
Abstract
HIV is known for its genetic variability across the globe. The HIV epidemic in India is primarily driven by subtype C, although sporadic circulating and unique recombinant forms are also reported from a few metropolitan cities in which genotyping facilities are available. Here we report a novel CRF01_AE/C recombinant from a multicenter study on the effectiveness of antiretroviral therapy (ART), 12 months after its initiation. Our subject is a 32-year-old heterosexual female, a native of Pune city in western India. Identification and analyses of recombination breakpoints using jpHMM@Gobics and SimPlot bootscanning revealed six recombination breakpoints, indicating insertion of the CRF01_AE genome at three points in the backbone of subtype C. Both subtype C and CRF01_AE are commonly seen in the population at risk of heterosexual HIV transmission, thereby providing an opportunity for cocirculation and recombination. The emergence of a novel recombinant of CRF01_AE/C is indicative of the increasing genetic diversity of the HIV epidemic in India.
W
Hence, over the past few years newer circulating recombinant forms (CRFs) and unique recombinant forms (URFs) are being reported extensively across the globe. Introduced around 1971, HIV-1 subtype C infection is most predominant in India irrespective of the route of transmission, although cases of infection with subtype A, B, CRF 01_AE, and recombinants of A/C or B/C have also been reported. 4 –7 However, CRF01_AE is spreading in epidemic proportions in neighboring Southeast Asian countries. 8 Both subtype C and CRF01_AE are predominantly seen among people at risk of heterosexual transmission, which can provide an opportunity for cocirculation and recombination. 9,10 In this study we characterize the near full-length genome (NFLG) of HIV-1 URF involving subtype C and CRF01_AE from Pune city in Western India.
In August 2014, a 32-year-old heterosexual female, on ART with zidovudine, lamivudine, and efavirenz, presented for routine follow-up at a free ART clinic in Pune city. She acknowledged a high adherence to ART over the past 6 months. Despite this high adherence, she was diagnosed with immunological failure based on a decline in CD4 cell count from 150 cells/mm3 to 18 cells/mm3 1 year after initiation of ART. She underwent plasma viral load testing and drug resistance genotyping after obtaining informed consent in a multicenter study on the “Effectiveness of ART at 12 months after its initiation.” The parent study was approved by the Ethics Committee of the National AIDS Research Institute and her plasma sample was identified by a unique ID, NARI-FLS_YCM-151.
Her plasma viral load was 72,994 copies/ml at the time of genotyping. Multiple drug resistance mutations were observed in the reverse transcriptase (RT) sequence on population-based in-house drug resistance genotyping, which was validated previously. 11 Initial phylogenetic assessment of the partial pol gene sequence [protease (PR), 1–99 amino acid and RT, 1–256 amino acid] in the Stanford University HIVdb genotypic resistance interpretation algorithm results revealed 92.3% similarity of PR with subtype C and 90.5% similarity of RT with CRF 01_AE. Revelation of discordant subtypes of PR and RT prompted us to perform NFLG analysis.
Briefly, total nucleic acid extraction from 500 μl of plasma was done by the NucliSENS EasyMAG (Biomerieux, Durham, NC) automated nucleic acid extraction system followed by reverse transcription into cDNA by the Qiagen One step RT-PCR kit (Qiagen, Hilden, Germany). A three amplicon strategy was used to amplify NFLG comprising overlapping fragments of 2.6 kb (gag–pol), 3.7 kb (pol–vpu), and 3.3 kb (env–nef) as described by Nadai et al.
