
Abstract
African and Caribbean Black (ACB) women in Canada are disproportionately impacted by new HIV infections. ACB women's HIV vulnerability is shaped by contexts of stigma and discrimination. HIV-related stigma compromises quality of life (QOL) among women living with HIV (WLWH), yet scant research has examined concomitant effects of racial discrimination and HIV-related stigma on QOL. We used data from a cross-sectional survey with ACB WLWH in Ontario (n = 173) to test a conceptual model of pathways between HIV-related stigma, racial discrimination, depression, social support, and QOL. We conducted structural equation modeling using maximum likelihood estimation to test the model. In independent models, HIV-related stigma was associated with lower QOL, and depression partially mediated the association between HIV-related stigma and QOL. In the simultaneous model, HIV-related stigma had significant direct effects on depression, social support, and an indirect effect on QOL. When social support was added as a mediator, the direct effect between HIV-related stigma and QOL was no longer significant, suggesting mediation. Racial discrimination had significant direct effects on HIV-related stigma, depression, and social support and an indirect effect on QOL. QOL was associated with higher social support and lower depression scores. The model fit the data well: χ 2 = 203.266, degrees of freedom (DF): 112, p < .0001; Comparative Fit Index (CFI): 0.929, Tucker-Lewis Index (TLI): 0.912, Root-Mean Square Error of Approximation (RMSEA): 0.071. We found racial discrimination was associated with increased HIV-related stigma, and HIV-related stigma and racial discrimination compromised QOL. Findings suggest the need for multilevel interventions to reduce stigma and discrimination, address depression, and build social support to improve QOL among ACB WLWH.
Introduction
A
Social and structural drivers contribute to HIV vulnerability among ACB women. Stigma and discrimination based on HIV, gender, race, and ethnicity converge increase vulnerability to HIV infection, while reducing access to care. 7,9 –12 Stigma and discrimination also contribute to mental health issues and reduced quality of life (QOL) among people living with HIV (PLHIV). 13 –16 HIV-related stigma includes processes of devaluing, labeling, and stereotyping that result in loss of status, unjust and unfair treatment, and social isolation of PLHIV. 17 Racial discrimination and racism refer to the ways in which negative beliefs, attitudes, and stereotypes targeting ethnoracial minorities result in systemic inequalities and reduced access to power, services, opportunities, and material goods. 18,19 HIV-related stigma and racism both harm health and well-being across diverse contexts and populations, 20,21 yet scant research has assessed the concomitant effects of racial discrimination and HIV-related stigma on QOL among PLHIV. 17 –20,22
QOL is an essential marker of overall well-being, providing information about an individuals’ range of health outcomes, including physical, mental, and social health. 23,24 QOL is important to examine among PLHIV, as the impacts of HIV on the lives of PLHIV extend beyond physical health to mental health and other aspects of well-being. 25,26 Research has identified disparities in QOL between PLHIV and non-PLHIV; PLHIV report significantly higher levels of anxiety, depression, pain discomfort, reduced mobility, self-care, and lower ability to perform everyday activities. 27 Some studies have found that women consistently report lower QOL in comparison with men. 28 –30 Lower QOL among PLHIV persists after controlling for HIV infection stage. 29 Degroote's review of factors that influence health-related QOL (HRQoL) among PLHIV identified depression as a strong predictor of poor HRQoL; depression may negatively influence both mental and physical health among PLHIV. 31 HIV-related stigma is associated with reduced HRQoL among PLHIV. 21,31,32 Scant research has explored racism or ethnoracial identity and QOL among PLHIV. 20,31 Racism, however, has been associated with increased HIV-related stigma. 9,33 Social support is a key factor in improving HRQoL among PLHIV in North America. 31 A recent systematic review reported positive impacts of social support group participation on QOL among PLHIV. 34
To sum up, literature focusing on stigma and QOL among PLHIV has predominantly focused on HRQoL and HIV-related stigma. Gaps in knowledge remain regarding factors associated with multiple dimensions of QOL, and associations between QOL and other intersecting forms of stigma, such as racism, among PLHIV. 25,27,31,35 This study aimed to extend our understanding of correlates of QOL among ACB women living with HIV (WLWH) in Ontario, Canada. The study objectives were as follows: (1) to examine associations between racial discrimination, HIV-related stigma, and QOL; and (2) explore social support and depression as mediators of the association between stigma/discrimination and QOL among ACB WLWH.
Materials and Methods
We conducted a community-based research project with ACB WLWH that involved a community advisory board (n = 11) and collaborations with AIDS Service Organizations (ASOs), community health centers, ethno-specific agencies, and hospitals. We hypothesized the following: (1) higher levels of HIV-related stigma and racial discrimination would be associated with lower QOL; (2) higher levels of social support and lower levels of depression would be associated with higher QOL; and (3) HIV-related stigma and racial discrimination would be associated with increased depression and reduced social support, which would contribute to lower QOL (mediation).
