
Abstract
The human T cell lymphotropic virus type 1 (HTLV-1) is the etiologic agent of HTLV-1-associated myelopathy/tropical spastic paraparesis (HAM/TSP). HTLV-1 infected individuals have increased susceptibility to Mycobacterium tuberculosis infection but the influence of tuberculosis (TB) on the course of HTLV-1 infection is unknown. The aim of this study was to evaluate the influence of TB on immunological, virologic, and neurologic features of HTLV-1 infection. This is a retrospective analysis of individuals enrolled in a cohort study from an HTLV-1 clinic who were evaluated for past or latent tuberculosis (LTB) and classified clinically as HTLV-1 carriers, probable HAM/TSP and definite HAM/TSP. Spontaneous cytokine production (interferon-gamma [IFN-γ], tumor necrosis factor [TNF], and interleukin[IL]-10), serum chemokines (CXCL9 and CXCL10) and HTLV-1 proviral load were evaluated. Of 172 participants, 64 did not have histories of TB (TB- group), 81 had LTB and 27 had TB in the past (TB+ group). In the TB+ group, there was a higher frequency of HAM/TSP patients (35%) than in HTLV-1 carriers (10%) (OR = 3.8, p = .0001). HAM/TSP patients with histories of TB had higher IFN-γ/IL-10 and TNF/IL-10 ratios when compared with HAM/TSP patients without histories of TB. There were no differences in serum chemokine production and proviral load across TB groups stratified on HTLV-1 clinical status. In conclusion, TB may influence the development of HAM/TSP, and patients with these two diseases have an impairment in the modulation of immune response.
Introduction
T
HTLV-1 induces a spontaneous cell proliferation and high production of proinflammatory cytokines, such as interferon-gamma (IFN-γ) and tumor necrosis factor (TNF). 10 Unstimulated peripheral blood mononuclear cells (PBMC) from HAM/TSP patients produce more proinflammatory cytokines than cells from HTLV-1 carriers, but IL-10 and IL-5 are detected in cell cultures of both groups of patients. 10,11 Since IL-10 modulates inflammatory response, IL-10 production could be related to the maintenance of the clinical status of HTLV-1 carriers. 12 This hypothesis was supported by an in vitro study that showed that the addition of exogenous IL-10 in cell cultures from HTLV-1 carriers decreased the IFN-γ production, which was not observed in cell cultures from HAM/TSP patients. 13,14 Proinflammatory chemokines CXCL9 and CXCL10 are also spontaneously produced by HAM/TSP patients and HTLV-1 carriers. But higher levels of CXCL9 and CXCL10 are detected in serum and cerebrospinal fluid from HAM/TSP patients when compared with HTLV-1 carriers. 13,15,16
The immunological abnormalities observed in HTLV-1-infected individuals may lead to increased susceptibility to acquiring other infectious diseases such as strongyloidiasis, 17,18 severe scabies, 19 and tuberculosis (TB). 20 –22 According to the Ministry of Health from Brazil, the country has the eighteenth highest number of TB cases worldwide. Thus, Brazil is endemic area for both HTLV-1 and Mycobacterium tuberculosis infection.
Few studies have focused on HTLV-1 and TB coinfection. Pedral-Sampaio et al. demonstrated that there was a high prevalence (8.5%) of HTLV-1 infection in individuals diagnosed with TB; furthermore, HTLV-1 infection was associated with increased risk of M. tuberculosis infection and disease severity. 21 In Peru, it was reported that HTLV-1/TB-infected individuals have higher death rates due to TB than TB patients without HTLV-1. 22 Additionally, in a population where HTLV-1 and TB are prevalent, HTLV-1 infection may increase the susceptibility to active TB. 23 Recently, in a study performed in an infectious diseases hospital in Salvador, Bahia, 10% of TB patients were found to be coinfected with HTLV-1. 20 These studies show that there is an association between HTLV-1 and TB, and this association may lead to a worse prognosis in TB patients. 24 However, there are no studies evaluating the potential influence of TB on the clinical status of HTLV-1 infection. In this study, we evaluated the associations between TB status with immunological and virological features in HTLV-1 infected individuals with and without neurological symptoms. We hypothesized that TB influences the clinical status, immune response, and proviral load in HTLV-1 infection.
