
Abstract
The objective of this study was to determine the virological response and the possible emergence of drug resistance at 1 and 2 years postpartum in HIV-positive pregnant women enrolled under the Option B approach and meeting the criteria for treatment. In the study, women with baseline CD4+ <350/mm3 received a combination of stavudine, lamivudine, and nevirapine during pregnancy (from week 25 of gestation) and continued it indefinitely after delivery. HIV-RNA was measured at 12 and 24 months postpartum. Drug resistance mutations were assessed in those with HIV-RNA >50 copies/ml. Baseline resistance mutations were assessed in the entire cohort. A total of 107 women were studied. At baseline, resistance mutations were seen in 6.6% of the women. At 12 months, 26.7% of the women had >50 copies/ml and among them 12.9% had virological failure (HIV-RNA >1,000 copies/ml). At 24 months, detectable HIV-RNA was seen in 28.3% of the women and virological failure in 10.1% of the women. Resistance mutations (mainly non-nucleoside reverse transcriptase inhibitors mutations) were seen in 40% of the women with detectable HIV-RNA. Baseline mutations did not correlate with virological failure or the emergence of resistance at later time points. Virological failure 2 years postpartum and emergence of resistance were rare in this cohort of HIV-infected women. These findings are reassuring in the light of the new strategies for the prevention of mother-to-child HIV transmission, recommending life-long antiretroviral therapy administration.
Introduction
L
For these reasons, we conducted a study to evaluate in a cohort of women receiving life-long antiretroviral therapy meeting the criteria for treatment (CD4+ lymphocyte count <350/mm3 at the time of the study under an Option B approach), the virological response at 1 and 2 years postpartum and the possible associated emergence of resistance. We also evaluated baseline resistance in the entire cohort since studies have shown a significant association between pretreatment resistance and subsequent virological failure and emergence of mutations. 5 –7
Materials and Methods
We studied HIV-infected pregnant women enrolled in an observational study aimed to assess safety and pharmacokinetics of antiretroviral administration in breastfeeding women [SMAC (Safe Milk for African children) study]. 8,9 The study was conducted in Malawi within the structures of the DREAM (Drug Resource Enhancement against AIDS and Malnutrition) program of the community of S. Egidio, an Italian faith-based nongovernmental organization and received ethical approval by the National Health Research Committee (Approval No. 486). In the study conducted between 2008 and 2011, women meeting the criteria for treatment (CD4+ lymphocyte count <350/mm3) started stavudine, lamivudine, and nevirapine (d4T/3TC/NVP, first-line recommended regimen at the time of the study in Malawi) after the first trimester of pregnancy, and continued treatment indefinitely after delivery (with 6 months of breastfeeding). Women developing nevirapine toxicity were switched to a lopinavir-containing regimen. Clinical visits were scheduled monthly during the first 12 months after delivery, then every 3 months until 24 months postpartum. CD4+ lymphocyte count and viral load were measured locally every 6 months and the information was available to the treating physicians. No drug resistance assessment was performed locally. Information about drug adherence was not available. However, the proportion of missed clinical visits during follow-up was used as a marker of treatment adherence. Peer community health workers assisted patients through home-care visits and treatment adherence counseling. 10
Virological analyses
Plasma samples were stored frozen at −80°C after collection and then shipped in dry ice to the laboratory of the Istituto Superiore di Sanità where they were analyzed. Viral load was measured using the Versant kPCR assay (Siemens Healthcare Diagnostics, Deerfield, IL) at baseline, and at 12 and 24 months after delivery. Presence of drug resistance mutations was assessed by the use of the TruGene Genotyping kit (Siemens Healthcare Diagnostics) at baseline and in patients with detectable HIV-RNA (>50 copies/ml) at 12 and 24 months postpartum. Resistance mutations were classified according to the 2013 IAS-USA classification.
Data analysis
Results are presented as medians with interquartile ranges (IQRs) and proportions. Quantitative variables were compared with the Mann–Whitney test and categorical data using the chi-square test or the Fisher test, as appropriate. Statistical analysis was performed using SPSS, version 22.0 (IBM, Somers, NY).
