
Abstract
We investigate mutations and correlates according to HIV-1 subtype after virological failure (VF) of standard first-line antiretroviral therapy (ART) (non-nucleoside/nucleotide reverse transcriptase inhibitor [NNRTI] +2 nucleoside/nucleotide reverse transcriptase inhibitor [N(t)RTI]). SECOND-LINE study participants were assessed at baseline for HIV-1 subtype, demographics, HIV-1 history, ART exposure, viral load (VL), CD4+ count, and genotypic ART resistance. We used backward stepwise multivariate regression (MVR) to assess associations between baseline variables and presence of ≥3 N(t)RTI mutations, ≥1 NNRTI mutation, ≥3 thymidine analog-N(t)RTI [ta-N(t)RTI] mutations (TAMs), the K65/K70 mutation, and predicted etravirine (ETV)/rilpivirine (RPV) activity. The inclusion p-value for MVR was p < .2. The exclusion p-value from stepwise elimination was p > .05. Of 541 participants, 491 (91%) had successfully characterized baseline viral isolates. Subtype distribution: B (n = 123, 25%), C (n = 202, 41%), CRF01_AE (n = 109, 22%), G (n = 25, 5%), and CRF02_AG (n = 27, 5%). Baseline CD4+ 200–394 cells/mm3 were associated with <3 N(t)RTI mutations (OR = 0.47; 95% CI 0.29–0.77; p = .003), absence of the K65/K70 mutation (OR = 0.43; 95% CI 0.26–0.73; p = .002), and higher ETV sensitivity (OR = 0.52; 95% CI 0.35–0.78; p = .002). Recent tenofovir (TDF) use was associated with K65/K70 mutations (OR = 8.91; 95% CI 5.00–15.85; p < .001). Subtype CRF01_AE was associated with ≥3 N(t)RTI mutations (OR = 2.34; 95% CI 1.31–4.17; p = .004) and higher RPV resistance (OR = 2.13; 95% CI 1.30–3.49; p = .003), and subtype C was associated with <3 TAMs (OR = 0.45; 95% CI 0.21–0.99; p = .015). Subtypes CRF01_AE (OR = 2.46; 95% CI 1.26–4.78; p = .008) and G (OR = 4.77; 95% CI 1.44–15.76; p = .01) were associated with K65/K70 mutations. Higher VL at confirmed first-line VF was associated with ≥3 N(t)RTI mutations (OR = 1.39; 95% CI 1.07–1.78; p = .013) and ≥3 TAMs (OR = 1.62; 95% CI 1.15–2.29; p = .006). The associations of first-line resistance mutations across the HIV-1 subtypes in this study are consistent with knowledge derived from subtype B, with some exceptions. Patterns of resistance after failure of a first-line ta-N(t)RTI regimen support using TDF in N(t)RTI-containing second-line regimens, or using N(t)RTI-sparing regimens.
Introduction/Background
I
WHO guidelines recommend two nucleos(t)ide reverse transcriptase inhibitors [N(t)RTI] plus either a non-nucleoside reverse transcriptase inhibitor (NNRTI) or a boosted protease inhibitor (PI) for first- and second-line regimens, respectively. 2 In LMICs, it is common practice for HIV-positive individuals to receive zidovudine (AZT), stavudine (d4T), or tenofovir disoproxil fumerate (TDF) as the first N(t)RTI component combined with lamivudine (3TC) as the second N(t)RTI component of the 2 N(t)RTI backbone, combined with an NNRTI, usually nevirapine (NVP) or efavirenz (EFV). 3 The WHO-preferred component since the most recent iteration of the WHO antiretroviral therapy (ART) guidelines for first-line regimen is EFV+TDF/3TC 2 , although for various reasons the transition to the exclusive use of this WHO-recommended regimen has not been universal.
