
Abstract
The immune response against HIV and hepatitis C virus (HCV) infection partly depends on chemokine-mediated recruitment of specific T cells. CXCL12 polymorphisms have been associated with AIDS progression and survival, but there are no data related to HCV infection. The aim of this study was to determine whether CXCL12 polymorphisms are related so as to achieve sustained virological response (SVR) after HCV therapy with pegylated-interferon-alpha/ribavirin (pegIFN-α/ribavirin) in HIV/HCV-coinfected patients. We carried out a retrospective study in 319 naive patients who started HCV treatment. The CXCL12 (rs266093, rs1029153, and rs1801157) and IL28B (rs12980275) polymorphisms were genotyped by using the GoldenGate assay. Genetic data were analyzed under an additive inheritance model. The overall rates of the SVR were 54.9% (175/319) and 41.5% (90/217) in GT1/4 patients and 83.2% (84/101) in GT2/3 patients. Patients with a favorable CXCL12 rs1029153 T allele had higher SVR rates than patients with the rs1029153 CC genotype (44% CC, 49% CT, and 61.3% TT; p = 0.025). No significant results for the rs266093 and rs1801157 polymorphisms were found. Patients harboring the favorable rs1029153 T allele had significantly increased odds of achieving SVR [adjusted odds ratio (aOR) = 1.55; 95% confidence interval (95% CI) = 1.01; 2.40; p = 0.047]. Moreover, no significant association was found when the study population was stratified by HCV genotype (data not shown), possibly due to the low number of patients in each group. In conclusion, in this study we found that the favorable CXCL12 rs1029153 T allele seems to be related so as to achieve an SVR in HIV/HCV-coinfected patients on pegIFN-α/ribavirin therapy.
H
The dual therapy with pegylated-interferon-alpha plus ribavirin (pegIFN-α/ribavirin) is still used in HIV/HCV-coinfected patients for the treatment of CHC. 2 A sustained virological response (SVR) is achieved in approximately 20–40% of patients infected with HCV genotype 1/4 (GT1/4) and in 50–60% in of patients infected with HCV genotype 2/3 (GT2/3). 2 Today, the best baseline predictors for pegIFN-α/ribavirin therapy include the age, sex, HCV genotype, HCV viral load, liver fibrosis, and single nucleotide polymorphisms (SNPs) around the interleukin 28B (IL28B) gene. 3
Today, the use of new direct-acting antivirals (DAAs) has improved the SVR rate, particularly in difficult-to-treat patients infected with GT1/4. 2 However, despite the emergence of DAAs, pegIFN-α/ribavirin continues to be used alone or in combination with DAAs. 2 In addition, the new DAAs are more expensive and there are serious restrictions for its administration in many regions. For these reasons, treatment with pegIFN-α/ribavirin remains the only therapy option for many patients in the world.
The immune response against HCV infection depends partly on chemokine-mediated recruitment of specific T cells to the liver. 4 CXCL12, also known as stromal-derived factor 1 alpha (SDF1α), is the specific ligand for CXCR4 and CXCR7. 5 The CXCL12/CXCR4 axis has been besieged by many pathogens that employ a range of strategies to modify or exploit CXCR4 activity. Although CXCL12/CXCR4 has been identified as a critical cofactor for early entry of HIV into CD4+ T cells, other viruses may utilize CXCR4 to gain cell entry as well, modulate CXCR4 expression, or alter its functional activity, with direct effects on cell trafficking, immune responses, cell proliferation, and cell survival. 5 In HCV infection, the CXCL12/CXCR4 axis has an important role in the recruitment and retention of immune cells in the liver, 6 and it has been associated with developing fibrosis, cirrhosis, and hepatocellular carcinoma during CHC. 6 –9 Moreover, the CXCR7–CXCL12 complex may act in two ways: first, as a modulator of CXCR4 signaling when it acts as a scavenger of extracellular CXCL12, and second, by promoting migration and chemotaxis when there is heterodimerization of CXCR7 with CXCR4. 5
Few studies have linked CXCL12 polymorphisms with viral infections. The CXCL12 rs1801157, the best-studied polymorphism in the CXCL12 gene, has been associated with effects ranging from strong protection 10,11 to enhancement 12,13 of AIDS progression. In addition, the rs1801157 polymorphism did not seem to have an effect on susceptibility to HIV-1 infection. 14 There are no data concerning CXCL12 SNPs and CHC.
