
Abstract
To assess the efficacy and safety of maraviroc (MVC) administered once-daily in routine clinical practice. A retrospective multicenter study (27 centers in Spain) was conducted. Data were collected from the records of patients starting a regimen with MVC. Laboratory and clinical data were recorded every 3 months the first year and every 6 months thereafter. Data are presented as median and interquartile range. Among 667 patients treated with MVC, 142 (21.3%) received MVC once-daily: 108 (76.1%), 150 mg and 34 (23.9%), and 300 mg. Age was 47 (42–45) years, there were 76.1% men, and 81 (57%) patients had baseline HIV-RNA <50 copies/mL. Viral tropism was R5 in 118 (83.1%) patients. Reasons for prescribing MVC: salvage therapy (36.6%), drug toxicity (31.2%), simplification (16.9%), and immunodiscordant response (7.1%). Median follow-up was 13 (9–16) months. In 95.8%, a PI/r was part of the regimen (67% on dual therapy). At months 12 and 24, 73.3% and 68.2% of patients had HIV-RNA <50 copies/mL, respectively (p = .041 and p < .001 vs. baseline). CD4+ cell count increased by a median of 52 (−36,135) and 84 (−9.5,180) cells/mm3 at 12 and 24 months, respectively (p < .001 and p = .039 vs. baseline). Twenty-five (17.6%) patients discontinued MVC: virologic failure (6), medical decision (5), and other reasons (14). Two patients presented grade 3 adverse events (hypertransaminasemia, hypertriglyceridemia) without the need for MVC withdrawal, whereas MVC was discontinued in two patients due to gastrointestinal toxicity. In routine clinical practice, MVC once-daily combined with at least PI/r was virologically effective and well tolerated in a high percentage of pretreated patients.
M
The aim of this study was to assess the efficacy and safety of MVC administered once-daily in routine clinical practice.
This is a substudy of an observational multicenter study, carried out in 27 Spanish hospitals. 8 Data were retrospectively collected from the clinical records of patients starting a regimen with MVC. Follow-up data included laboratory parameters (CD4+ cell count and plasma HIV-RNA), clinical adverse events, occurrence of an AIDS-defining event or death, and the reasons for MVC discontinuation. The study was approved by the institutional review boards and ethics committees of all participating centers, and patients gave informed consent.
The primary endpoints were the percentage of patients with plasma HIV-RNA <50 copies/mL and CD4+ cell count changes at months 12 and 24. Secondary endpoints were the safety of the regimens and causes of MVC discontinuation. Virological failure was defined as confirmed HIV-RNA >50 copies/mL.
An FDA snapshot analysis was performed, with patients changing treatment or lost to follow-up considered as failures, including all individuals receiving at least 1 dose of MVC. Comparisons between baseline and follow-up in each arm were carried out with the paired t-test or Wilcoxon signed-rank or McNemar test. Comparisons between patients taking MVC 150 or 300 mg/day were done with the Mann-Whitney U, chi-square, or Fisher exact test. Continuous variables are expressed as the median and interquartile range (IQR).
Data from 667 patients were collected from October 2012 to May 2013, and 142 patients (21.3%) had received MVC once-daily. Baseline characteristics are summarized in Table 1. Viral tropism was known to be R5 in 118 patients (83.1%), and the percentage could be higher, taking into account that there were 21 patients (14.8%) with unknown viral tropism. Compared with patients receiving 150 mg/day, those on 300 mg/day had higher baseline HIV-RNA levels (2.14 vs. 1.3 log copies/mL; p = .002) and more frequently, salvage therapy was the reason for prescribing MVC (58.8% vs. 29.6%; p = .006). In 136 (95.8%) patients, MVC was combined with a PI/r, which was given as dual therapy in 96 patients: 68 (71%) received darunavir/r, and 24 (25%) received atazanavir/r. The median follow-up was 13 months (9–16).
Continuous variables are expressed as median and interquartile range.
PI+NNRTI or raltegravir+NRTI: 9; PI+raltegravir+NNRTI±NRTI±T-20: 3; NNRTI+raltegravir+NRTI±T-20: 3; IP+T-20+AN: 1.
PI +1 NRTI: 3; PI+raltegravir: 2; PI+NNRTI: 2; NNRTI+raltegravir: 1; raltegravir+NRTI: 1; 2 PI +1 NRTI: 1, 3 NRTI: 2.
HCV, hepatitis C virus; MVC, maraviroc; NNRTI, non-nucleoside reverse transcriptase inhibitor; NRTI, nucleoside reverse transcriptase inhibitor; PI, protease inhibitor.
A significant increase in the percentage of patients with HIV-RNA <50 copies/mL was observed at months 12 and 24 [77/105 (73.3%); p = .041 and 15/22 (68.2%); p < .001 vs. baseline, respectively]. CD4+ cell count increased at months 12 and 24 [448 (270–703); p < .001 and 466 (266–604); p = .039 vs. baseline, respectively], as well as the percentage of patients with CD4+ cell count >200 cells/mm3 at month 12 (87.4%; p = .002). There were no differences in the percentage of virologic failure at months 12 or 24 when comparing salvage therapy with toxicity or simplification as the reason for prescribing MVC, or between patients receiving 150 or 300 mg/day.