Despite the great successes in supporting access to HIV-1 care in LMIC over the past decade, HIV-1 remains a pressing global health problem. The massive scale-up of cART after the WHO “3 by 5” initiative has come at the inevitable cost of some degree of HIV drug resistance (HIVDR). 4 Significant population-level HIVDR could limit future therapy options requiring new and expensive treatment regimens. 5 WHO has developed a global HIVDR prevention strategy that includes acquired resistance surveillance and viral load (VL) monitoring. This is challenging due to costs and the availability of the requisite technologies, and results have been mixed. 4,6,7
Drug resistance data have historically been relatively limited to subtype B, the predominant subtype in resource-rich countries that accounts for only about 10% of global infections. The differences in HIVDR among other HIV-1 subtypes is far less well researched and only partially understood. 8 –11 Earlier studies have suggested minimal differences in resistance patterns between subtypes. In regard to N(t)RTI resistance mutations, a study from Zimbabwe in 2002 found that subtypes B and C selected mostly the same mutations under similar drug pressure. 12 However, more recently, it has been suggested that subtype C may have a higher propensity for selection of resistance through the K65R mutation. 13,14 Regarding NNRTI resistance mutations, the V106M mutation is commonly seen in subtypes C and CRF01_AE after therapy with efavirenz or nevirapine; whereas in subtype B infections, V106A more commonly emerges. 15 –18 Under PI drug pressure, non-subtype B viruses commonly select particular mutations compared with subtype B viruses, due to polymorphisms in the PI coding regions that are associated with each subtype. Subtypes A, C, and CRF01_AE often select for M89T due to an M89 polymorphism, leading to substantial resistance to nelfinavir, atazanavir, and lopinavir. 19,20 There are few studies comparing HIVDR profiles between subtypes in diverse, well-characterized cohorts. One such instance is Huang et al.’s analysis of a multi-cohort, multi-subtype dataset, 21 building on an earlier work by Kantor et al. 22 The latter study found little difference in resistance mutation positions between non-B and subtype B viruses. The former study found lower mutation frequencies in subtype B and higher frequencies in subtypes C and CRF01_AE.
This study aims at describing patterns of drug resistance mutations and their correlates after virological failure (VF) of first-line therapy consisting of NNRTI +2 N(t)RTIs in patients enrolled in the SECOND-LINE study. 23
Materials and Methods
Study design and participants
A full description of the SECOND-LINE trial has been published. 23 In brief, SECOND-LINE compared the use of ritonavir-boosted lopinavir combined with either 2–3 N(t)RTIs or raltegravir alone for second-line treatment after first-line VF. SECOND-LINE was a randomized, parallel, open-label, multicenter, international trial, enrolling patients from 37 sites in 14 high- and middle-income countries. 23 This sub-study was approved by the UNSW Australia Human Research Ethics Committee as well as by all relevant local institutions. 23
HIVDR testing
To qualify for SECOND-LINE study enrolment, prospective participants had to have a confirmed VL ≥500 copies/mL drawn at least 7 days apart. All enrolled participants were advised to continue to take their failing regimen until they received their randomized second-line regimen on the day of the baseline visit.
Patients were assessed at week 0 (baseline) for demographics, HIV-1 infection history, and previous cART exposure using an electronic case report form. Patients were asked to estimate the month and year of infection; if unknown, then the date of the first HIV-1-positive test was used. Blood samples were collected for plasma VL measurement, genotypic resistance testing, and T-cell counts. VL and genotypic resistance testing for study analysis purposes was performed using samples stored at a single central laboratory (HIV Immunovirology Laboratory, St Vincent's Hospital Centre for Applied Medical Research, Sydney, Australia). The reverse transcriptase and protease regions were sequenced using the ViroSeq HIV-1 genotyping system v2.0 (Catalogue No. 4J94-93; distribution: Abbott Molecular; manufacturer: Celera Corporation, Alameda, CA). The integrase region was sequenced using the ViroSeq HIV-1 integrase genotyping kit v1.0 RUO (Catalogue No. 04J94-71; distribution: Abbott Molecular; manufacturer: Celera Corporation). Major resistance mutations and subtypes were identified according to the Stanford database version 6.3.1. 