The aim of this study was to determine whether CXCL12 polymorphisms are related so as to achieve an SVR after HCV therapy with pegIFN-α/ribavirin in HIV/HCV-coinfected patients.
We carried out a retrospective study in all HIV/HCV-coinfected patients who started treatment with pegIFN-α/ribavirin on regular follow-up from October 2000 to June 2010 at two reference HIV hospitals located in Madrid (Spain): Hospital Gregorio Marañón and Hospital Carlos III. All patients were European and white.
The criteria for starting HCV antiviral treatment were as follows: (1) Inclusion criteria for CHC were no clinical evidence of hepatic decompensation, detectable HCV RNA by polymerase chain reaction, negative for hepatitis B surface antigen, CD4+ lymphocyte count higher than 200 cells/mm3, and stable cART for at least 6 months before study entry or no need for cART according to treatment guidelines used in the study period. Furthermore, we included only HIV-infected patients who had an available DNA sample for DNA genotyping. (2) Exclusion criteria were active opportunistic infections, active drug or alcohol addiction, and other concomitant diseases or conditions such as diabetes, nephropathies, autoimmune diseases, hemochromatosis, primary biliary cirrhosis, Wilson's disease, α1-antitrypsin deficiency, and neoplasia. Finally, we included only 319 patients who had an available DNA sample and genotyping data.
The study was conducted in accordance with the Declaration of Helsinki and patients gave their written consent. The Institutional Review Board and the Research Ethic Committee of the Instituto de Salud Carlos III (ISCIII) approved the study.
HCV infection was documented in all patients by an enzyme-linked immunosorbent assay (ELISA) and polymerase chain reaction (PCR) test. HCV genotype was determined by hybridization of biotin-labeled PCR products to oligonucleotide probes bound to nitrocellulose membrane strips (INNO-LiPA HCV II, Innogenetics, Ghent, Belgium). Plasma HCV-RNA viral load was measured by PCR (Cobas Amplicor HCV Monitor Test, Branchburg, NJ) and real-time PCR (COBAS AmpliPrep/COBAS TaqMan HCV test); results were reported in terms of international units per milliliter (IU/ml), with a lower limit of detection of 10 IU/ml.
Liver fibrosis was assessed by different methods, depending on the hospital: (1) Hospital Gregorio Marañon employed liver biopsy and the fibrosis score was estimated following the criteria established by the METAVIR Cooperative Study Group: F0, no fibrosis; F1, portal fibrosis; F2, periportal fibrosis or rare portal–portal septa; F3, fibrous septa with architectural distortion but with no obvious cirrhosis (bridging fibrosis); and F4, definite cirrhosis. (2) Hospital Carlos III used transient elastometry (FibroScanR, Echosens, Paris, France) and liver stiffness values ≤7.0, between 7.1 and 9.4, between 9.5 and 12.4, and ≥12.5 were considered to correspond to Metavir scores F0–F1, F2, F3, and F4, respectively.
Treatment regimens included pegIFN-α 2a or 2b at standard doses (180 μg/week or 1.5 μg/kg/week, respectively) plus weight-adjusted ribavirin dosing (1,000 mg/day for patients weighing <75 kg and 1,200 mg/day for patients weighing ≥75 kg). Following international guidelines, 15 patients with HCV genotypes 1 or 4 received either 48 or 72 weeks of treatment, and patients with HCV genotype 2 or 3 were treated for 24 or 48 weeks, depending on the virological response at week 4. An SVR was defined as an undetectable serum HCV-RNA level (<10 IU/ml) at week 24 after the end of treatment.
