
Abstract
Background:
Antiretroviral therapy (ART) markedly reduces the risk of HIV-1 transmission in serodiscordant partnerships. We previously found that younger age and higher CD4 counts were associated with delayed initiation of ART by HIV-1-infected partners in serodiscordant partnerships. Among those initiating ART, we sought to explore whether those same factors were associated with failure to achieve viral suppression.
Methods:
In a prospective study of HIV-1-infected persons who had a known heterosexual HIV-1-uninfected partner in Kenya and Uganda [Partners Pre-Exposure Prophylaxis (PrEP) Study], we used Cox proportional hazards regression to evaluate correlates of viral nonsuppression (HIV-1 RNA >80 copies/ml).
Results:
Of 1,035 HIV-1-infected participants initiating ART, 867 (84%) achieved viral suppression: 77% by 6 months and 86% by 12 months. Younger age [adjusted hazard ratio (aHR) 1.05 for every 5 years younger; p = .006], lower pretreatment CD4 count (aHR 1.26; p = .009 for ≤250 compared with >250 cells/μl), and higher pretreatment HIV-1 RNA quantity (aHR 1.21 per log10; p < .001) independently predicted failure to achieve viral suppression. Following initial viral suppression, 8.8% (76/867) experienced virologic rebound (HIV-1 RNA >200 copies/ml): 6.3% and 11.5% by 6 and 12 months after initial suppression, respectively. Age was the only factor associated with increased risk of virologic rebound (aHR 1.33 for every 5 years younger; p = .005).
Conclusions:
For HIV-1-infected persons in serodiscordant couples, younger age was associated with delayed ART initiation, failure to achieve viral suppression, and increased risk of virologic rebound. Motivating ART initiation and early adherence is a key to achieving and sustaining viral suppression.
Introduction
T
The concentration of HIV-1 RNA in plasma is the principal indicator of ART prevention effectiveness. Nonadherence to ART increases the likelihood of poor virologic outcomes, including viral nonsuppression, virologic rebound, disease progression, and HIV-1 transmission, including transmission of drug-resistant virus. 7,8 In resource-rich settings, younger age predicts nonadherence, viral nonsuppression, virologic rebound, and loss to follow-up. 9 Correlates of ART nonadherence include lower income, depression, alcohol and substance use, and lack of social support. 10 –14 Nonadherence also occurs when asymptomatic individuals on ART skip doses or stop treatment completely because they feel well. 15 As ART for HIV-1 prevention is scaled-up, and ART is prescribed to healthy individuals with higher CD4 counts more generally, it will be critical to understand and address preventable factors related to viral nonsuppression.
We previously reported that younger individuals and persons with higher CD4 counts in HIV-1 serodiscordant partnerships in Kenya and Uganda were more likely to delay ART initiation. 16 In this study, we evaluated correlates of nonsuppression among the subset of HIV-1-infected partners who initiated ART. We sought to evaluate whether factors that predicted delay in ART initiation were similarly related to failure to achieve viral suppression and virologic rebound after initial suppression.
Materials and Methods
Study cohort and procedures
We conducted a prospective study among HIV-1-infected partners in HIV-1 serodiscordant couples enrolled in the Partners Pre-Exposure Prophylaxis (PrEP) Study, a randomized clinical trial of daily oral PrEP to decrease HIV-1 acquisition among HIV-1-uninfected members of serodiscordant couples (
CD4 testing was performed at baseline and every 6 months thereafter at study site laboratories using the BD FACSCalibur or BD FACSCount instrumentation (BD Biosciences). 18 Plasma for HIV-1 RNA quantification was collected at enrollment and every 6 months thereafter and archived and batch tested at the University of Washington after the end of the study using the Abbott m2000 Real-Time HIV-1 RNA assay (Abbott); the lower limit of quantification was 80 copies/ml. Viral load testing was not standard of care, and results were not available until after the study ended.