24 Major mutations are defined by the Stanford database as those that make major contributions to reducing drug susceptibility, usually with a penalty score of 30 to 60. Rilpivirine (RPV) resistance was calculated according to the Stanford HIVdb algorithm, where RPV resistance mutations are assigned drug penalty scores that are added to infer 1 of 5 resistance levels: susceptible, potential low, low, intermediate, and high. 24 Etravirine (ETV) sensitivity was evaluated using a published weighted scoring algorithm based on 17 ETV resistance-associated mutations. Scores are added and stratified into highest, intermediate, and reduced virological responses. 25,26
Statistical analysis
Baseline characteristics and ARV drug resistance profiles were described according to subtype. We analyzed for the following outcomes at baseline: <3 or ≥3 major N(t)RTI mutations, 0 or ≥1 major NNRTI mutations, <3 or ≥3 thymidine analog mutations (TAMs), and K65 or K70 mutations; sensitivity to ETV; and sensitivity to RPV. We assessed each category for association with HIV-1 subtype, age, gender, CD4+ T cells/mm3 (CD4), VL, most recent N(t)RTI and NNRTI, treatment time on thymidine analogs-N(t)RTIs (ta-N(t)RTIs), and exposure to TDF, NVP, and EFV. Variables with association at p-value <.2 were included in multivariate analysis models. Previous exposure to TDF, NVP, and EFV was dropped from the multivariate analyses due to being significantly correlated with the most recent N(t)RTI and NNRTI (r = 0.7668, r = 0.8705, r = −0.8437, respectively). Multivariate models were built using binary logistic and ordinal logistic regression methods with backward stepwise elimination (inclusion p < .05). Results with p < .05 were considered statistically significant. A Bonferroni analysis was performed to correct for multiple comparisons. All analyses were done using Stata 12 software. Outcomes were assessed in study participants who had an amplified sequence at baseline. We made no imputations for missing data. Overall, we hypothesized that rates, types, and predictors of mutations in non-B subtypes would be similar to experience in the western world with subtype B viruses.
Results
Of the 541 participants in the SECOND-LINE study, 491 (91%) had a successfully amplified genotypic antiretroviral resistance test (GART) for analysis (Fig. 1). 23 The mean age (SD) of the group was 38.6 (8.9) years. Overall, 56% of participants were male, 42% were Asian, 37% were African, 14% were Hispanic, and 8% were Caucasian. The mean estimated duration of infection (SD) was 6.6 (4.1) years, and treatment duration was 4.1 (2.9) years. At baseline, 51% had a CD4 cell count of <200 cells/mm3; 33%, 200–349 cells/mm3; 12%, 350–499 cells/mm3; and 4%, ≥500 cells/mm3. The mean VL (SD) was 4.3 (0.9) log10 copies/mL; 80% had a VL ≤100,000 copies/mL. The majority were receiving ta-N(t)RTIs (77%) at the time of screening, whereas the NNRTI component was split 50/50 for EFV and NVP. Eighty-nine percent had been previously exposed to ta-N(t)RTIs; 21%, to TDF; 57%, to EFV; and 57%, to NVP (Table 1).

Study population profile.
The most prevalent subtype was subtype C (41%), followed by B (25%), CRF01_AE (22%), CRF02_AG (5%), and G (5%). Subtype B was seen in 54% Hispanic and 32% Caucasian participants; subtype C was seen in 61% African and 39% Asian participants. Subtype CRF01_AE was almost exclusively seen in Asian participants (98%). Subtypes G and CRF02_AG were exclusively seen in African participants. Two patients carried subtype F, and 1 each carried subtypes A, D, and K. Of 491 patients, 452 (92%) had at least 1 major N(t)RTI mutation and 476 (97%) of patients had at least 1 major NNRTI mutation. The most common N(t)RTI mutation was at M184 (86%) followed by TAMs at codons 215 (28%), 67 (23%), 70 (20%), 219 (18%), and 41 (17%). The most common NNRTI mutation was K103 (52%), followed by Y181 (28%) (Table 1 and Fig. 2).