Materials and Methods
Study design and population
This is a retrospective analysis of HTLV-1-infected individuals from the HTLV-1 Clinic at the Hospital Universitario Professor Edgard Santos, Federal University of Bahia, Salvador, Bahia, Brazil. The diagnosis of HTLV-1 was performed by enzyme-linked immunosorbent assay (ELISA) (Murex Biotech Limited, Dartford, United Kingdom) and confirmed by western blot (HTLV blot 2.4; Genelabs, Singapore). Since 2004, we have conducted a cohort study within our HTLV-1 Clinic. Determination of IFN-γ, TNF, IL-10, CXCL9, and CXCL10 along with HTLV-1 proviral load from HTLV-1-infected individuals is performed at the time of enrollment in the clinic as detailed below. Serum samples from these individuals are collected and stored at −20°C.
The inclusion criteria were male and female patients 18 to 70 years old who had available data on TB status. The exclusion criteria were patients coinfected with HIV, autoimmune diseases, other confounding chronic diseases, and use of corticosteroids.
The clinical status of HTLV-1 infection was classified as follows: (1) HTLV-1 carriers: infected individuals without neurological symptoms, Expanded Disability Status Scale (EDSS) = 0 (zero) 25 , and Osame's motor disability score (OMDS) = 0 (zero) 26 ; (2) Probable HAM/TSP: HTLV-1-infected individuals who did not fulfill the criteria for HAM/TSP (EDSS ≤2.5 and OMDS = 0) but presented with urgency in the absence of urinary tract infection along with detrusor overactivity in the urodynamic study 27 ; (3) HAM/TSP: patients who fulfill criteria for HAM/TSP according to the World Health Organization criteria (EDSS >2.5 and OMDS > 0).
For this study, HTLV-1 carriers, probable HAM/TSP and HAM/TSP patients were evaluated for history of M. tuberculosis infection. HTLV-1-infected individuals who did not have evidence of active or history of TB and had negative tuberculin skin tests (TST) were classified as TB negative. Patients who had positive TST but no history of TB were classified at the latent TB group (LTB). Most patients from the LTB group had a TST greater than or equal to 10 millimeters (mm), which generally suggests exposure to M. tuberculosis. Those patients who had a history of TB with documentation of acid fast bacilli in the sputum were classified as TB+. All TB patients received and were cured after multidrug chemotherapy for TB. Additionally, all of them had a positive TST, and radiologic features of TB were present in 23 (85.1%) of the cases.
Informed consent was obtained from all individuals and the Institutional Review Board of the Federal University of Bahia approved this project.
PBMC culture
Fresh PBMC were isolated from heparinized blood samples by density gradient centrifugation using Ficoll-Hypaque (GE Healthcare Bio-sciences, Uppsala, Sweden). A total of 3 × 106 cells/ml were cultured without stimulation in RPMI 1640 (Life Technologies Gibco BRL, Grand Island, NY), 10% serum fetal bovine (Sigma, St. Louis, MO), glutamine, HEPES, and antibiotics for 72 h at 37°C with 5% CO2. Supernatant fluids were collected and stored at −20 oC for cytokine assays.
Measurement of cytokines and chemokines
ELISA was used to measure the spontaneous production of IFN-γ, TNF, and IL-10 from supernatant fluids. The serum chemokines CXCL9 and CXCL10 were measured by ELISA. The reagents were purchased from BD Bioscience Pharmingen (San Jose, CA). The results were expressed as pg/ml based on a standard curve.
Determination of HTLV-1 proviral load
DNA extraction was performed as previously described. 13 The HTLV-1 proviral load was quantified using a real-time TaqMan polymerase chain reaction method. 28 Amplification and data acquisition were carried out using the ABI Prism 7700 Sequence detector system (Applied Biosystems). The normalized value of the HTLV-1 proviral load was calculated as the ratio of (HTLV-1 DNA average copy number/albumin DNA average copy number) × 2 × 106. 13 The data were expressed as the number of HTLV-1 DNA copies/106 mononuclear cells.