We have analyzed the most common SNPs included in the CXCL12 family using the databases of the HapMap Project (
Genomic DNA was extracted from peripheral blood with the Qiagen kit (QIAamp DNA Blood Midi/Maxi; Qiagen, Hilden, Germany). DNA samples were sent to the Spanish National Genotyping Center (CeGen;
Statistical tests were performed with the Statistical Package for the Social Sciences (SPSS) 19.0 software (IBM Corp., Chicago, IL). All p-values were two-tailed and statistical significance was defined as p < 0.05. Data were analyzed by on-treatment analysis of observed data. Patients who prematurely interrupted their HCV treatment due to adverse events, abandonment, or loss to follow-up were eliminated from the analysis.
The genetic analysis was carried out according to an additive inheritance, which was the model that best fit our data according to the statistical power to detect significant associations. The chi-squared/Fisher's exact test was used for categorical variables. For the association study, logistic regression analysis was used to investigate the relationship between CXCL12 polymorphisms and HCV therapy response. These analyses were adjusted by the most important clinical and epidemiological characteristics. We included the SNP with the Enter algorithm (Forced Entry) and the covariables with the Stepwise algorithm (at each step, factors are considered for removal or entry: a p-value for entry and exit of 0.15 and 0.20, respectively). Thus, each logistic regression test was adjusted by only the most significant covariables associated with each one of the outcome variables, avoiding overfitting the regression. The covariables used were gender, age, body mass index, nadir CD4+ T cells, cART, HCV genotype, HCV-RNA viral load, liver fibrosis, and IL28B rs12980275 polymorphism.
Hardy–Weinberg equilibrium (HWE) for all SNPs was assessed by a Chi-square test, considering equilibrium when p > 0.05. In addition, pairwise linkage disequilibrium (LD) analysis was computed to detect the intermarker relationship using the standardized r-squared values by Haploview 4.2 software (
Table 1 shows the clinical and epidemiological characteristics of all 319 patients on HCV treatment at baseline (before starting anti-HCV therapy). The overall rates of the SVR were 54.9% (175/319) and 41.5% (90/217) in GT1/4 patients and 83.2% (84/101) in GT2/3 patients.
Categorical variables are expressed in percentage (absolute count).
AIDS, acquired immunodeficiency syndrome; cART, combination antiretroviral therapy; GT, genotype; HCV, hepatitis C virus; HCV-RNA, HCV plasma viral load; HIV, human immunodeficiency virus; HIV-RNA, HIV plasma viral load; IVDU, intravenous drug users; NNRTI, nonnucleoside analog reverse-transcriptase inhibitors; NRTI, nucleoside analog reverse-transcriptase inhibitors; PI, protease inhibitors.
Figure 1 shows the characteristics of CXCL12 SNPs (rs266093, rs1029153, and rs1801157), all located at the UTR-3 region. We found a low LD value for the rs266093/rs1029153 couple (D′ = 0.43), while LD values were higher for the rs1029153/rs1801157 couple (D′ = 0.99) and rs266093/rs1801157 couple (D′ = 0.99) (Fig. 1A). The three SNPs had low r-square values (r-square <0.150), meaning that the CXCL12 SNPs did not provide exactly the same information and the CXCL12 SNPs cannot be substituted for each another. Furthermore, all SNPs had a minimum allele frequency (MAF) >20%, displayed missing values <5%, and were in HWE (p > 0.05) (Fig. 1B). The allelic frequencies in our dataset were in accordance with data listed on the NCBI SNP database.