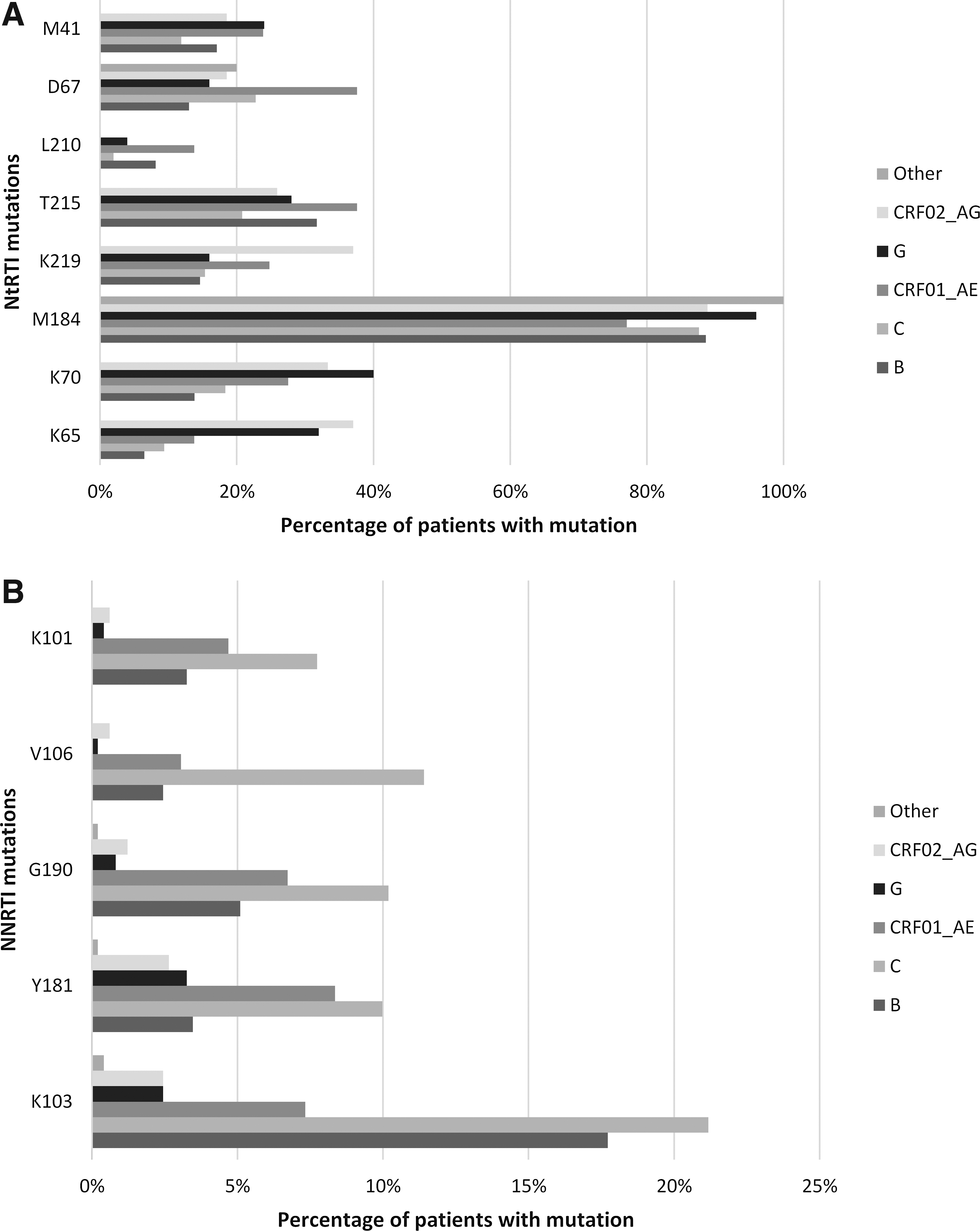
Mutation frequency by subtype. Chart shows the proportion of patients with major
Two hundred ninety (59%) patients had <3 major N(t)RTI mutations. Having ≥3 major N(t)RTI mutations was significantly associated with being infected with subtype CRF01_AE (OR = 2.34, 95% CI = 1.31–4.17, p = .004), a higher SECOND-LINE study baseline VL (OR = 1.39, 95% CI = 1.07–1.78, p = .006), having received TDF as the most recent N(t)RTI (OR = 3.87, 95% CI = 1.97–7.59, p < .001), having a drug other than TDF or a ta-N(t)RTI as the most recent N(t)RTI (OR = 8.35, 95% CI = 1.97–35.45, p = .004), and a longer total time of receiving ta-N(t)RTIs (all quartiles significant compared with first quartile, p < .001; see Table 2). Those with CD4+ cell counts between 200 and 349 cells/mm3 compared with <200 cells/mm3 at SECOND-LINE study baseline were more likely to have <3 mutations (OR = 0.47, 95% CI = 0.29–0.77, p = .003) (Table 2).