Statistical analysis
The Chi-square test was used to compare the gender distribution between the three groups (TB−, LTB, and TB+), the frequency of HTLV-1 carriers, probable HAM/TSP and HAM/TSP patients with history of TB (TB+ group).
The one-way analysis of variances was used to compare the age distribution. The Kruskal–Wallis test with post-test was used to compare cytokine and chemokine production and HTLV-1 proviral load.
To evaluate the association between TB status and HTLV-1 clinical status and to assess potential confounders, we performed ordinal logistic regression considering the dependent variable of clinical status of HTLV-1 infection (HTLV-1 carrier, probable HAM/TSP and HAM/TSP) as ordinal data. The odds ratios from these models approximated the risk of having a clinical state that is one category higher (i.e., more severe) as a result of the defined increase in a continuous independent variable or a change from “no” to “yes” in a dichotomous independent variable.
Analyses were done with GraphPad Prism 5 (San Diego, CA) and STATA version 10 (StataCorp, College Station, TX) and a p-value < .05 was considered to be statistically significant.
Results
A total of 172 HTLV-1-infected individuals were enrolled into this study. All of them were evaluated for history of TB. Sixty-four subjects were considered as TB negative (negative TST and no history of TB); 81 were LTB (positive TST, no history of TB, and negative chest radiography); and 27 had a history of TB (Table 1). The female/male frequency was 52/12 in the TB- group; 47/34 in the LTB group; and 14/13 in the TB+ group (p = .004). Comparing the age distribution of the three groups, the patients with history of TB were older than patients from TB- group (56 ± 10 and 50 ± 12.3 years; p = .04) (Table 1). The diagnosis of TB was made before the diagnosis of HAM/TSP, for all but one case. There was a gap of 5.8 ± 8.28 years (mean ± standard deviation) between the diagnosis of TB and HAM/TSP.
Chi-square test.
Difference between TB− and TB+ (ANOVA).
Nonparametric test for trend (of HTLV-1 status) across TB groups
HAM/TSP = HTLV-associated myelopathy/tropical spastic paraparesis. Odds ratio = 3.8; 95% confidence interval 1.9, 9.1 by ordinal logistic regression with HTLV-1 clinical status as the outcome.
ANOVA, analysis of variance; HAM, HTLV-1-associated myelopathy; HTLV-1, human T cell lymphotropic virus type 1; TB, tuberculosis; TSP, tropical spastic paraparesis.
Frequency of HTLV-1 clinical status in TB+ group
Table 1 summarizes the frequency of the clinical forms of HTLV-1 infection by TB status. Using ordinal logistic regression with HTLV-1 clinical status as an ordinal outcome, a history of TB was associated with increased odds of having HAM/TSP relative to those with no history of TB (OR 3.8; 95% CI 1.9–9.1, p = .0001). There was no difference in risk associated with having latent TB relative to no history of TB (OR 0.97; 95% CI 0.50–1.9, p = .94). Models incorporating age and gender as potential confounders, neither of which was statistically significant, yielded similar results (data not shown).
Spontaneous cytokine production
Among the HTLV-1 carriers, there was no difference in spontaneous cytokine production when we compared across the three study groups (TB−, LTB, and TB+). The same result was seen regarding probable HAM/TSP and HAM/TSP patients across the three TB groups.
Since IL-10 regulates proinflammatory cytokine production, we evaluated the ratio between IFN-γ and IL-10 (IFN-γ/IL-10) production and the TNF/IL-10 ratio.
Among the HTLV-1 carriers, the median IFN-γ/IL-10 ratio in the TB- group was 39.4 (interquartile range [IQR] 16–419), compared with 33.9 (5–447) in the LTB group and 84 (6–447) in the TB+ group, (p = .8) (Fig. 1A). There was no statistical difference between the three groups when we compared the TNF/IL-10 ratios: 8.6 (1–156) for TB−; 8.8 (1–106) for LTB; and, 25.6 (0.6–303) for TB+ group (Fig. 1B).