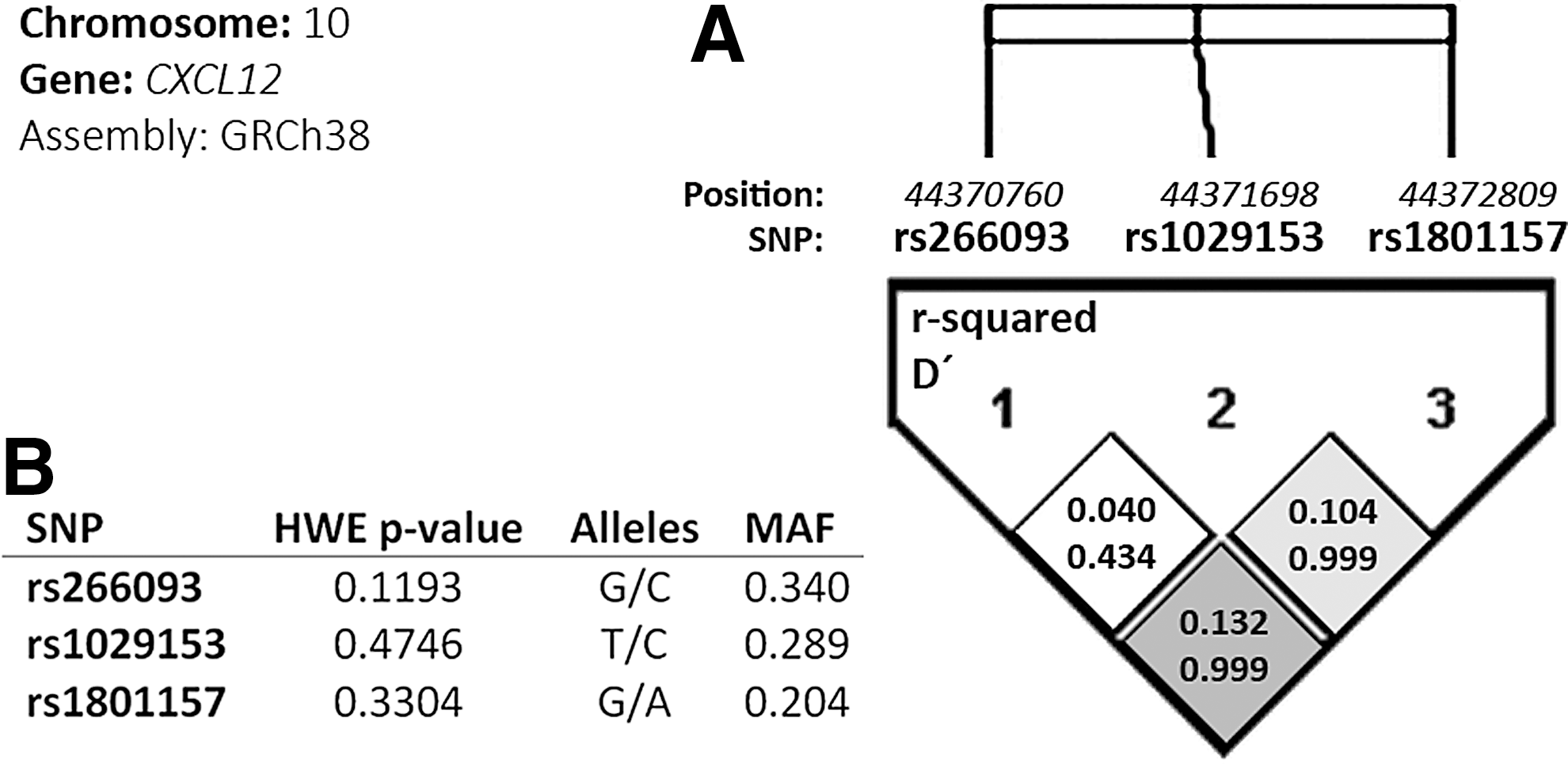
Characteristics of CXCL12 polymorphisms according to genome assembly GCRh38.