Statistical analyses
Participants were included in the analyses if they initiated ART during study follow-up, had a pre-ART plasma HIV-1 RNA concentration >80 copies/ml, and had at least one HIV-1 RNA quantification after starting treatment. Failure to achieve viral suppression (the primary outcome) was defined as plasma HIV-1 RNA concentration >80 copies/ml. We used a Cox proportional hazards regression model to assess factors related to viral nonsuppression. Baseline factors evaluated included age, gender, years of education, duration of partnership and known HIV-1 serodiscordant status, monthly income, alcohol use, pretreatment CD4 count, and HIV-1 RNA concentration. Unprotected sex in the prior month and pregnancy were evaluated as time-varying covariates. Factors with p ≤ .20 in bivariate analyses were included in multivariate models. In sensitivity analyses, we repeated our primary analysis by including subjects who achieved viral suppression before reporting ART use (although this potentially indicated unreported ART use before first reporting having started ART 19 ) and by using a different cutoff (HIV-1 RNA concentration >400 copies/ml) to define viral nonsuppression. In addition, we assessed factors associated with virologic rebound, which we defined as HIV-1 RNA concentration >200 copies/ml following initial viral suppression. Statistical analyses were performed using SAS version 9.3 and Stata 12.1.
Ethical approval
The Partners PrEP Study was approved by the University of Washington Human Subjects Review Committee and ethics review committees at all collaborating institutions. All participants provided written informed consent.
Results
Participant characteristics
Of the 4,747 HIV-1-infected participants enrolled and followed in the Partners PrEP Study, 1,817 initiated ART during study follow-up, of whom 1,035 (57%) were included in the primary analysis (Fig. 1). The median age was 35 years [interquartile range (IQR) 28–41] and 560 (54%) were women (Table 1). Most (98%) were married or cohabiting with their HIV-1-uninfected partner. The median duration of partnership was 9 years (IQR 3–16), and 263 (26%) reported having unprotected sex with the study partner at