Results
Study population and virological response
In this study, a total of 164 women met the criteria for treatment and were initiated life-long antiretroviral therapy. Blood samples at 12 and/or 24 months were available for 107 of these women that were, therefore, included in this analysis. Patient characteristics are reported in Table 1. Patient characteristics were not different from those of the entire cohort of women meeting the criteria for treatment (data not shown). Baseline median CD4+ lymphocyte count was 218 cells/mm3 (IQR: 150–288) and baseline median plasma HIV-RNA was 22,506 copies/ml (IQR: 9,724–56,360). The majority of women (59.8%) were fully compliant with the protocol, whereas 17.8% missed more than one clinical visit between delivery and month 24. Five women during pregnancy switched to lopinavir/ritonavir for nevirapine-associated toxicity and one woman died during follow-up. At months 12 and 24 postpartum, the median values of CD4+ lymphocyte counts were 439 (IQR: 326–541) and 493 (IQR: 400–688) cells/mm3, respectively, whereas the percentage of women with HIV-RNA >50 copies/ml was 26.7% (27 out of 101 available samples) and 28.3% (28 out of 99 available samples) at months 12 and 24, respectively. If we consider the threshold of 1,000 copies, 12.9% (13/101) at month 12 and 10.1% (10/99) at month 24 had virological failure according to the WHO definition. Median viral load in women with failure was 6,787 copies/ml (IQR: 1,441–18,260) at month 12 and 4,250 copies/ml (IQR: 1,466–13,596) at month 24. No patient with low-level (50–1,000 copies/ml) viremia at month 12 had virological failure at month 24. No woman changed therapy between months 12 and 24.
ART, antiretroviral therapy; IQR, interquartile range; WHO, World Health Organization.
Resistance analysis
Numbers of available and sequenced samples are shown in Figure 1. Plasma samples were available for 106 patients at baseline. Resistance mutations were found in 6.6% of the women (7/106). All seven women had non-nucleoside reverse transcriptase inhibitors (NNRTI)-associated mutations, six harboring the E138A mutation and one the K103N mutation. At month 12, resistance mutations were seen in 40% of patients (6/15) with detectable HIV-RNA (>50 copies/ml) and available and sequenced samples. Four out of six (66.7%) had NNRTI-associated mutations (two had the K103N, one the E138A and one the Y181C mutation) and two out of six (33.3%) had both NRTI and NNRTI-associated mutations (Table 2). At month 24, resistance mutations were found in 37.5% of the women (3/8) with