by sex. However, the double-blinded, randomized assignment to rosuvastatin therapy, eliminating the prescribing bias found in observational studies of statins, and the study duration of nearly 2 years are clear strengths.
In summary, the absence of toxicity on BMD and the potential benefit of rosuvastatin on LBM after 96 weeks of therapy provide some reassurance as to the safety, as well as potential mechanistic insight into the preservation of LBM in an inflammatory state. The heightened risk of cardiovascular disease and cardiovascular disease-related deaths in HIV-infected persons despite effective ART has led to growing interest in developing strategies to prevent cardiovascular disease. A comprehensive understanding of statin risks, including insulin resistance as previously shown in SATURN-HIV, 12 and potential cardiovascular and noncardiovascular benefits, including effects on muscle, will inform treatment decisions in HIV, particularly when determining the role of statins in primary prevention.
Footnotes
Acknowledgments
Results of this study were presented in part at the Conference on Retroviruses and Opportunistic Infections 2015, Seattle, WA. This project was supported by the National Institutes of Health [NR012642 to G.A.M. and K23 AG050260 to K.M.E.]. Technical support was provided by the Center for AIDS Research, Case Western Reserve University (P30 AI36219). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. Study drug and matching placebo were donated by AstraZeneca.
Author Disclosure Statement
G.A.M. has served as a scientific advisor or speaker for Bristol-Myers Squibb, Gilead, ViiV/GlaxoSmithKline, Pfizer, and ICON and has received research grants from Bristol-Myers Squibb, GlaxoSmithKline, and Gilead Sciences. S.M.D. serves on the DSMB for Johnson & Johnson-sponsored studies.