enrollment. The median body mass index was 22 kg/m2 (IQR 20–24) for women and 21 kg/m2 (IQR 20–23) for men. Women had higher median pre-ART CD4 counts than men (260 vs. 246 cells/μl; p < .0001). The median HIV-1 RNA plasma concentration before ART start was 4.44 log10 copies/ml (IQR 3.90–4.89): 4.57 and 4.30 log10 copies/ml in men and women, respectively. As previously reported, study retention was high in the Partners PrEP Study, with at least 91% of HIV-1-infected partners retained at all study visits. 20
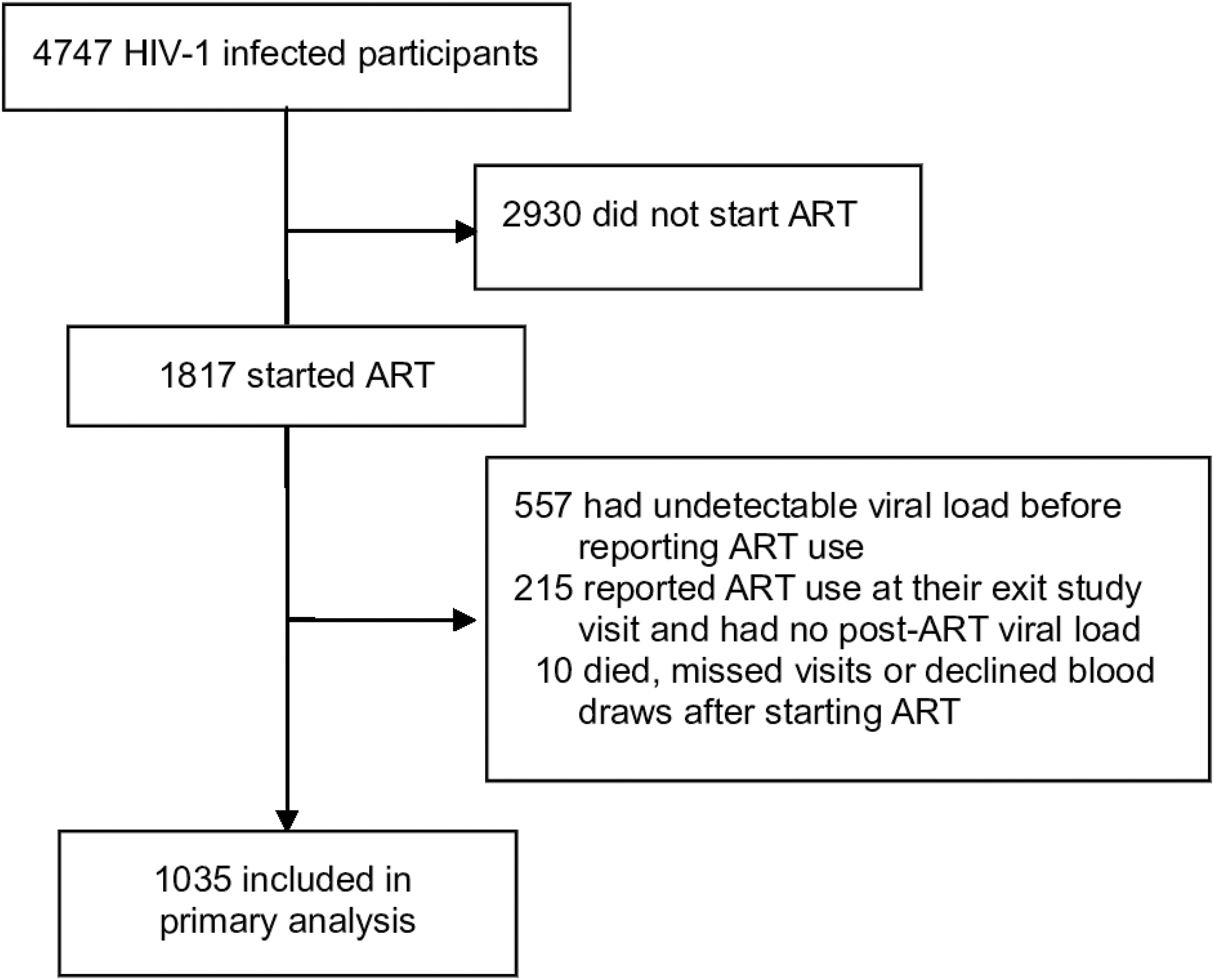
Study profile. ART, antiretroviral therapy.
The aHR for younger age differed by <1% after stratifying by study site (aHR 1.052).
Pregnancy and unprotected sex were analyzed as time-varying covariates. These are visits at which unprotected sex was reported or the woman was pregnant, and blood was collected for plasma viral load quantification.
aHR, adjusted hazard ratio; CI, confidence interval; IQR, interquartile range.
Plasma viral suppression and correlates of nonsuppression
After ART initiation, HIV-1-infected participants were followed for 467 person-years for the assessment of viral suppression, with a median duration of follow-up of 13.8 months (IQR 7.8–19.4). Overall, 867 (84%) achieved viral suppression and the median time to first viral suppression was 3.1 months (IQR 2.8–5.6). The cumulative probabilities of achieving viral suppression at 3, 6, 12, and 24 months after starting ART were 46.7%, 76.7%, 86.0%, and 90.1%, respectively (Fig. 2).

Time to first viral suppression following ART initiation.
In bivariate analyses, younger age (p = .01), lower CD4 count before treatment initiation (p = .003), and higher pretreatment HIV-1 RNA concentration (p < .001) were significantly associated with viral nonsuppression (Table 1). In the adjusted model, the likelihood of viral nonsuppression increased by 5% for every 5-year decrease in age [adjusted hazard ratio (aHR) 1.05; p < .006]. Lower pretreatment CD4 count (aHR 1.26 for ≤250 compared with >250 cells/μl; p = .009) and higher pretreatment HIV-1 RNA concentrations (aHR 1.21 per log10; p < .001) were also significantly associated with failure to achieve viral suppression in plasma.