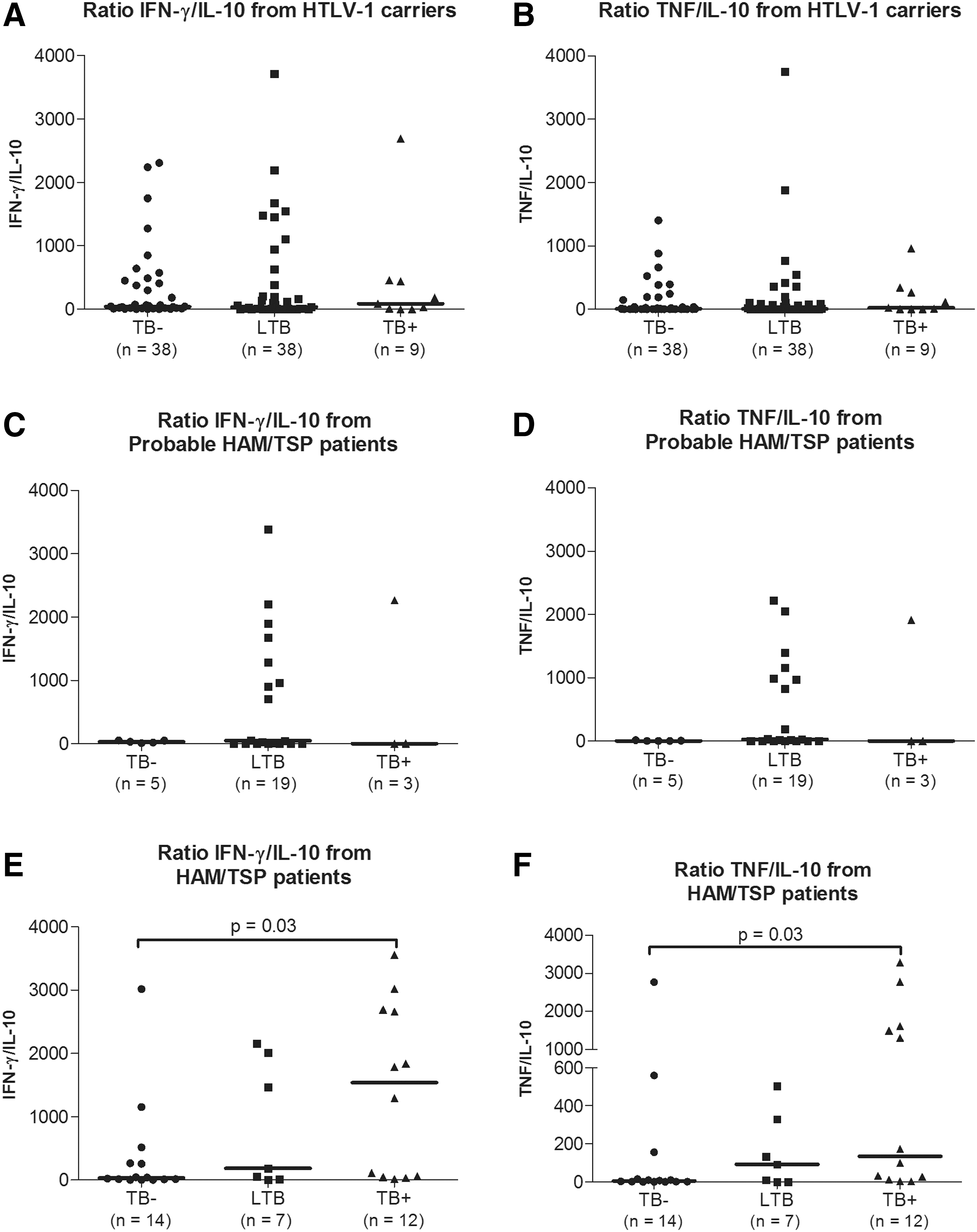
IFN-γ/IL-10 and TNF/IL-10 ratios from HTLV-1 carriers, probable HAM/TSP and HAM/TSP patients. The cytokine ratios are calculated with values of spontaneous cytokine production from HTLV-1 carriers
Among probable HAM/TSP patients, the IFN-γ/IL-10 ratios were 30.9 (13.9–52) in TB− group; 48.7 (1–1285) in LTB group; and 5.0 (1–2264) in TB+ group (p = .9) (Fig. 1C). Regarding TNF/IL-10 ratios, there was no difference between the three groups (p = .2): 1.0 (0.6–12.7) in TB− group; 26.9 (1–990) in LTB group; and 1.0 (1–1911) in TB+ group (Fig. 1D).
