
Abstract

H
We describe three HIV-positive patients on elvitegravir/cobicistat/tenofovir/emtricitabine who received lumbar punctures for persistent headache in the absence of other neurological complaints (and with normal brain CT scans). After obtaining written informed consent (allowing the procedure, drug measurement, and potential anonymous data publication), CSF was withdrawn using atraumatic needles. Recent adherent was reported to be above 90% of prescribed doses and the last dose was administered under direct observation. Beside biochemical and virological examinations, CSF was tested for albumin levels; antiretroviral plasma and CSF concentrations (on samples collected <15 min apart) were measured by validated ultra-performance liquid chromatography tandem mass-spectrometry methods [with lower limits of quantification of 11.7 ng/ml (plasma) and 0.125 ng/ml (CSF)].
Patient A was a middle-aged female with body mass index (BMI) of 27.5 kg/m2; her CD4 cell count and plasma HIV RNA were 441 cells/μl and <20 copies/ml, respectively. Patient B was a male in his 40s (BMI of 26.4 kg/m2) with a previous diagnosis of disseminated cryptococcosis without meningeal involvement; his CD4 cell count and plasma HIV RNA were 46 cells/μl and <20 copies/ml, respectively. In these two subjects, the onset of headache was unrelated to the introduction of elvitegravir/cobicistat/tenofovir/emtricitabine.
Patient C was a young male in his 30s (BMI of 22.2 kg/m2) with a previous diagnosis of cytomegalovirus retinitis; 2 months after starting elvitegravir/cobicistat/tenofovir/emtricitabine plus atazanavir (300 mg once daily), he complained of persistent headache. His CD4 cell count and plasma HIV RNA were 75 cells/μl and 395 copies/ml. All subjects had a normal renal function with estimated creatinine clearances of 112.1, 86.3, and 103.2 ml/min.
CSF samples were negative for causes of encephalitis, contained no cells, and showed normal protein levels; CSF serum albumin ratios were within age-corrected range, representing normal blood–brain barriers. CSF HIV RNA was 56, <20, and 71 copies/ml, respectively.
Plasma and CSF concentrations (in ng/ml) as well as CSF-to-plasma ratios are summed up in Figure 1. In patient C, atazanavir plasma and CSF concentrations were 692 and 36 ng/ml, respectively; CSF-to-plasma ratio was 0.05. Tenofovir and emtricitabine CSF-to-plasma ratios were, respectively, 0 (0–0.07) and 0.51 (0.37–0.76); in two out of three samples, CSF tenofovir was not detectable.
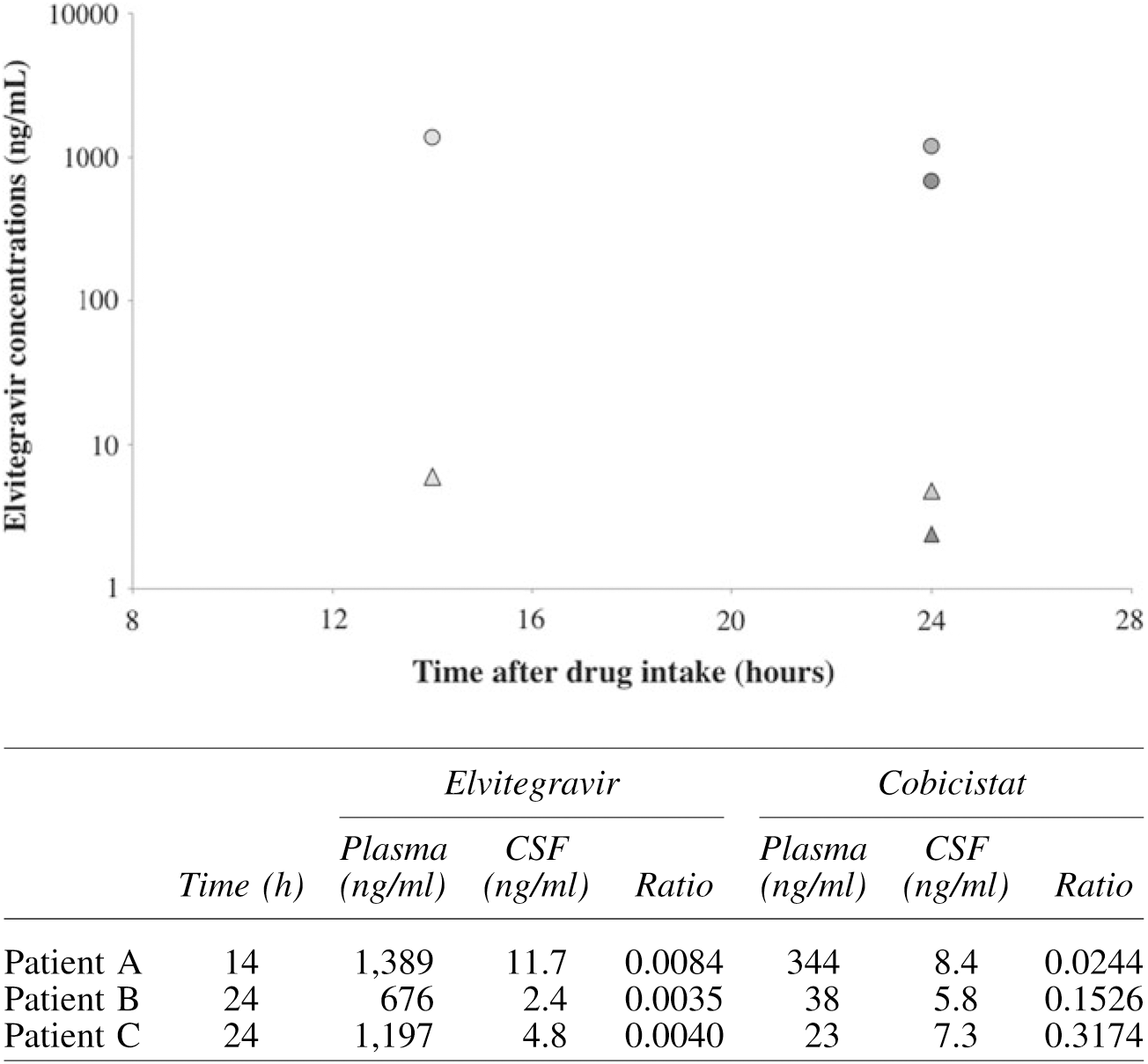