In sensitivity analyses, with viral nonsuppression defined as HIV-1 RNA >400 copies/ml, our findings were similar to the primary analysis (Table 2). Failure to achieve viral suppression was independently associated with younger age (p = .01), lower pretreatment CD4 count (p = .004), and higher pretreatment HIV-1 RNA quantity (p = .008). Similar findings were obtained when HIV-1-infected persons who achieved viral suppression before reporting ART use (n = 557, Fig. 1) were included (Table 2).
Virologic rebound
The 867 HIV-1-infected partners who achieved viral suppression were followed for 688 person-years for assessment of virologic rebound. Of the 76 persons (8.8%) who experienced virologic rebound (HIV-1 RNA >200 copies/ml), 51 (67%) were women. The cumulative probabilities of virologic rebound at 6 and 12 months after viral suppression were 6.3% and 11.5%, respectively (Fig. 3). The median HIV-1 RNA concentration at the first occurrence of virologic rebound was 1,244 copies/ml (IQR 208–7894); however, 24% (18/76) subsequently were suppressed (HIV-1 RNA <80 copies/ml) before their last study visit.
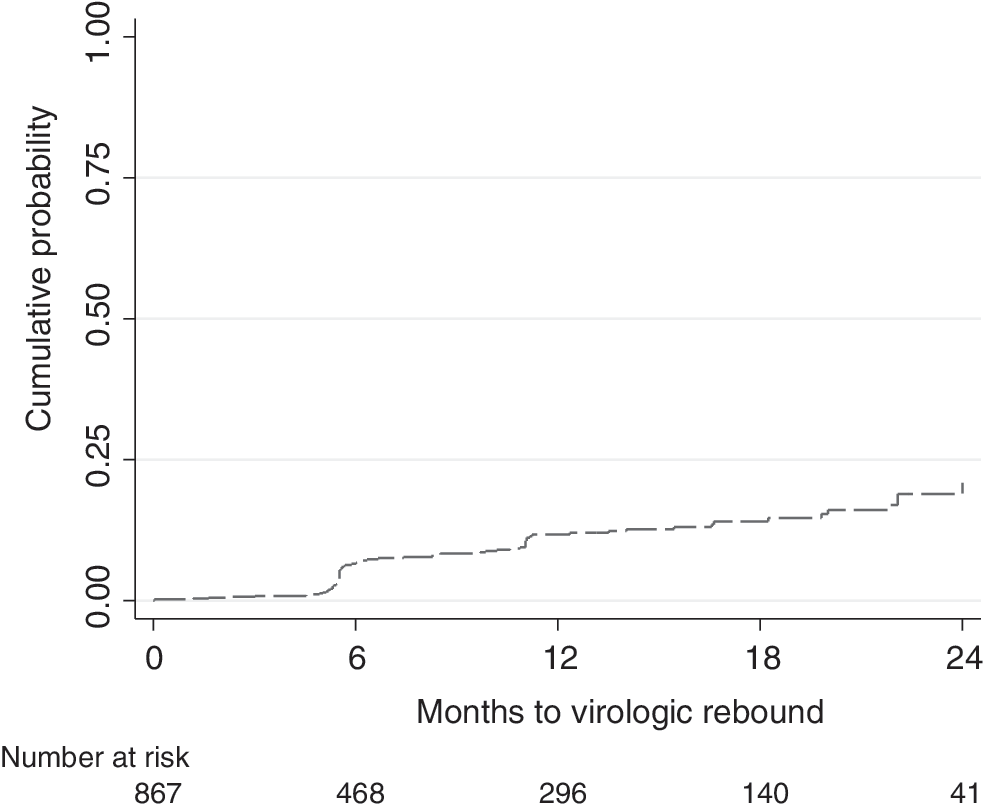
Cumulative probability of virologic rebound following initial viral suppression.
In bivariate analyses, age [HR 1.35 for every 5 years younger; 95% confidence interval (CI): 1.18–1.54; p < .001] and female gender (HR 1.95; 95% CI: 1.20–3.16; p = .007) were associated with virologic rebound, but pregnancy (p = .31) and pretreatment HIV-1 RNA concentrations (p = .67) were not. After adjusting for gender, age remained the only independent predictor of virologic rebound (aHR 1.33 for every 5 years younger; 95% CI: 1.14–1.56; p = .005); gender was not statistically significant after controlling for age (p = .8).