available and sequenced samples (one M184V mutation, one K103N+M184V mutation and one E138A mutation). Considering both time points, resistance mutations were present in 40% of the women (8/20) tested at month 12 and/or at month 24. Genotyping success rate in samples with <1,000 copies/ml was 31.0% (9/29 available samples). Within these samples in seven cases, there were no mutations, and in two cases (8%) there was only the E138A mutation (in the same woman). Genotyping success rate in samples with >1,000 copies/ml was 70.0% (14/20 available samples): in seven cases there was resistance and in seven cases no mutation was present.
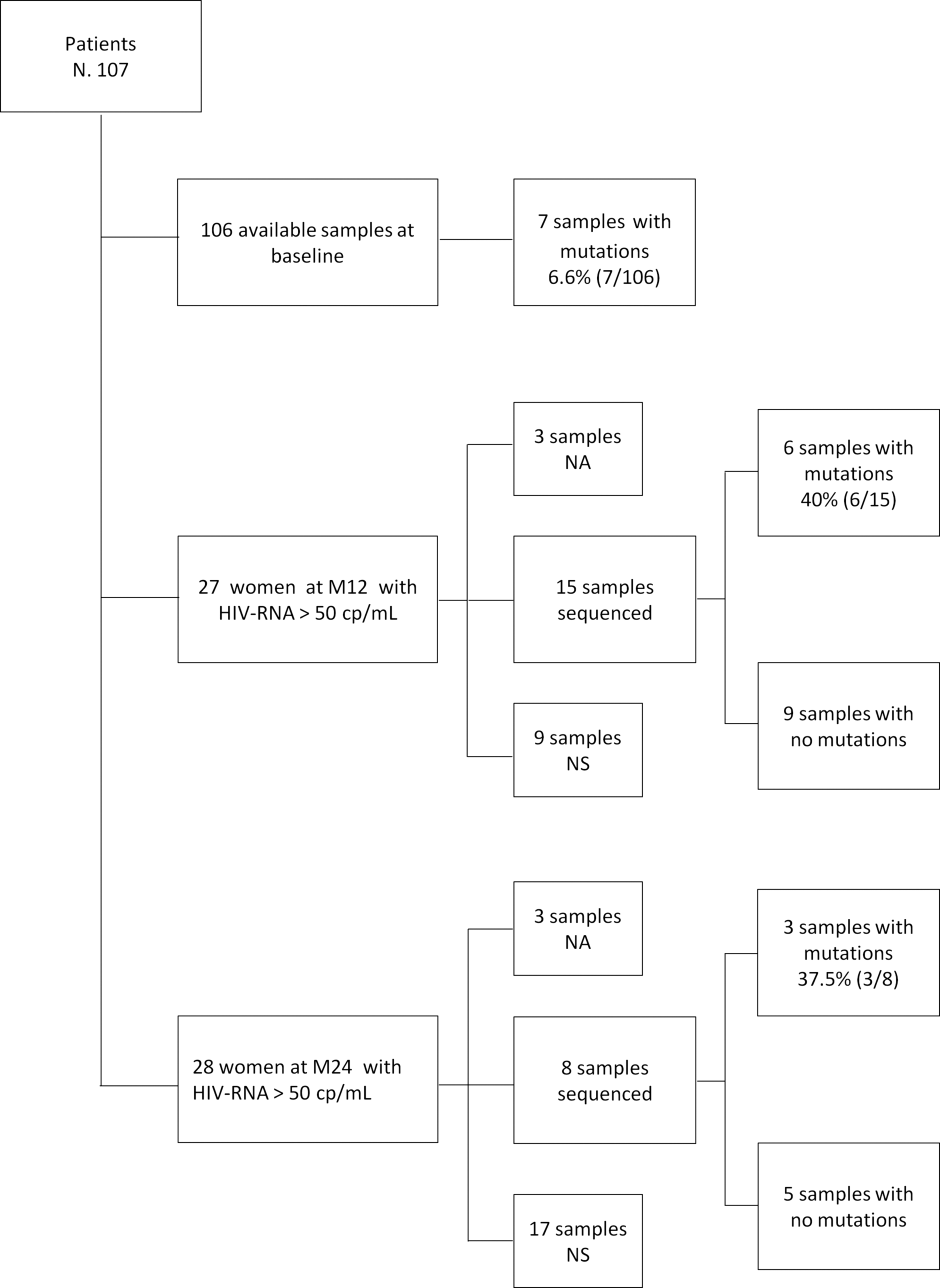
Samples available for resistance testing at months 12 and 24. NA, not available; NS, not sequenced.
NA, not available; NS, not sequenced.
There was no correlation between baseline resistance and subsequent occurrence of virological failure or the emergence of resistance mutations. In fact four out of seven (57.1%) women with baseline resistance had detectable levels of HIV-RNA either at month 12 or at month 24 compared with 36 out of 99 (36.4%) women without baseline resistance (p = .273). The same was true for virological failure: two out of seven women (28.6%) with baseline resistance had HIV-RNA >1,000 copies/ml at either month 12 or month 24 compared with 17 out of 99 (17.2%) without baseline resistance (p = .447). Baseline resistance was also not associated with emergence of mutations at later time points: no patient with baseline resistance developed mutations at either month 12 or month 24 and 7 out of 99 (7.1%) with no baseline resistance developed subsequent mutations (p = .466). No other factor was associated with the rate of virological failure or with the emergence of resistance at both time points. There was a trend toward a greater proportion of women who missed more than one clinical visit among those with no mutations at month 12 (seven out of nine women with no mutation vs. two out of six with detected resistance) (p = .085).
Discussion
In this study, we evaluated the occurrence of virological failure and the possible associated emergence of resistance mutations at 1 and 2 years postpartum in HIV-positive pregnant women initiating life-long antiretroviral treatment. We showed that virological failure (HIV-RNA >1,000 copies/ml) was infrequent, whereas the presence of low-level viremia (HIV-RNA >50 copies/ml but <1,000 copies/ml) occurred in a more significant proportion of women. Resistance mutations were present in less than half of the women studied.