Significant results are bold.
Four hundred thirty (88%) patients had <3 TAMs. Having <3 TAMs was significantly associated with subtype C (OR = 0.45, 95% CI = 0.21–0.99, p = .047). Having ≥3 TAMs was significantly associated with higher VL at the time of confirmed first-line VF (OR = 1.62, 95% CI = 1.15–2.29, p = .006), and with a total longer time of receiving ta-N(t)RTIs (p < .001, see Table 3).
Significant results are bold.
One hundred fifty-two (31%) patients had a major N(t)RTI mutation at either K65 or K70. Having either a K65 or K70 mutation was associated with subtypes CRF01_AE (OR = 2.46, 95% CI = 1.26–4.78, p = .008) and G (OR = 4.77, 95% CI = 1.44–15.76, p = .010), and having TDF as part of a recent cART regimen (OR = 8.91, 95% CI = 5.00–15.85, p < .001). Being female (OR = 0.62, 95% CI = 0.38–1.00, p = .049) and having a CD4+ cell count between 200 and 349 cells/mm3 compared with <200 cells/mm3 (OR = 0.43, 95% CI = 0.26–0.73, p = .002) were significantly associated with not having either mutation (Table 4).
Significant results are bold.
Two hundred ninety-one (59%) viruses were classified as being highly responsive to ETV, 156 (32%) as intermediate, and 44 (9%) as reduced. Older age (OR = 0.98, 95% CI = 0.96–1.00, p = .046) and having a CD4+ cell count >200 cells/mm3 (Table 5) were associated with better ETV responses, whereas receiving NVP as the most recent NNRTI was associated with a reduced response compared with those receiving EFV (OR = 2.75, 95% CI = 1.89–4.00, p < .001) (Table 6).
Significant results are bold.
Significant results are bold.
Two hundred seventy-six (56%) viruses displayed resistance to RPV (low-, intermediate, or high-level resistance); 180 (37%) were fully susceptible. Higher degrees of resistance to RPV were associated with subtype CRF01_AE viruses (OR = 2.13, 95% CI = 1.30–3.49, p = .003), having received NVP compared with EFV as the most recent NNRTI (OR = 1.72, 95% CI = 1.22–2.43, p = .002), and being female (OR = 1.47, 95% CI = 1.04–2.09, p = .031) (Table 6).
Patients who were older were less likely to have a major NNRTI mutation (OR = 0.94, 95% CI = 0.89–0.99, p = .015) (Table 7).
Significant results are bold.
Discussion
This study describes the distribution and patterns of HIVDR mutations in a cohort of 491 HIV-1-positive individuals who had failed first-line cART and whose plasma samples underwent successful antiretroviral drug resistance genotyping. Multivariate analysis demonstrated associations with selected mutations that are, on the whole, consistent with prior research findings reported from studies of HIV-1 B subtype viruses. In general, the longer a patient received first-line NNRTI +2N(t)RTI, the more likely they were to select resistance mutations; those displaying a K65 or K70 mutation were more likely to have recently received a TDF-containing first-line ART regimen; and participants with CD4+ cell counts >200 cells/mm3 at first-line VF were less likely to have mutations and more likely to have a better predicted response to ETV than those with lower CD4+ counts at VF.