12
The amplified products from each fragments were visualized on UV gel electrophoresis and sequenced on an automated genetic analyzer ABI 3730 XL DNA Sequencer (Applied Biosystems Inc., Foster City, CA). A total of 45 primers were used for sequencing and a contig sequence was formed using SeqScape Ver. 2.6 (Applied Biosystems). The NFLG sequence of NARI-FLS_YCM-151 was aligned with reference subtype C, CRF01_AE, and A1 and B sequences obtained from the Los Alamos HIV Database (
The 8388-base pair (bp) NFLG sequence spanned from nucleotide position 792 to 9180 corresponding to the reference HXB2 strain. Phylogenetic analysis of the complete genome showed clustering of the NARI-FLS_YCM-151 sequence within Clade C radiation but away from Indian subtype C sequences, suggestive of recombination (Fig. 1). Initial scrutiny by the RIP program (
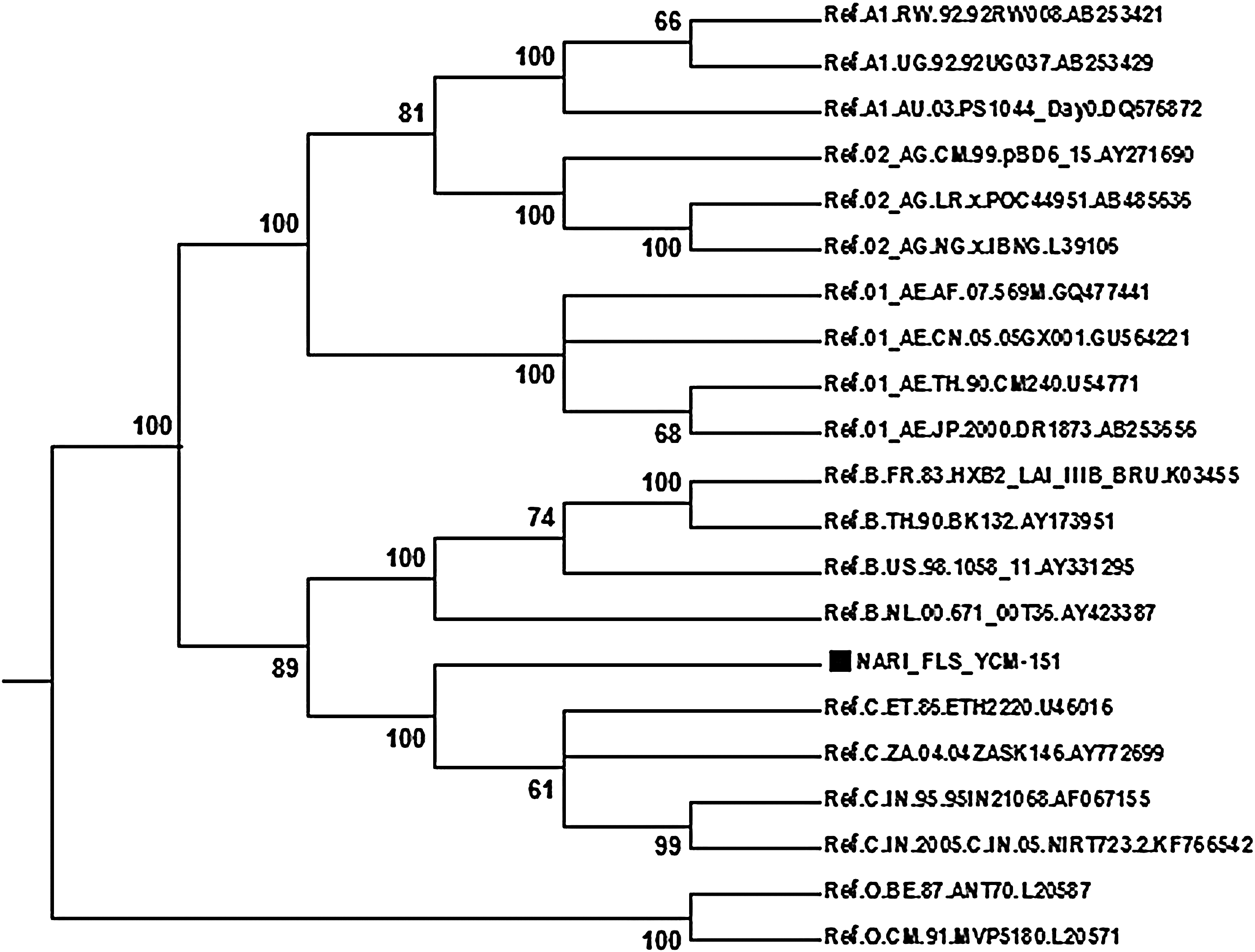
The condensed phylogenetic tree (cut off value 60%) of near full-length sequences showing the relationship of NARI-FLS_YCM-151 with other common subtypes of HIV-1 seen in India. All the reference sequences were retrieved from the Los Alamos National Laboratory HIV Sequence Database. The NARI-FLS_YCM-151 sequence is labeled with a black solid square.