Baseline resistance in this cohort was rare and not associated with subsequent outcomes. However, the numbers were small and we cannot exclude that this has prevented us to find a significant correlation (a trend was indeed present toward more frequent virological failure and baseline resistance). Also, it has to be underlined that in the majority of cases, only the E138A mutation was present at baseline. Recent data 11 indicate that E138A is polymorphic in drug-naive patients and is present in a high proportion of subtype C viruses (in Malawi subtype C is the largely predominant subtype). In a previous study 12 that we performed in a different population of the same cohort (women not meeting the criteria for treatment and, therefore, stopping antiretroviral therapy [ART] 6 months postpartum), we assessed baseline resistance in HIV-DNA to evaluate archived mutations. In that study, we found that 11.9% of the women had baseline archived resistance. This may reflect the fact that possible resistance due to previous exposure to single-dose nevirapine or transmitted resistance may have disappeared from plasma and remained archived in HIV-DNA. However, our proportion of 6% of baseline resistance in plasma is in agreement with that previously reported for Malawi. 13
The low rate of virological failure that we observed is in line with other findings obtained in HIV-infected patients on antiretroviral therapy 14,15 ; the rates of failure at month 12 (11.1%–16.1%) and at month 24 (12.4%) compare well with our rates of 12.9% and 10.1% at months 12 and 24, respectively.
Data on postpartum women are scarce. A study conducted in the United Kingdom 16 reports that the cumulative probability of viral rebound (defined as HIV-RNA >200 copies/ml) at 6 months was 35% in women starting combination antiretroviral therapy during pregnancy, significantly higher than a nonpostpartum control cohort (with a 4.8% probability of rebound). The most likely explanation was reduced adherence to ART. Data obtained in the United States 17 were similar with a proportion of viral rebound at 24 weeks of 28.6% among postpartum women.
In a study performed in Tanzania 18 on postpartum women, a very high proportion of women had HIV-RNA >1,000 copies/ml at month 12 (53%) and at month 24 (82%). The study, however, besides being based on a small number of patients (73 women), had a different CD4+ count threshold to initiate life-long ART (<200/mm3); women were, therefore, more immunocompromised and this could have affected the response to treatment. However, drug adherence in the study was identified as the main cause of the high rate of failure, confirming previous observations in resource-limited settings. 15,19 In a recent study in South African women, 20 71% at 12 months postpartum had HIV-RNA below 400 copies/ml, and factors associated with suppression included efavirenz plasma concentrations as a marker of treatment adherence. Favorable responses in our study can be related to the treatment adherence counseling all the women received. 10,21
Although the rates of virological failures were low, a significant proportion of women had low-level viremia. Previous studies 22 have associated low-level viremia with virological failure and this association was explained with the presence of drug resistance mutations. In our study, low-level viremia was not associated with subsequent virological failure, probably due to the fact that in our study mutations were not present in patients with low-level viremia, as reported in a previous study, 19 with the exception of the polymorphic E138A mutation.
We observed a low prevalence of resistance among our patients with failure (40%) compared with other studies, showing proportions between 70% and 80% of patients with resistance in failed patients. 15,19,23 We did not find any significant difference in the proportion of missed visits between patients with or without resistance (except for a trend at month 12); however, this parameter may not be sensitive enough to identify poor adherence in these women.
Overall, the global development of resistance was infrequent in the cohort with 6% of the women (6 out of 101) at month 12 and 3% (3 out of 99) of the women at month 24 with drug resistance mutations, in line with previous data. 5
Our study has several limitations: first the small sample size, second the lack of complete pairs of samples at both time points, and third the use of population sequencing for resistance not determining, therefore, the possible impact of minority variants. Furthermore, several samples were not sequenced especially at month 24, leaving a low number of patients to be evaluated. Also, these results may not directly apply to the Option B-plus scenario since these women were started on ART because of the low CD4+ cell count and, therefore, in need of treatment for their own health.
In conclusion, in these women followed for 2 years after delivery under the B approach, virological failure was rare and resistance mutations were present in less than half of the cases. These results are reassuring on the feasibility of the long-term antiretroviral administration in HIV-infected pregnant women and support the large-scale implementation of the Option B-plus approach. Further studies are needed to evaluate the role and significance of the presence of low-level viremia in this context.
Footnotes
Acknowledgments
The authors wish to thank Alessandra Mattei for administrative assistance and Patrizia Cocco e Ferdinando Costa for technical work and Marco Mirra, Massimiliano Di Gregorio, Stefano Lucattini, and Luca Fucili for IT support. This work was supported by a grant from the Istituto Superiore di Sanità, Rome, Italy (grant no. 528c/28c7) and by Esther-Italy, Ministry of Health, 2009–2010 (grant no. 9 M34).
Author Disclosure Statement
Stefano Vella has received honoraria from ViiV, Gilead, and Merck for scientific board membership. All other authors have no conflicts to declare.