Among the HAM/TSP patients, the IFN-γ/IL-10 ratio tended to increase across the TB status groups: 34.3 (9–328) for TB−; 184 (15–2015) for LTB; and 1537 (53–2685) for TB+. The difference between TB− and TB+ groups was statistically significant (p = .03) (Fig. 1E). A similar result was seen at TNF/IL-10 ratio: 4.8 (1–50) for TB−; 92 (0.9–329) for LTB; and 136 (15–1583) for TB+ (p = .02 for the comparison between TB− and TB+ groups) (Fig. 1F).
Serum chemokine production
Serum CXCL9 levels (Fig. 2A) and CXCL10 levels (Fig. 2B) from HTLV-1 carriers did not differ across the three groups (TB−, LTB, and TB+). Similar patterns of serum CXCL9 and CXCL10 levels were seen in subjects with HAM/TSP (Fig. 2E, F) stratified by TB status. Among probable HAM/TSP patients, there was no difference in CXCL9 production in those three groups (Fig. 2C). However, probable HAM/TSP patients from the TB− group produced more CXCL10 (499 pg/ml [271–1880]) than the LTB group (225 pg/ml [129–336]) (p = .04) (Fig. 2D).

Serum chemokine production from HTLV-1 carriers, probable HAM/TSP and HAM/TSP patients. The serum CXCL9 and CXCL10 levels were evaluated in HTLV-1 carriers
HTLV-1 proviral load
Proviral load from HTLV-1 carriers (Fig. 3A), probable HAM/TSP (Fig. 3B) and HAM/TSP subjects (Fig. 3C) did not differ by TB status.
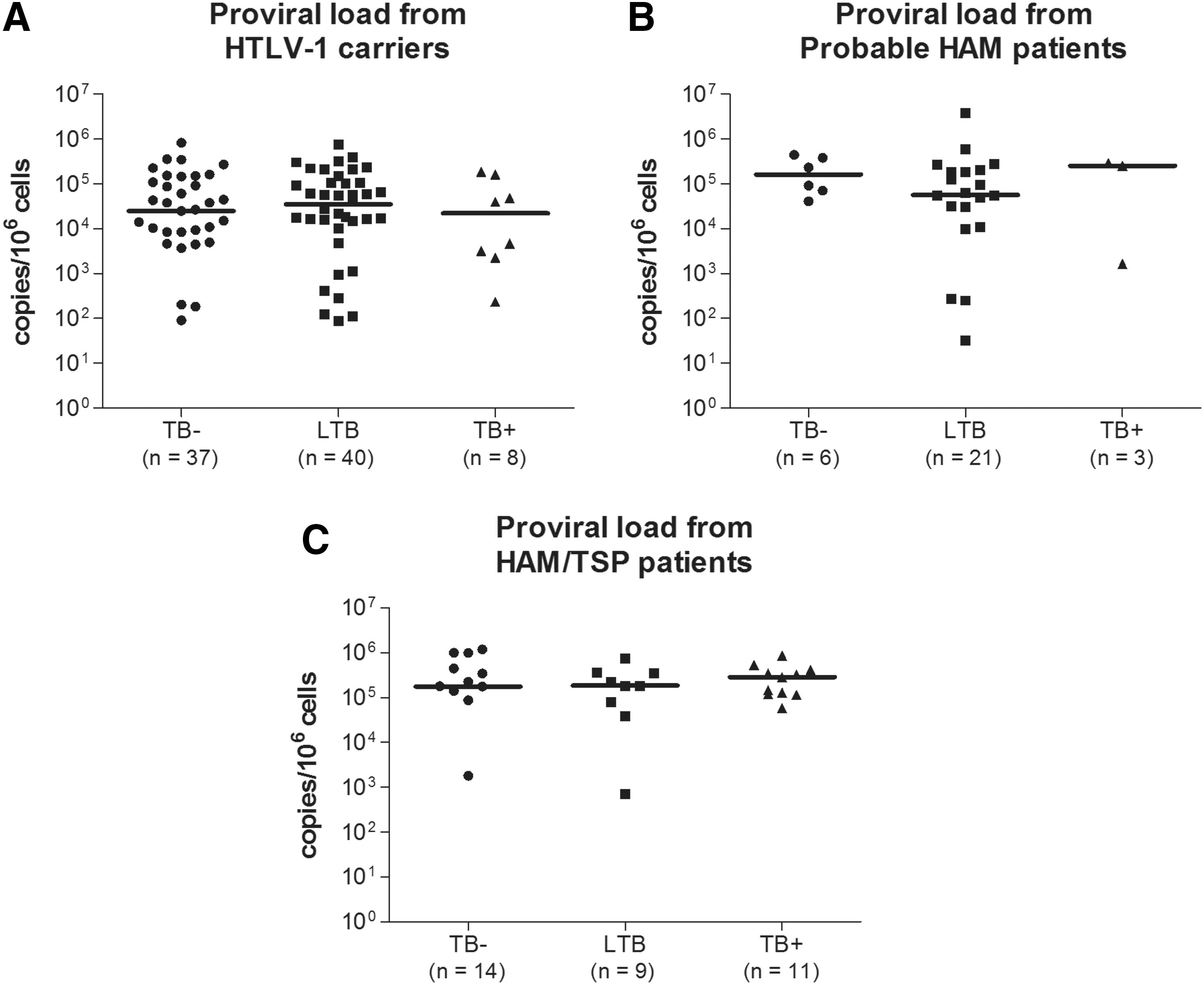
Proviral load determination in HTLV-1 carriers, probable HAM/TSP and HAM/TSP patients. The proviral load was determined in HTLV-1 carriers
Discussion