Discussion
In this prospective study of ∼1,000 East African HIV-1-infected persons in serodiscordant partnerships, nearly all HIV-1-infected persons achieved plasma viral suppression after starting ART. Younger age, lower CD4 count, and higher HIV-1 RNA concentrations at treatment initiation independently predicted failure to achieve viral suppression in plasma. Younger age was the only significant factor associated with virologic rebound after initial viral suppression. In previous work from this cohort, younger age and higher pretreatment CD4 counts predicted delays in ART initiation in the same population. Unique to this population, all individuals initiating ART had a known HIV-1-uninfected partner, and all were counseled about both treatment and prevention benefits of ART.
Younger age has been associated with lower rates of HIV-1 virologic suppression in prior studies. A review of 49,921 HIV-1-infected persons on ART in 33 European cohorts found that increasing age correlated with better virologic outcomes. 21 A study of ∼9,000 adults on ART in South Africa found lower rates of virologic suppression in younger adults (16–24 years) compared with those aged 25–49 years. 22 These data suggest that younger age predicts failure to achieve viral suppression and that this risk decreases with age. Younger age is associated with poor ART adherence. 23 –25 Younger age also predicted low PrEP adherence in our cohort. 26 Behavioral and psychosocial correlates of nonadherence in young adults include anxiety and depression, 13,27 HIV-1-associated stigma and discrimination, lack of disclosure, feelings of invulnerability to the consequences of HIV-1 disease, 9,28 alcohol and recreational drug use, 27 and low socioeconomic status. 29 These factors may mediate the observed association among younger age, nonadherence, and poor virologic outcomes.
Our finding that younger age predicts virologic rebound is consistent with prior studies, which reported lower risk of viral rebound with older age 30,31 and a significantly shorter time to viral rebound in younger adults (20–29 years) compared with older (≥30 years). 32 In a prospective study of 1,305 HIV-1-infected persons on ART in British Columbia, younger age was independently associated with viral rebound after initial viral suppression. 33 Predictors of nonadherence in sub-Saharan Africa include higher pill burden (twice-daily regimens vs. once-daily regimens), 34 stavudine-containing regimens, 35 geographic or transportation-related barriers, 36 and Global Positioning System measured distance from home to clinic. 37 In multiple settings, younger age predicts virologic rebound, and clinicians and ART programs should more effectively address behavioral, structural, and psychosocial barriers to ART adherence and provide adherence support for younger HIV-infected persons initiating ART.
We previously reported that younger age predicted delayed ART initiation in this cohort. 16 In contrast, a South African study found no age difference between ART initiators and refusers. 38 Delayed ART initiation is common in sub-Saharan Africa 39 –42 and results from health system, provider, and patient-level factors. 41,43 –46 Individuals who delay ART initiation may not be motivated to achieve the high level of adherence needed to achieve and sustain viral suppression 47 or may have competing priorities, less stable lives, and less familiarity or experience with daily treatment. Our finding that younger age predicts ART noninitiation, delays in achieving viral suppression, and virologic rebound points to a common theme related to ART barriers. Patient-level barriers to ART initiation are often similar to adherence barriers and include denial of the need to start treatment, lack of motivation to stay on treatment, fear of side effects, lack of social support, stigma, fear of disclosure, and the perception that starting ART signifies AIDS and impending mortality. 41,46 –52 Lower mental health scores were the only psychosocial variable significantly associated with poor adherence in a randomized trial of ART for HIV-1 prevention (HPTN 052). 53 These factors may influence adherence during the initial period after ART initiation, as well as subsequent virologic outcomes. Durable viral load suppression is the ultimate goal of ART, both for individual health outcomes and for treatment as prevention. Addressing adherence barriers is a key to improving virologic outcomes in younger adults. Evidence-based interventions to improve adherence include once-daily regimens, fixed-dose combinations, reminder devices, mobile health technology, and provision of one-on-one or couple-based adherence support with feedback about viral suppression. 53,54
The strengths of our study include the prospective design, large sample size, the diversity of a multinational cohort specifically of HIV-1-infected persons with known HIV-1-uninfected partners, regular clinical and laboratory monitoring of HIV-1-infected participants, and robustness of results in sensitivity analyses. Limitations of the analysis include time-limited follow-up after ART initiation, lack of in-depth psychometric surveys to understand the bases for adherence and nonadherence, and reasons for nonadherence in real time, since viral load testing was conducted after the end of the study. We evaluated participants who were alive and on treatment at the time viral suppression was assessed (on-treatment analysis) and may have overestimated the effectiveness of ART. However, nearly, all HIV-1-infected partners were retained in study follow-up and, thus, our results are unlikely to be influenced by selection bias due to attrition and death.