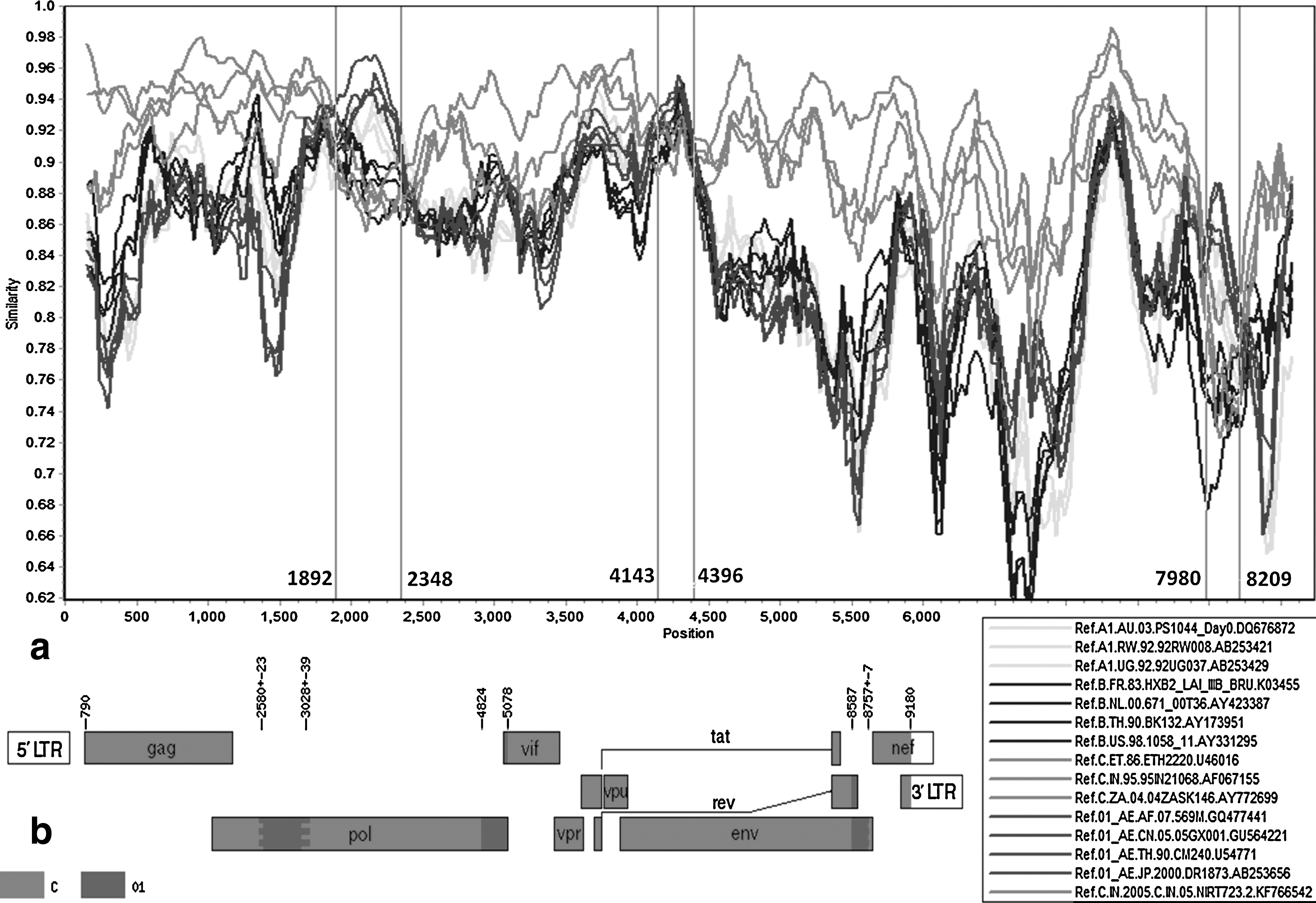
Bootscanning analysis of a near full-length sequence of NARI-FLS_YCM-151.
