
Abstract
Inversion of the CD4/CD8 ratio (<1) has been identified as a surrogate marker of immunosenescence and an independent predictor of AIDS events in HIV-infected patients and mortality in the general population. We aimed to assess the association between the CD4/CD8 ratio and carotid intima-media thickness (cIMT) progression in treated HIV-infected patients as a marker of coronary heart disease. A longitudinal study was conducted during 3 years in 96 virally suppressed HIV-infected patients receiving antiretroviral treatment (ART). We analyzed the associations between the CD4/CD8 ratio, cardiovascular risk factors, and antiretroviral treatment (ART) and progression of subclinical atherosclerosis assessed using cIMT at baseline and after 3 years. Finally, 96 patients completed the study. Seventy six (79.1%) patients were male, aged 44 ± 10 years; 39 (40.6%) were on treatment with protease inhibitors; 49 (51.04%) with nonnucleoside reverse transcriptase inhibitors, 6 (6.25%) with integrase inhibitors, 3 (3.12%) with maraviroc, and 2 (2.08%) just with nucleoside reverse transcriptase inhibitors. The mean of ART exposition was 6.9 ± 5.9 years. Twenty six (27%) patients had family history of ischemic heart disease, 51 (53.12%) were smokers, 12 (12.5%) were hypertensive, 4 (4.16%) had type 2 diabetes, 23 (23.9%) had dyslipidemia, and 31 (32.3%) were infected with hepatitis C virus. Baseline cIMT was significantly associated with age (rho = 0.497; p < .001), basal glucemia (rho = 0.323; p = .001), triglycerides (rho = 0.232; p = .023), Framingham risk score (rho = 0.324; p = .001), CD4/CD8 ratio (rho = −0.176; p = .05), and dyslipidemia (0.72 ± 0.16 mm vs. 0.63 ± 0.11 mm; p = .029). In multivariable analysis where cardiovascular risk factor and ART were included, cIMT progression was inversely associated with CD4/CD8 ratio [odds ratio (OR) = 0.283; confidence interval (95% CI) 0.099–0.809; p = .019]. In conclusion, the inversion of CD4/CD8 ratio in treated HIV-infected patients is independently associated with cIMT progression, a marker of coronary heart disease. Therefore, it might be clinically useful as predictor of cardiovascular events.
Introduction
D
In this context, our objective was to evaluate whether the CD4/CD8 ratio, which can be obtained in most clinical settings and is routinely measured in HIV-infected patients, was associated with cIMT progression in treated HIV-infected patients.
Material and Methods
Study design, participants, setting, and eligibility
An observational and longitudinal study was performed. We analyzed patients who attended university-based HIV clinic in Murcia anytime between February 2009 and June 2013. Subjects were recruited if they were HIV infected and on stable triple ART, defined as continuous treatment with three antiretroviral drugs, including either a nonnucleoside reverse transcriptase inhibitor (NNRTI) or a protease inhibitor, and if they had undetectable plasma HIV RNA levels for at least 6 months.
Exclusion criteria included the presence of cardiovascular disease (previous stroke, myocardial infarction, or intermittent claudication). The study conformed to the principles of the Declaration of Helsinki and the Good Clinical Practice Guidelines and was approved by the local Ethics Committee (“Comité Ético de Investigación Clínica del Hospital General Universitario Reina Sofía de Murcia”). All patients gave their written informed consent to participate in the study.
Clinical and laboratory measurements
Medical records were carefully reviewed and all subjects underwent a physical examination. Information on gender, age, body mass index, smoking status, family history of cardiovascular disease, and treatment with antiretroviral drugs was recorded. The presence of arterial hypertension, hypercholesterolemia, and hypertriglyceridemia was defined according to the Adult Treatment Panel III criteria. 12 A sample of fasting venous blood was obtained to determine concentrations of glucose, high-sensitivity C-reactive protein (hsCRP), interleukin-6, creatinine, total cholesterol, high-density lipoprotein (HDL) cholesterol, and triglycerides using standard enzymatic methods. Low-density lipoprotein cholesterol concentrations were calculated using the Friedewald equation. 13 Plasma viral load was measured using the COBAS TaqMan HIV-1 assay (Roche Diagnostics Systems, Branchburg, NJ). CD4 and CD8 T-cell counts were determined by flow cytometry (Beckman-Coulter, Munster, Germany). Plasma levels of hsCRP were measured using nephelometry (Siemens Healthcare Diagnostics, Deerfield, IL), vascular cell adhesion molecule (VCAM) was measured using commercially available ELISA Kits (Quantikine; R&D Systems Europe Ltd, Abingdon, United Kingdom), and interleukin-6 using chemiluminescence (Siemens Healthcare Diagnostics).
cIMT measurements
Carotid measurements were performed at the baseline visit and at year 3 of follow-up. For the determination of the cIMT, B-mode high resolution ultrasound was used following a standard procedure previously described. 14 All measurements were performed by the same investigator, who was blinded to the group to which the patients belonged. It was considered as cIMT progression if there was an increase of 5% compared to baseline.