In conclusion, the majority of heterosexual East African HIV-1-infected persons with known HIV-1-uninfected partners achieved viral suppression. Younger age independently predicted delayed ART initiation, failure to achieve viral suppression, and virologic rebound in this cohort. ART programs should give special consideration to motivating adherence and sustaining viral suppression in younger HIV-1-infected persons in serodiscordant partnerships. Future studies should develop, test, implement, and rigorously evaluate evidence-based interventions to improve ART adherence in young adults and assess their correlation with virologic outcomes.
Footnotes
Acknowledgments
We are grateful to the study participants for their participation and dedication.
Funding Source and Disclaimer
This study was supported through research grants from the Bill & Melinda Gates Foundation (Grant OPP47674) and the National Institute of Mental Health of the US National Institutes of Health (Grant R01 MH095507).
Role of the Funding Source
The authors designed and executed the study, had full access to the raw data, performed all analyses, wrote the article, and had final responsibility for the decision to submit for publication. The funder had no role in design, data collection, analysis, interpretation, or writing of the report.
Partners PrEP Study Team
University of Washington Coordinating Center and Central Laboratories, Seattle: Connie Celum (Principal Investigator, Protocol Cochair), Jared M. Baeten (Medical Director, Protocol Cochair), Deborah Donnell (Protocol Statistician), Robert W. Coombs, Lisa Frenkel, Craig W. Hendrix, Jairam R. Lingappa, and M. Juliana McElrath.
Study sites and site principal investigators: Eldoret, Kenya (Moi University, Indiana University): Kenneth H. Fife and Edwin Were; Kabwohe, Uganda (Kabwohe Clinical Research Center): Elioda Tumwesigye; Jinja, Uganda (Makerere University, University of Washington): Patrick Ndase and Elly Katabira; Kampala, Uganda (Makerere University): Elly Katabira and Allan Ronald; Kisumu, Kenya (Kenya Medical Research Institute, University of California, San Francisco): Elizabeth Bukusi and Craig R. Cohen; Mbale, Uganda (The AIDS Support Organization, CDC-Uganda): Jonathan Wangisi, James D. Campbell, and Jordan W. Tappero; Nairobi, Kenya (University of Nairobi, University of Washington): James Kiarie, Carey Farquhar, and Grace John-Stewart; Thika, Kenya (University of Nairobi, University of Washington): Nelly R. Mugo; Tororo, Uganda (CDC-Uganda, The AIDS Support Organization): James D. Campbell, Jordan W. Tappero, and Jonathan Wangisi.
Data management was provided by the DF/Net Research, Inc. (Seattle, USA), and site laboratory oversight was provided by the Contract Laboratory Services (CLS) of the Wits Health Consortium (University of the Witwatersrand, Johannesburg, South Africa).
Study medication was donated by the Gilead Sciences.
Author Contributions
A.M. and J.M.B. designed the study and wrote the first draft. A.M. performed the statistical analyses. All authors contributed to data collection, interpretation of the results, and the writing of the article, and all approved the final draft.
Author Disclosure Statement
No competing financial interests exist.