In patients receiving dual therapy (MVC and PI/r), toxicity (44%) was the most frequent reason for prescribing MVC, followed by simplification (22.9%), and salvage therapy (21%). In this subgroup, HIV-RNA <50 copies/mL was achieved in 74.3% of patients at month 12 and was achieved in six patients at month 24 (week 96 remove).
Maraviroc was discontinued in 25 (17.6%) patients with a gradual discontinuation over time as is shown in figure 1, with a median (IQR) of 8 (4-11) months. MVC was interrupted due to: virologic failure (6 patients, 5 receiving 150 mg), medical decision (5), gastrointestinal toxicity (2), loss to follow-up (2), withdrawal from treatment (2), death (2), study completion (2), and simplification (2).
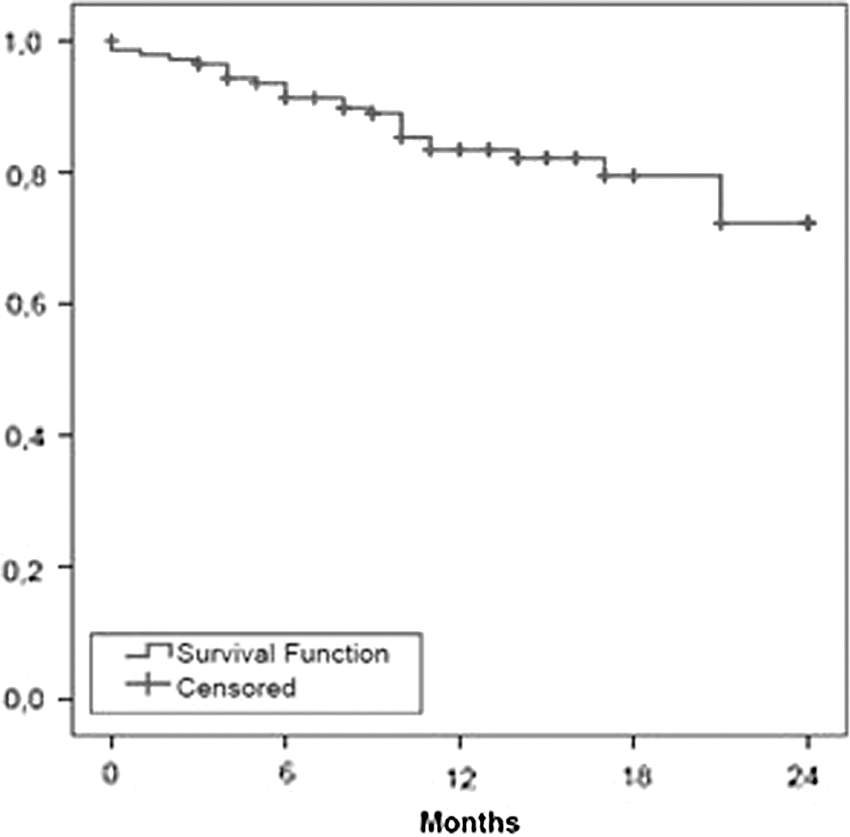
Survival curve of maraviroc discontinuation.
Forty-two patients (29.6%) experienced at least one adverse event, which were grade 1 or 2 in the majority of cases. Only five grade 3 or 4 adverse events occurred, two of them deemed related to MVC use (one grade 3 hypertransaminasemia and one hypertriglyceridemia), without withdrawal of the drug. In two patients, MVC was discontinued due to gastrointestinal toxicity. Five category C AIDS-defining events occurred (two tuberculosis, one esophageal candidiasis, one non-Hodgkin lymphoma, and one Kaposi's sarcoma).
The present study analyzes the largest cohort of patients taking MVC once-daily in routine clinical practice. We showed that in treatment-experienced HIV-infected patients, MVC once-daily combined with at least a PI/r was virologically effective and well tolerated in a high percentage of patients.
Pharmacokinetic data support once-daily MVC use combined with a PI/r, but there is little available clinical information of efficacy and safety from randomized or observational studies. 2,3,6,7
Unexpectedly, a high percentage of the patients compiled had received dual therapy with MVC and a PI/r, a non-standard regimen, that could be interesting in some scenarios due to toxicity, comorbidities, or prior failure or resistance to nucleos(t)ide reverse transcriptase inhibitors or non-nucleoside reverse transcriptase inhibitors. To our knowledge, there is only one observational study reporting the use of this regimen, including 60 pretreated patients starting MVC 150 mg once-daily combined with darunavir/r 800/100 mg, with a virologic success achieved in 75% of patients at month 12, similar to that observed in patients on dual therapy in our study (74.3%), which supports the efficacy of this dual combination. 7
To our knowledge, no comparisons between MVC once- and twice-daily have been reported since the initial Motivate studies. 2 Patients receiving MVC twice-daily in the overall cohort showed virological success rates of 77% and 79.8% at months 12 and 24, comparable to the rates found in the present substudy. 8 However, patients receiving MVC twice-daily had lower CD4+ cell counts and higher HIV-RNA levels at baseline, and a higher percentage of them were prescribed MVC for salvage therapy, than patients receiving the once-daily regimen. Therefore, this comparison should be viewed with caution, as there were significant differences between patients receiving each dose; hence, there is a risk of prescription bias, favoring the choice of once-daily dosing in easier-to-treat individuals. 8
The optimal MVC dose (150 mg/day vs. 300 mg/day) is uncertain. Several trials have assessed the pharmacokinetic parameters of MVC once-daily at a dose of 150 or 300 mg combined with a PI/r in naive and pretreated patients. 5,9 In those studies, most participants achieved adequate pharmacokinetic parameters based on reference values related with virologic success. 10 In our study, patients receiving 300 mg daily had a higher HIV viral load at baseline, and salvage therapy was the main reason for initiating MVC. Virological efficacy was similar between the two doses; therefore, in patients with poorer clinical status, the 300 mg once-daily dose would likely be preferable.