However, there were a number of findings that were not consistent with current understandings of resistance and its correlates and consequences. Study plasma VL at the time of first-line cART VF was found to be an important predictor for both the number of N(t)RTI mutations and the number of TAMs acquired. Wallis et al. found that the degree of N(t)RTI and NNRTI resistance after first-line failure was associated with higher VL at VF (>1,000 copies/mL) in a non-subtype B cohort (66% C, 18% CRF01_AE). 3 Fofana et al. found that high VL at failure is associated with resistance to abacavir and TDF. 27 Hassan et al. also found high VL (>4 log10 copies/mL) to be associated with higher prevalence of HIVDR in a cohort of first-line VF (>400 copies/mL) patients. 28 This finding is interesting given that it is generally believed that the more mutated the virus, the less replication competent it becomes. If this were true, then one might expect to see an association between highly mutated viruses and lower VLs compared with less mutated viruses or wild-type virus. Our finding, however, should be interpreted with caution. Although participants were instructed to continue to take their failing first-line cART until the baseline study visit, this was not monitored and we, therefore, cannot guarantee that it occurred. If many participants stopped their first-line cART before the baseline visit, then it is possible that the finding merely reflects viral replication in the absence of cART drug pressure. It may also be the case that these participants selected resistance-associated mutations as a direct consequence of poor adherence while receiving their first-line cART, making assumptions about adherence to the failing therapy hazardous. 29
However, the presence of resistance mutations at first-line cART failure does not necessarily result in poorer performance of second-line cART, as seen in an exploratory analysis of the SECOND-LINE dataset. 29 In that study, patients with high degrees of N(t)RTI resistance at baseline did as well as those with little to no resistance, suggesting that factors such as adherence are more important than degree of baseline N(t)RTI resistance in a successful virological response to second-line ART. 29 Furthermore, a recent presentation on the impact of N(t)RTI resistance on second-line therapy performance in the EARNEST study showed clear benefit in PI/N(t)RTI second-line therapy, despite little or no predicted N(t)RTI activity in resistance testing. 30 These results suggest that an earlier switch from a failing first-line regimen and investment in adherence-improving strategies may be favorable over GART implementation in LMIC per se, which is expensive, complex, and difficult to sustain. Simple measurement of the presence or absence of antiretroviral drug in an untimed blood plasma sample at a routine monitoring visit may be a useful and less technologically complicated intervention to monitor adherence and intervene before resistance is selected. 31 Recent research has provided evidence that mobile phone message reminders are highly effective in improving cART adherence and VL suppression in LMIC. 32,33
Being younger was significantly associated with having major NNRTI mutations and worse ETV sensitivity. This result most likely reflects the better cART adherence generally displayed by older people living with HIV-1 and receiving cART. It has been repeatedly shown that older patients are more adherent to cART 34 and that specifically for NNRTIs, mutations are uncommon in highly adherent patients. 35 Hassan et al. found in a rural Kenyan cohort that younger age was a potent risk factor for VF and HIVDR development. 28
Our results also suggest that the propensity for HIVDR mutations of the various HIV-1 subtypes may not always be consistent with knowledge derived from subtype B. Subtype CRF01_AE was significantly associated with having ≥3 major N(t)RTI mutations compared with subtype B. This is a concern for South East Asian LMIC, where the CRF01_AE subtype is dominant and there is expanding cART use. 11 Other factors, for which data were unavailable, may have contributed to this result, such as adherence, drug availability, and frequency and type of monitoring available to these patients.
Subtype C was less likely to be associated with having ≥3 TAMs compared with subtype B. This finding is consistent with the hypothesis that subtype B may be more likely to generate TAMs due to frequent pausing at codon 67, leading to D67N mutations and TAMs. 36,37 There is broad evidence suggesting that subtype C has a higher propensity to select for the K65R mutation. 13,14,36,37 However, our results suggest that subtypes CRF01_AE and G may have a greater propensity to select either K65 or K70 mutations.