Patients with HAM/TSP have a higher proviral load and higher production of proinflammatory cytokines than HTLV-1 carriers, and proviral load is considered a marker of HAM/TSP. In this study we found a strong association between prior history of TB and the presence of HAM/TSP. Furthermore, our exploratory analysis of spontaneous cytokine production by PBMC showed that HAM/TSP patients with histories of TB had higher TNF/IL-10 and IFN-γ/IL-10 ratios than HAM/TSP patients without TB. This indicates an imbalance between proinflammatory and regulatory cytokines, which may contribute to the development of severe CNS disease in patients with TB coinfected with HTLV-1.
Prior studies suggest that HTLV-1-infected individuals are at high risk of acquiring M. tuberculosis infection. 20,22,23,29 Initially, studies in the United States and Japan showed that HTLV-1 carriers had low delayed type hypersensitivity response to PPD (purified protein derivative from M. tuberculosis) compared with seronegative individuals. 30,31 In addition, an in vitro study conducted by Mascarenhas et al. demonstrated that mononuclear cells from HTLV-1-infected individuals did not proliferate when stimulated with PPD. 32 These observations raised the possibility that HTLV-1 carriers are at higher risk of acquiring TB. Moreover, coinfection with HTLV-1 and M. tuberculosis was associated with higher mortality compared with patients with only TB. 21 Although we have documented the association between TB and HTLV-1 infection in two previous studies, we have not detected any impairment in the response to TST among HTLV-1-infected patients in either study. 20,33 Herein the TST was positive in all patients with histories of TB and also in a large percentage of HTLV-1 without histories of TB. Additionally, we have previously shown that TST is better than interferon-gamma release assay (IGRA) in detecting exposure to M. tuberculosis in HTLV-1-infected individuals (unpublished data).