Table 2 shows the relationship between CXCL12 polymorphism and HCV therapy outcome. Patients with a favorable CXCL12 rs1029153 T allele had higher SVR rates than patients with the rs1029153 CC genotype (44% CC, 49% CT, and 61.3% TT; p = 0.025) (Table 2). No significant results for rs266093 and rs1801157 polymorphisms were found. To define the independent effect of CXCL12 rs1029153 variants on the response to HCV therapy, we performed a multivariate logistic regression adjusted by the most significant variables. Our data showed that patients harboring the favorable rs1029153 T allele had significantly increased odds of achieving SVR [adjusted odds ratio (aOR) = 1.55 (95% confidence interval (95% CI) = 1.01; 2.40); p = 0.047)] (Table 2). In addition, we did not find significant associations for rs266093 and rs1801157 polymorphisms.
p-values were estimated with Chi-square.
Odds ratios and p-values were calculated by logistic regression analysis adjusted by the most important clinical and epidemiological characteristics (see statistical analysis section).
Statistically significant differences are shown in bold.
95% CI, 95% confidence interval; OR, adjusted odds ratio; HCV-GT, hepatitis C virus genotype.
Moreover, no significant association was found when the study population was stratified by HCV genotype (data not shown), possibly due to the low number of patients in each group (217 in HCV-GT1/4 and 101 in HCV-GT2/3). We also performed an analysis between haplotypes of SDF1 with SVR, but we did not find significant OR values (data not shown). Finally, we analyzed whether there was any epistatic interaction between SDF1 and IL28B polymorphisms, but no significant values were found.
The efficacy of pegIFN-α/ribavirin treatment depends, in part, of the interaction of virus and host factors. 16 Among these, the CXCL12/CXCR4 axis also appears to influence the response to pegIFN-α/ribavirin therapy since baseline chemotaxis of plamacytoid dendritic cells (pDCs) to CXCL12 predicted failure of the antiviral response to HCV and correlated with the histological activity index inflammation score. 17 Thus, it could be possible that CXCL12 may be able to recruit inflammatory cells that are not able to clear HCV during treatment. In this regard, as rs1801157 SNP is located at 3′ UTR of the CXCL12 gene, we analyzed in silico whether this SNP could be part of microRNA (miRNA) binding sites. By using mrSNP, a software to detect SNP effects on microRNA binding, 18 we have found that the minor allele generates putative binding sites for hsa-miR-4777-3p/921/1294, whereas the major allele (T) disrupts these target sites and creates one for hsa-miR-3606. Therefore, it could be predicted that this SNP could affect the miRNA binding sites, and thus could be implicated in differences in CXCL12 expression.
CXCR4 is a coreceptor for the HIV-1 X4 virus and, as such, plays an important role in virus entry into target cells. Thus, CXCL12 may act as an inhibitor of HIV-1 infection in T cell CXCR4+ and antiviral agents that bind to CXCR4 may inhibit HIV-1 entry. 5 In this regard, CXCL12 rs1801157, the best-studied polymorphism in the CXCL12 gene, and other polymorphisms in LD with the rs1801157 have been associated with higher levels of CXCL12. 19 –21 In HIV infection, the CXCL12 rs1801157 polymorphism has been reported to offer strong protection against AIDS progression. 10,11 Moreover, the CXCL12 rs1801157 polymorphism has also been related to enhanced progression to AIDS and shorter survival. 12,13 In our study, we found no apparent influence of CXCL12 SNPs on markers of HIV infection such as nadir CD4+, baseline CD4+, HIV-RNA, and prior AIDS diagnosis (data not shown). Likewise, no significant association between polymorphisms and variables related to the natural history of HCV infection (HCV viral load, liver fibrosis, HCV genotype, etc.) was found. However, we cannot rule out a possible role of SDF1 polymorphisms in the course of HCV natural infection (in nontreated patients). Future studies should be conducted concerning this.
This article focused on pegIFN-α/ribavirin treatment. Currently, the new IFN-α-free regimens with DAAs have improved the SVR rate, especially for difficult-to-treat patients. 22 This fact might diminish the clinical usefulness of biomarkers as predictors of antiviral response. However, not all patients have indications for treatment with these new antivirals. Furthermore, these DAA treatments are still extremely expensive, which results in serious restrictions on their administration and as well as their accessibility for use in many regions of the world. For these reasons, pegIFN-α/ribavirin still remains the backbone of some HCV treatment strategies, and the new DAAs are generally being administered in combination with pegIFN-α/ribavirin. 15 Thus, we consider that the search for new predictors of pegIFN-α/ribavirin-based treatment remains important today and screening for new polymorphisms is a valid pretreatment approach for maximizing treatment success and minimizing HCV therapy-related toxicity.