Statistical analysis
To compare the study groups (cIMT progression vs. no progression), we used the Mann–Whitney U-test and the χ 2 test where appropriate. The Wilcoxon signed-rank test was used to compare differences in basal and after 3 year measures. Binary logistic regression was used to evaluate the independent variables associated with cIMT progression. Significance levels were placed at p < .05.
Results
Table 1 summarizes the main characteristics of the 96 subjects included in the study.
Categorical variables are expressed as frequencies (%). Continuous variables are expressed as mean (standard deviation). Dyslipidemia, diabetes, and hypertension were defined by a previous diagnosis or by a current prescription of pharmacological therapy for any of such risk factors.
ART, antiretroviral therapy; CHD, cardiovascular heat disease; cIMT, carotid intima-media thickness; HCV, hepatitis C virus; IDU, intravenous drug user; IMT, intima-media thickness; NNRTI, nonnucleoside reverse transcriptase inhibitor; PI, protease inhibitors; VCAM, vascular cell adhesion molecule; hs-CRP, high-sensitivity C-reactive protein.
Thirty-nine (40.6%) were on treatment with protease inhibitors, 49 (51.04%) with NNRTIs, 6 (6.25%) with integrase inhibitors, 3 (3.12%) with maraviroc, and 2 (2.08%) just with nucleoside reverse transcriptase inhibitors. The mean of ART exposition was 6.9 ± 5.9 years, the median CD4 count was 584 cells/ml, and 100% of patients had undetectable viral load.
Most patients (70%) displayed a low 10-year cardiovascular risk (<10%), estimated using the Framingham risk score. Moreover, more than 50% had hs-CRP higher than 3 mg/dl despite being long-term virally suppressed.
Baseline cIMT was significantly associated with age (rho = 0.497; p < .001), basal glucemia (rho = 0.323; p = .001), triglycerides (rho = 0.232; p = .023), Framingham risk score (rho = 0.324; p = .001), basal CD4/CD8 ratio (rho = −0.176; p = .05), and dyslipidemia (0.72 ± 0.16 mm vs. 0.63 ± 0.11 mm; p = .029). In multivariate linear analysis, the age (beta coefficient 0.588; p < .001) and basal CD4/CD8 ratio (beta coefficient −0.127; p = .013) were independently associated with cIMT (R 2 = 0.359; p < .001).
There was a positive correlation between basal levels of hs-CRP and progression of cIMT (Pearson correlation 0.354; p = .009) (Fig. 1).

Correlation between basal inflammation (hsCRP) and cIMT progression. Pearson correlation was 0.354 (p = .009). cIMT, carotid intima-media thickness; hsCRP, high-sensitivity C-reactive protein.
Table 2 summarizes the characteristics of patients according to progression of cIMT. A total of 54 patients (56.25%) showed progression of cIMT. No significant differences were found between both groups in the frequency of cardiovascular risk factors, ART, levels of CD4, and inflammatory markers (hsCRP and VCAM). Individuals with cIMT progression showed lower CD4/CD8 ratio at baseline and after 3 years of follow-up.
Categorical variables are expressed as frequencies (%). Continuous variables are expressed as mean (standard deviation). Dyslipidemia, diabetes, and hypertension were defined by a previous diagnosis or by a current prescription of pharmacological therapy for any of such risk factors.
In Figure 2 are shown CD4/CD8 ratios according to progression of cIMT.