The results of subregion phylogenetic tree analyses of the recombinant genome showed the following: region I (Nt positions 790 to 2556), subtype C; region II (Nt positions 2603 to 2988), CRF01_AE; region III (Nt positions 3067 to 4823), subtype C; region IV (Nt positions 4824 to 5077), A1/CRF01_AE; region V (Nt positions 5078 to 8586), subtype C; region VI (Nt positions 8587 to 8749), CRF01_AE; and region VII (Nt positions 8764 to 9180), subtype C (Fig. 3). In the subtree phylogenetic analysis of region IV, the 253-bp segment identified by SimPlot appeared closer to subtype A1 rather than CRF01_AE due to inadequate genetic information evident by a lack of grouping of the reference A1 subtype as well as CRF01_AE. In addition, this specified region in CRF01_AE is closely related to subtype A as the origin of subtype E remains obscure. 9
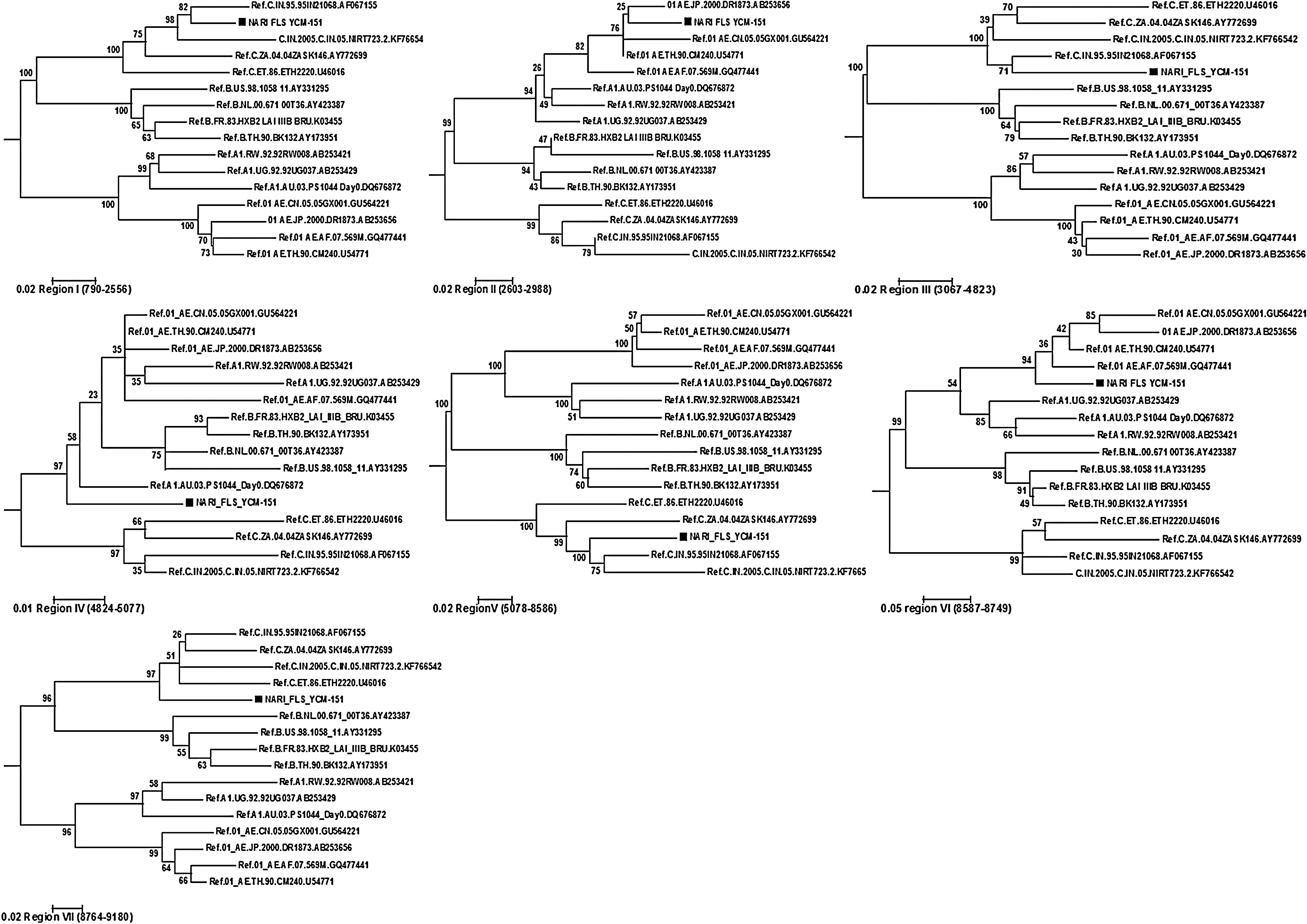
Subgenomic phylogenetic analyses of seven mosaic segments identified by SimPlot bootscanning. The phylogenetic trees were constructed with MEGA 6.06 using the maximum likelihood method under the General time reversible model and the discrete Gamma was distributed with invariant sites (G + I) with the number of discrete gamma category 5.
The 385-bp insertion of CRF01_AE in region II (Nt positions 2603 to 2988) belongs to the RT region of the pol gene. This region harbored multiple drug resistance mutations (DRMs) against nucleoside reverse transcriptase inhibitors (M41L, D67N, M184V, L210W, T215Y, and K219N) and nonnucleoside analogue reverse transcriptase inhibitors (V90I, A98G, K103N, and K238T). There were no major DRMs against protease inhibitors (PIs) or integrase inhibitors except for L10I, which is a minor DRM against PI.
Although the ART regimen does not differ across various subtypes, the response to treatment may vary. Recently Kantor et al. 13 indicated that those infected with subtype C were more likely to fail ART and to fail earlier than those infected with subtype B. In addition, a prospective study on 1036 Asian patients concluded that individuals infected with CRF01_AE have a reduced immunologic response after 12 months of ART as compared to subtype B-infected counterparts. 