There are some issues that have to be considered for the correct interpretation of the data. First, this report has a retrospective design and the number of patients was relatively small. This could limit the achievement of statistically significant values between CXCL12 polymorphisms and SVR, especially when we performed the stratified analysis according to the HCV-GT. Second, HCV therapy regimens were not identical for all patients since they varied in characteristics such as pegIFN-α 2a or 2b and likely varied as well for ribavirin (RBV) dose. Instead, each physician administered the appropriate HCV therapy regimen according to his or her criteria and by following local and/or international guidelines. Third, the patients selected for our study met a set of criteria for starting HCV treatment (e.g., no alcohol abuse, high CD4 cell counts, controlled HIV replication, and good treatment adherence), and it is possible that this may have introduced a selection bias. Fourth, our study was carried out entirely on white patients; therefore since the frequency of these alleles varies among ethnicities, an independent study with different ethnic groups would clarify the current data. Fifth, our study included only HIV/HCV-coinfected patients, and results may differ in HCV-monoinfected patients. However, we did not have access to a cohort of HCV-monoinfected patients. The absence of another cohort of monoinfected patients with only HCV may preclude assessing the influence of HIV infection in our results. Sixth, regarding the statistical significance, there is considerable controversy about adjusting the “p-value” after multiple tests on clinical-oriented studies. 23,24 In our study there was a hypothesis supported by theory and previous reports on HIV-infected subjects. 10 –13 Therefore, we were not literally doing a random search of a meaningful result, and our results should not be affected by the fact that we carried out a large number of statistical tests.
In conclusion, our data show that the presence of the favorable CXCL12 rs1029153 T allele might be related to more easily achieving an SVR in HIV/HCV-coinfected patients on pegIFN-α/ribavirin therapy. Further analyses are needed to determine the potential use of the CXCL12 rs1029153 polymorphism as a predictive biomarker.
Footnotes
Acknowledgments
The authors wish to thank the Spanish National Genotyping Center (CeGen) for providing the SNP genotyping services (
This work has been supported by grants given by Fondo de Investigación de Sanidad en España (FIS) [Spanish Health Foundation for Research] [grants PI11/01556, PI14/01094, PI11/00245, and PI14CIII/00011], Red Española de Investigación en SIDA (RIS) [AIDS Research Network] [grants RD12/0017/0024, RD12/0017/0004, and RD12/0017/0031], and “Fundación para la Investigación y la Prevención del Sida en España” (FIPSE) [grant 361020/10]. D.P-T., M.A.J-S., and M.G-A. are supported by “Instituto de Salud Carlos III” [grants CM12/00043, CM10/00105, and CD12/00442, respectively]. J.B. is an investigator from the Programa de Intensificación de la Actividad Investigadora en el Sistema Nacional de Salud (I3SNS).
This work has been (partially) funded by the RD12/0017/00XX project as part of the Plan Nacional R + D + I and cofinanced by ISCIII–Subdirección General de Evaluación y el Fondo Europeo de Desarrollo Regional (FEDER).
Author's contributions: D.P-T., M.A.J-S., and S.R. performed all statistical analysis, interpretation of the data, and wrote the manuscript. J.B. and S.R. participated in the study concept and design. J.B., F.T., C.D., A.C., and T.A-E. participated in patient selection, collection of samples, and acquisition of data. A.F-R. and M.G-A. participated in sample preparation, DNA isolation, and genotyping preprocedure, and contributed a critical revision of the manuscript. S.R. supervised the study. All authors revised the manuscript from a draft by S.R.
Author Disclosure Statement
No competing financial interests exist.