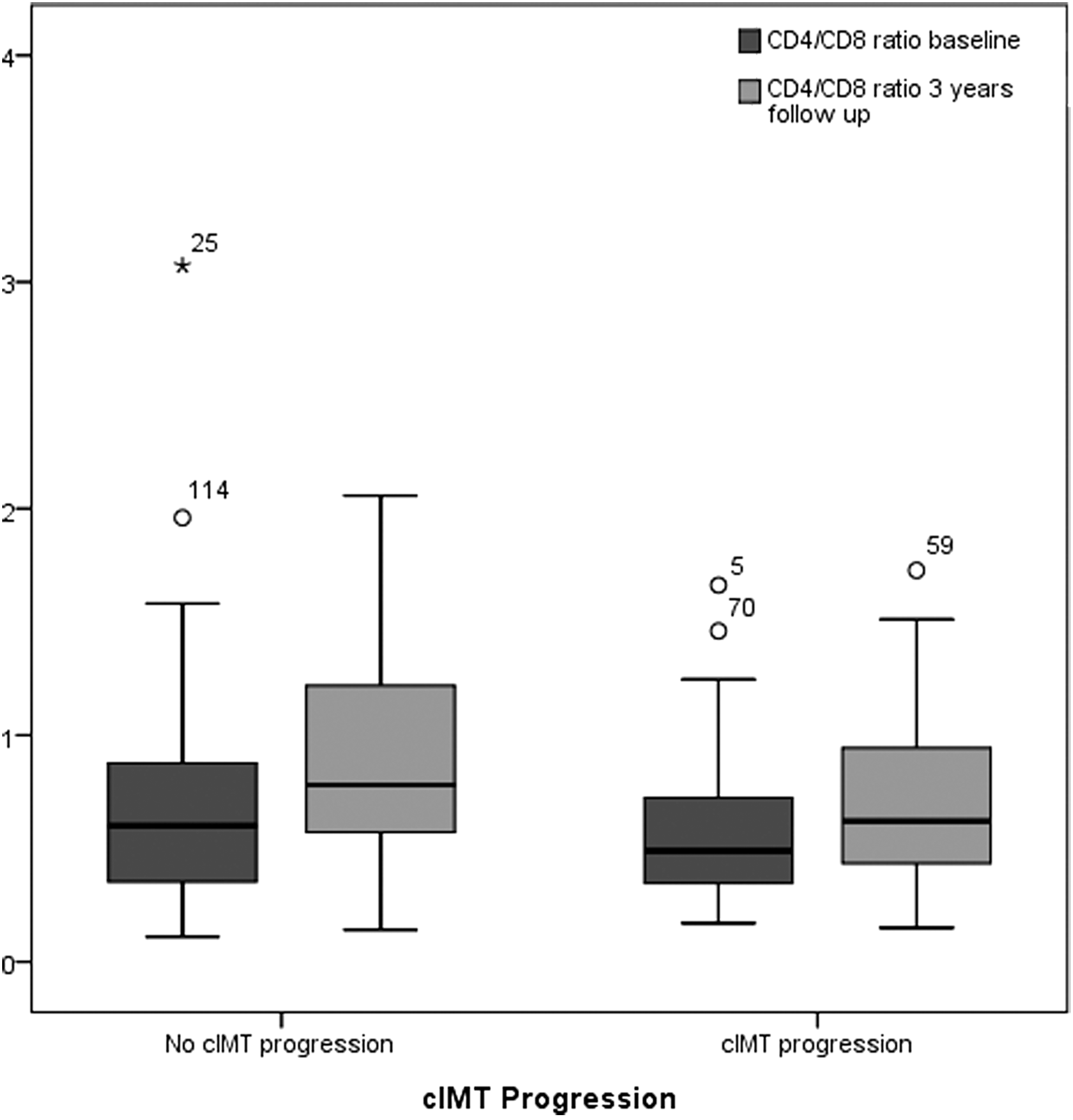
Box plot of CD4/CD8 ratio at baseline and after 3 years follow-up according to cIMT progression. HIV-infected patients with cIMT progression had lower CD4/CD8 ratio at baseline (p = .05) and after 3 years follow-up (p = .04).
Logistic regression models were explored to analyze the association between cIMT progression and CD4/CD8 ratio adjusted by age, sex, dyslipidemia, tobacco use, and cumulative ART exposure. In a multivariate analysis, the only one factor independently associated with cIMT progression was the inversion of CD4/CD8 ratio [odds ratio (OR) = 0.283, confidence interval (95% CI) 0.099–0.809; p = .019] at baseline.
Discussion
In this study conducted in HIV-infected subjects on ART virally suppressed with low cardiovascular risk, we found that the CD4/CD8 ratio was negatively correlated with progression of cIMT after 3 years of follow-up.