14 In the present case, the woman showed poor immunological response and treatment failure with the development of multiple DRMs within 12 months of initiation of ART. She also developed cryptococcal meningitis despite high adherence.
The HIV epidemic in India is driven by subtype C and is concentrated among high-risk groups, namely female sex workers (FSW), men who have sex with men (MSM), transgenders, and intravenous drug users. 1 However, a recent study has highlighted the primary role of Thailand and the secondary role of Japan in the global dispersion of CRF01_AE. 8 Our subject was monogamous and denied any travel outside the country. Her HIV-seropositive husband died 4 years previously. He allegedly contracted HIV from multiple exposures to sex workers in Mumbai. A significant proportion of FSW in western India comes from West Bengal, Bangladesh, and Nepal, possibly explaining the origin of the CRF01_AE recombination in this case. 15
To conclude, we report a novel recombinant form involving CRF01_AE and subtype C from a female with rapid treatment failure. Reporting of newer recombinants is necessary to understand the evolution and genetic diversity of HIV in a country. In addition, we should be vigilant about newer recombinants and their clinicoepidemiological profile, which may change the face of the current HIV epidemic.
Sequence Data
The GenBank accession numbers obtained for the partial pol gene sequence used in drug resistance genotyping and the near full-length genomic sequence of NARI-FLS_YCM-151 are KR816077 and KT074935, respectively.
Footnotes
Acknowledgments
The authors would like to thank the counselor Girish Rahane, the staff from the Yashwantrao Chavan Memorial Hospital ART Center for their help with sample collection, and the patient who agreed to participate in the present study. This work is supported by an intramural grant from the National AIDS Research Institute (Indian Council of Medical Research), Pune.
Author Disclosure Statement
No competing financial interests exist.