As HTLV-1 infection is associated with upregulation of Th1-type immune responses, 10,34,35 it would be logical that this response would be protective against TB. Nevertheless, the decreased PPD-specific TNF production and high levels of proinflammatory cytokines could lead to greater severity of TB in coinfected patients. 33 In the present study, we evaluated the potential influence of TB on HTLV-1 infection. Since the exacerbated proinflammatory cytokine/chemokine production is also related to the immune response in HAM/TSP patients, M. tuberculosis infection might influence the clinical and immunological features of HTLV-1 infection. We observed no difference in spontaneous TNF, IFN-γ, and IL-10 production between the groups of subjects categorized by TB status. If we compare the extreme ends of clinical status of HTLV-1 infection (carriers and HAM/TSP), we observed that, even with high IFN-γ and TNF production in HAM/TSP patients, there was a low IL-10 production in these patients. Among HTLV-1 carriers and probable HAM/TSP patients, IFN-γ/IL-10 and TNF/IL-10 ratios did not differ by TB status. However, among HAM/TSP patients, these ratios were higher in patients with histories of TB compared with the TB negative group. These results suggest that HAM/TSP patients with histories of TB may have an impairment in the downmodulation of the inflammatory response, which may contribute to tissue damage in the CNS and consequently myelopathy. 2 This lack of modulation has been previously documented, since the exogenous addition of IL-10 in mononuclear cell culture from HAM/TSP patients did not decrease the IFN-γ production. 13,14
It is known that the chemokines CXCL9 and CXCL10 are found in high levels in cerebrospinal fluid and serum from HAM/TSP patients, and they may be potential biomarkers for the neurological injury seen in these patients. 13,16 In the present study, we evaluated serum concentrations of CXCL9 and CXCL10 in the three groups based on TB status, but we did not find any difference between them with the exception of CXCL10 production in probable HAM/TSP, where individuals with no history of TB produced more CXCL10 than probable HAM/TSP patients with LTB. This latter difference may be due to the outliers observed in the TB-negative group. Thus, TB may have no influence on serum chemokine production in HTLV-1 patients.
The high HTLV-1 proviral load has been considered the main risk factor for developing HAM/TSP in HTLV-1-infected subjects. 36 –38 We found no relationship between TB status and proviral load among both HTLV-1 carriers and patients with HAM/TSP. A limitation of our study was not knowing the exact time that each HTLV-1-infected subject acquired HTLV-1 infection. Since most of our patients did not receive blood transfusions, however, we believe that the majority of these patients acquired HTLV-1 through breastfeeding or sexual contact. An additional limitation is that cultures for M. tuberculosis were performed in only a few patients. We clearly showed, however, that the diagnosis of TB preceded the diagnosis of HAM/TSP, and there was an association between TB and HAM/TSP. Additional studies that include clinical and radiological evaluations for TB should be done in HTLV-1-infected patients to confirm the results presented here. Moreover, prospective, longitudinal evaluation of HTLV-1-infected subjects with TB would clarify the potential relationship between this exposure and the course of HTLV-1 infection.
In conclusion, our data suggest that history of TB may be a risk factor for development of HAM/TSP. Our observation of a higher IFNγ/IL-10 and TNF/IL-10 ratios in HAM/TSP patients with history of TB suggests that an impairment in the modulation of the inflammatory responses is one of the factors that may contribute to development of HAM/TSP in patients coinfected with TB and HTLV-1.
Footnotes
Acknowledgments
We are grateful to Cristiano Franco for his secretarial assistance.
We are grateful to Dr. Daniel Fitzgerald and Dr. Warren Johnson from Weill Cornell Medical College for their scientific contributions to this work.
The CNPq (Brazilian Council for Scientific and Technological Development), NIH R01 AI079238, and ICOHRTA (International Clinical, Operational and Health Service Research and Training Award) funded this work.
Author Disclosure Statement
The authors declare no conflicts of interest.