The strongest predictor of a K65 or K70 mutation was whether a participant took TDF as part of their most recent cART regimen before screening. This is consistent with our knowledge of the association between TDF use and selection of these signature mutations. 38,39 The 2013 WHO guidelines recommend the use of ta-N(t)RTIs plus 3TC as the preferred N(t)RTI-containing second-line cART regimen. 2 Our results support this recommendation given that the associations we found for 3 non-B subtypes were believed to have greater propensity for selection of TDF-associated mutations. However, with d4T having fallen out of favor as a result of its toxicity, AZT is the preferred ta-N(t)RTI. Anemia and other well-described AZT-associated adverse effects (headache, gastrointestinal disturbance, lipoatrophy) may well become problematic, as the use of AZT increases in people switching to second-line cART. A recent study examining the possibility of AZT dose reduction from a 600 mg bid dose to a 400 mg total daily dose was not promising in this regard. 40 The SECOND-LINE study has shown that ritonavir-boosted lopinavir plus raltegravir is a reasonable, efficacious, and safe alternative to recycling N(t)RTIs in second-line cART, 23,41 and this result has been confirmed by both the EARNEST and ACTG 5273 studies. 41,42
Those receiving an NVP-containing regimen before screening had a poorer predicted response to ETV and higher resistance to RPV compared with those on EFV-containing regimens. NVP selects for both Y181C and G190A, affecting susceptibility to both ETV and RPV 43 ; whereas the K103 mutation associated with EFV use does not. Some studies have shown a relationship between receiving NVP in failing regimens, leading to the selection of resistance mutations and compromising the efficacy of ETV. In both a Thai cohort of mostly CRF01_AE subtypes and a Nigerian cohort of various non-B subtypes, there was an association between failing NVP-containing regimens and sub-optimal predicted ETV activity. 44,45 A study of a similar cohort of virologically failing (not virologically monitored) people with HIV in South Africa among whom 89% were taking EFV found that only 9% had selected for ETV resistance. 43 Given this, EFV may be the more appropriate first-line NNRTI choice in settings in which there is no capacity to detect early VF by resistance testing. Further research into the rate of EFV resistance mutation development may help guide timing of VL tests in LMIC to help patients get therapeutic value from ETV in third-line cART (the WHO recommendation is for boosted darunavir+raltegravir+etravirine ± N(t)RTIs).
Our study has limitations. It is a cross-sectional study and, therefore, inferences about causality on the basis of associations should only be made with caution. In some cases, the possibility of reverse causality should be considered. Our results may be affected by data that were not collected, such as baseline patient demographic status, participants’ adherence to their first-line cART or how long they had been failing treatment before enrolment in SECOND-LINE. Statistically, there are weaknesses with regard to some small cell sizes, increasing the likelihood of making Type II errors. Furthermore, we performed a relatively large number of statistical tests, increasing the probability of finding spurious associations. A Bonferroni analysis was performed (Supplementary Table S1; Supplementary Data are available online at
Conclusion
Our study has generally given results that are consistent with our knowledge of HIV-1 resistance characteristics made on the basis of studies of subtype B. Higher VL at identification of VF and more time spent on treatment increased the likelihood of having mutations, whereas those with higher CD4 cell counts at identification of VF were less likely to have mutations. However, there are some novel and interesting differences between subtypes. Subtype CRF01_AE was associated with more N(t)RTI and RPV resistance, and subtype C was associated with less ta-N(t)RTI resistance. Subtypes CRF01_AE and G were more likely to select for K65 or K70 mutations. The WHO currently recommends TDF-based regimens for all first-line regimens (EFV+TDF +3[F]TC single tablet preferred). Therefore, in light of these results, ta-N(t)RTI +3TC as the second-line 2N(t)RTI backbone seems an appropriate choice, as this backbone combination would most likely retain antiretroviral activity. The nucleoside-sparing boosted-PI plus raltegravir regimen is also an efficacious and safe second-line cART alternative and would avoid the adverse effects of ta-N(t)RTIs. The results also support current recommendations to commence cART at higher CD4 T-cell counts, at which point the selection of resistance-associated mutations is less likely. Further research is needed in the development of cheap and reliable point-of-care testing and to clearly determine whether virological testing is genuinely required to optimize the prescription and use of cART worldwide.
Footnotes
Acknowledgments
The authors are grateful to the SECOND-LINE study participants and their partners, families, and caregivers for their participation in the study. They also thank all the staff from all centers for participating in the trial. Sequence data: GenBank Accession Numbers: KR867736–KR868227.
SECOND-LINE Study Group
Author Disclosure Statement
MB has received grants and personal fees from Merck, AbbVie, Gilead and ViiV Healthcare; PC, grants from Gilead, GlaxoSmithKlein, MSD Pharmaceuticals, and NIAID; DC, grants from AbbVie and Merck, Sharp & Dohme; SE, grants from Merck Research Laboratories and AbbVie; J-MM, grants from Merck and Gilead and is on the advisory boards for Gilead, Merck, ViiV, BMS and Janssen; HT, is an employee of Merck (MSD); JvW is an employee of AbbVie Inc, and holds stock and/or stock options in the company. All other authors have no conflicts of interest.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.