The cIMT progression in HIV-infected patients has basically not only been associated with traditional cardiovascular risk factors, such as hypertension, age, smoking, dyslipidemia, and diabetes, but also with ART as protease inhibitors and CD4 nadir. 3,15 The progression of cIMT in our patients was slight and lower than others. 15 –19 Unlike other studies performed in HIV-infected patients where more than 70% were smokers, in our study only 50% were nonsmokers. Furthermore, most of the subjects in our study had a low cardiovascular risk (less than 30% had Framingham risk score more than 10%) and less than 40% were on treatment with protease inhibitor, an antiretroviral treatment related to higher cIMT and coronary heart disease. 20 Moreover, this study was conducted in a Mediterranean cohort, a population where coronary heart disease is less prevalent than in others.
In a similar way to other studies where traditional factors are most importantly associated with atherosclerosis in HIV-infected patients, in our study, classical risk factors such as age, dyslipidemia, Framingham risk score, and glucemia were associated with basal cIMT. However, the only one factor that independently was associated with the progression of cIMT was inversion of CD4/CD8 ratio.
In recent years, consistent data have led to the general assumption that HIV infection leads to an increased risk of “non-AIDS-related” events. Although the underlying mechanisms are not fully understood, a whole body of research suggests that these adverse outcomes are linked to a remodeling of the immune system. Persistent inflammation and immune activation are widely accepted as the major driving factors of this immunosenescence and exhaustion that ultimately lead to disease progression and adverse outcomes. 21 The extent to which ART reverses these HIV-induced immune changes is currently the subject of ongoing investigation. Interestingly, in our study, there was a positive strong correlation between cIMT progression and baseline levels of hsCRP, although in the multivariate analysis it was not shown as an independent risk factor, probably due to sample size and because over 50% of our patients had elevated levels of hsCRP, indicating a high pro-inflammatory state despite receiving ART and being virology suppressed. The chronic inflammation is an important factor associated with atherosclerosis and cardiovascular events that HIV-infected patients on ART have. 10 At present, the causes of this higher inflammation are not known and it is under investigation. It is thought that low level of viral replication, bacterial translocation, cytomegalovirus (CMV) replication, and loss of regulated T cells could have influence in developing and maintaining chronic inflammation. In addition, hsCRP is an important marker related to atherosclerosis, cardiovascular events, and mortality. 22 In contrast, most of individuals (85%) in our study exhibited an inverted CD4/CD8 ratio despite at least 6 months of ART-mediated plasma virus suppression and CD4 T-cell count recovery. Outside HIV infection, a low CD4/CD8 ratio, also termed the immune risk profile, is considered a surrogate marker of immunosenescence and has been shown to be an independent predictor of all-cause mortality. 6,23 Furthermore, CD4/CD8 ratio has been associated with immune activation. 8,24 In a cross-sectional analysis with long viral suppression, CD4/CD8 ratio was an independent predictor of CD4 T-cell activation 24 and inversion of the CD4/CD8 was a strong independent predictor of higher percentages of CD8 T cells expressing activated (HLA-DR+CD38+), senescent (CD58+CD27−), and activated/exhausted (HLA-DR+PD-1+) phenotypes. 8 In view of the fact that immune activation is considered the major driving factor of this premature aging in HIV infection, these data suggested that inversion of the CD4/CD8 ratio could help to identify ART-treated patients at higher risk of noninfectious events.
Inversion of CD4/CD8 ratio has been correlated previously with marker of age-associated disease as cIMT, sarcopenia, and estimated glomerular filtration rate, 10 but there are no studies that evaluate its relationship with atherosclerosis progression or cardiovascular events.
The present study provides an insight into the clinical significance of the CD4/CD8 ratio in treated HIV-infected subjects, as we have demonstrated its value as a variable independently associated with cIMT progression as a marker of atherosclerosis and important predictor of cardiovascular events in the general population. 25
This study has several limitations. A statistical association between a risk factor and a measure of atherosclerosis does not prove that the risk factor directly promotes atherogenesis. cIMT reflects the cumulative effects of risk factors acting over many years, whereas we measured risk factors at one point in time only. Thus, blood cholesterol and triglyceride levels or blood pressure measured at baseline may not accurately represent lifetime exposure. The study may be underpowered to detect weak relationships; several risk factors thought to be important, such as HDL cholesterol, triglyceride, VCAM and hsCRP levels, or use of protease inhibitors, were not independent predictors of cIMT progression. Finally, the findings in our HIV patients from a Mediterranean clinic may not necessarily apply to other HIV-infected populations.
In conclusion, in this study in treated HIV-infected subjects, a low CD4/CD8 ratio, despite at least 6 months of effective ART, was an independent marker of conditions associated with age-related disease as progression of carotid atherosclerosis. These findings may have implications in both research and clinical settings.
Footnotes
Author Disclosure Statement
No competing financial interests exist.