Elvitegravir concentrations in plasma (circles) and CSF (triangles) and cobicistat concentrations (table underneath). The graph is semilogarithmic. CSF, cerebrospinal fluid.
In this case series, we describe elvitegravir and cobicistat CSF concentrations. Elvitegravir levels ranged from 2.4 to 11.7 ng/ml (14–24 h after drug intake), with one trough sample being below in vitro non protein-adjusted 50% effective concentration (3.9 ng/ml). 8 Elvitegravir CSF concentrations were 0.3% (0.4–0.8) of plasma levels. In patient C, higher elvitegravir trough may be due to the concomitant administration of atazanavir, yet this did not influence elvitegravir CSF exposure, which was comparable to that of patient B. Cobicistat exposure in the CSF was highly variable with concentrations ranging from 2% to 31% of plasma ones. We cannot extend these observations to other subjects nor judge the pharmacodynamic of elvitegravir in the CNS, given the inter-patient variability and the differences between plasma and CSF pharmacokinetic profiles. CSF HIV RNA was either well controlled or lower than plasma level in two out of three patients and detectable at very low level in the third patient (56 copies/ml). Pooled data from tenofovir/emtricitabine/elvitegravir/cobicistat-treated patients suggested that the drugs distribute into the CNS because several participants (11%–12%) reported somnolence, headache, dizziness, insomnia, or abnormal dreams. 7,8 Raltegravir and dolutegravir (the two other commercially available integrase inhibitors) were associated with CSF levels above 50% inhibitory concentrations in the majority of patients, but with a significant inter-patient variability. 9,10
In conclusion, to the best of our knowledge, these are the first data concerning the penetration of elvitegravir/cobicistat in the CSF: prospective studies are currently ongoing to establish the appropriateness of the drugs' compartmental exposure.
Footnotes
Acknowledgment
This work was supported by internal funding.
Author Disclosure Statement
A.C. has received grants, travel grants, and speaker's honoraria from Abbvie, Bristol-Myers Squibb (BMS), Gilead, Merck Sharp & Dohme (MSD), Janssen-Cilag, Viiv. S.B. has received grants, travel grants, and consultancy fees from Abbott, Boehringer-Inghelheim, BMS, Gilead-Sciences, GSK, MSD, Pfizer, and Janssen-Cilag. G.D.P. has received grants, travel grants, and consultancy fees from Abbott, Boehringer-Inghelheim, BMS, Gilead-Sciences, GSK, MSD, Pfizer, Roche, and Tibotec (Johnson & Johnson). Other authors have no competing financial interests.