There were few MVC-related adverse effects or discontinuations due to toxicity in our sample, in concordance with the findings from previous studies, 1,2,7,8 supporting a favorable safety profile for this drug.
This study has the limitations inherent to a retrospective design and the absence of a protocol for MVC prescription. Furthermore, pharmacokinetic data were not available; hence, we cannot know whether plasma levels of the drug were below the desirable threshold, mainly when 150 mg once-daily dosing was used.
In conclusion, in routine clinical practice, prescription of MVC once-daily may be an effective, safe treatment, at least when combined with a PI/r, even in a salvage therapy scenario. However, those patients with suppressed HIV-RNA who should change combined antiretroviral therapy due to simplification and/or toxicity may be the best candidates to this strategy.
Footnotes
Acknowledgments
The authors thank the study participants, study investigators, and study site staff.
ViiV Healthcare supported the study with an unrestricted grant.
Members of the MVC Cohort Spanish Group: Jhon Fredy Rojas, Iñaki Pérez, Josep M Gatell (Hospital Clinic IDIBAPS, Barcelona); Isabel Bravo, Jordi Puig, Cristina Herrero, Silvia Gel, Josep M Llibre (Hospital Universitari Germans Trias i Pujol, Badalona, Barcelona); Loreto Martínez-Dueñas López-Marín, Antonio Rivero (Hospital Universitario Reina Sofía, Córdoba); María Jesús Perez-Elías, Alberto Díaz, David Arroyo, Javier Zamora, Santiago Moreno (Hospital Universitario Ramón y Cajal, Madrid); Miguel García del Toro, Puri Rubio (Consorcio Hospital General Universitario, Valencia); Juan Ant° Pineda; Eva Recio (Hospital Universitario Ntra Sra de Valme, Sevilla); Juan Pasquau, Coral García-Valdecillos (Hospital Universitario Virgen de las Nieves); Mar Masià, Catalina Robledano, Félix Gutiérrez (Hospital General Universitario, Elche, Alicante); Manel Crespo, Jordi Navarro, Ariadna Torrella (Hospital Universitari Vall d'Hebrón, Barcelona); José Hernández-Quero, Valme Sánchez-Cabrera (Hospital Universitario San Cecilio, Granada); Jesús Sanz (Hospital Universitario La Princesa, Madrid); Manuel Márquez (Hospital Clínico Universitario Virgen de laVictoria, Málaga); Antonio Ocampo, Fernando Warncke (Complejo Hospitalario Universitario de Vigo, Vigo); Josean Iribarren, Miriam Aguado-Atorrasagasti (Hospital Universitario Donostia, San Sebastián); Maria José Galindo, Ramón Ferrando (Hospital Clínico Universitario, Valencia); Carlos Minguez (Hospital General de Castellón); Daniel Podzamczer, Maria Saumoy (Hospital de Bellvitge, L'Hospitalet de Llobregat, Barcelona); Alberto Terrón, Patricia Bancalero Herrera (Hospital del SAS de Jerez de la Frontera, Cádiz); José Ramón Arribas, María Yllescas (Hospital Universitario La Paz, Madrid); Hernando Knobel, Judith Villar (Hospital del Mar, Barcelona); Manuel Fernández-Guerrero (Fundación Jiménez Díaz, Madrid); Pere Domingo, Jessica Muñoz (Hospital Sant Pau, Barcelona); Teodoro Martín (Hospital Universitario Puerta de Hierro, Majadahonda, Madrid); Juan Miguel Santamaría, Oscar Luis Ferrero (Hospital de Basurto, Bilbao); Ma Rosario Pérez-Simón (Complejo Asistencial Universitario, León); Rafael Torres (Hospital Universitario Severo Ochoa, Leganés, Madrid); and Rafael Rubio, Angel Portillo (Hospital Universitario 12 de Octubre, Madrid).
Author Disclosure Statement
M.S., J.M.L., A.T., H.K., J.R.A., P.D., A.R., S.M., and D.P. have served as advisors or speakers or have been awarded grants for clinical research from Gilead Sciences, Merck Sharp and Dohme, ViiV Healthcare, Bristol-Myers Squibb, or Janssen-Cilag. D.A.-M. declares no conflict of interest.