Data collection
A cross-sectional survey was administered to ACB WLWH (n = 173) in five cities in Ontario, Canada, from June 2010 to January 2011. Locations were determined by the presence of ASOs that deliver support services to ACB women. Peer research assistants (PRAs) (n = 9) were ACB women who were living with HIV and/or working at ASOs in the same region as participants; PRAs were hired to conduct surveys to mitigate power differentials between researchers and research participants. PRAs participated in a 2-day research training that addressed research methods, ethics, survey implementation, and career development information and were provided ongoing support by the research investigators through biweekly teleconferences. Women's College Hospital at University of Toronto provided Research Ethics Board approval.
Convenience and venue-based sampling strategies were implemented. Recruitment through flyer, email listservs, and word-of-mouth was conducted at ASOs, community health centers, hospitals, and other community-based organizations in regions in Ontario that offered services to ACB WLWH. PRAs also reached out to social networks to recruit participants. PRAs aimed to target 200 participants across regions. There is no consensus on sample sizes for structural equation modeling (SEM). 36 As our SEM analyses included 5 variables, 3 of which were latent variables combining 15 indicators, this target sample size included 10 cases/variables. Prospective participants were adults aged 18 years and older, who were able to provide informed consent and self-identified as: (1) a woman, (2) HIV positive, and (3) Black, African, and/or Caribbean race/ethnicity.
Measures
Surveys were verbally administered, 90-min long, and participants chose to complete the questionnaire in a private room, community agency, or their own home. No identifying information was collected and each participant provided informed consent. Following survey completion, PRAs provided compensation ($50 CAD) to all participants as well as information on the availability of support and health services in their respective regions. We collected information about sociodemographic variables, including age, income, education, and ethnicity.
QOL was assessed using the WHO-QOL-BREF measure, consisting of six dimensions of QOL: physical health, psychological health, independence, social relationships, environment, and spirituality. 37 Cronbach's α for the overall scale was 0.93; subscales: physical health α = 0.73, psychological health α = 0.70, independence α = 0.72, social relationships α = 0.76, environment α = 0.82, and spirituality α = 0.74.
The HIV “Stigma Scale Revised” was used to measure HIV-related stigma. 38 This was adapted from Berger's stigma scale, consisting of a 10-item scale that comprised 4 subscales: personalized stigma, disclosure, negative self-image, and public attitudes. 38 Cronbach's α for the overall scale was 0.86; subscales: personalized stigma α = 0.89, disclosure α = 0.76, negative self-image α = 0.87, and public attitudes α = 0.76. The “Everyday Discrimination Scale” was used to assess racial discrimination using a modified scale from Clark et al. 39 Original instructions were “In your day-to-day life how often have any of the following things happened to you?” which were replaced with “In your day-to-day life how often have any of the following things happened to you because of your race?.” 39 The scale included nine items: treated with less courtesy, treated with less respect, receive poorer service, people act as if you are not as smart, people act as if they are afraid of you, people act as if you are dishonest, people act as if they are better, and called names, threatened, or harassed you (Cronbach's α = 0.91).
Social Support was measured with the MOS Social Support survey. 40 This 19-item survey consisted of five subscales: emotional, informational, tangible, affectionate, and positive social interaction. Cronbach's α for the overall scale was 0.95; subscales: emotional support α = 0.92, informational support α = 0.79, tangible support α = 0.86, affectionate support α = 0.61, and positive social interaction α = 0.93. The Beck Depression Inventory-Fast Screen (BDI-FS) was used to conduct a brief assessment of cognitive and affective depression symptoms (Cronbach's α = 0.85). 41
Data analysis
We assessed frequencies and means and standard deviations (SDs) among variables using descriptive analyses and conducted bivariate correlation analyses between variables. To calculate total scores for racial discrimination, HIV-related stigma, depression, social support, and QOL, scale items were added together and reverse coded where required. Subscales and total scores were calculated for HIV-related stigma (personalized, disclosure, negative self-image, public attitudes), QOL (physical health, psychological health, independence, social relationships, environment, spirituality), and social support (emotional, tangible, affectionate, positive social interaction). Data analyses were conducted using IBM SPSS version 23 and AMOS version 20.
We conducted SEM with maximum likelihood estimation to test the direct effects of HIV-related stigma and racial discrimination on QOL, as well as indirect effects through social support and depression (Fig. 1). SEM may include observed variables as well as latent variables that measure underlying constructs; SEM allows for modeling multivariate relationships and estimating indirect effects and mediation. 42 This method was appropriate for these research analyses that included three latent constructs (HIV-related stigma, social support, and QOL). We assessed model fit with the following: chi-square; Root-Mean Square Error of Approximation (RMSEA), where a score <0.08 indicates an acceptable fit; Comparative Fit Index (CFI), where a score greater than 0.90 is an acceptable fit; and the Tucker-Lewis Index (TLI) with a desired value of >0.90. 43
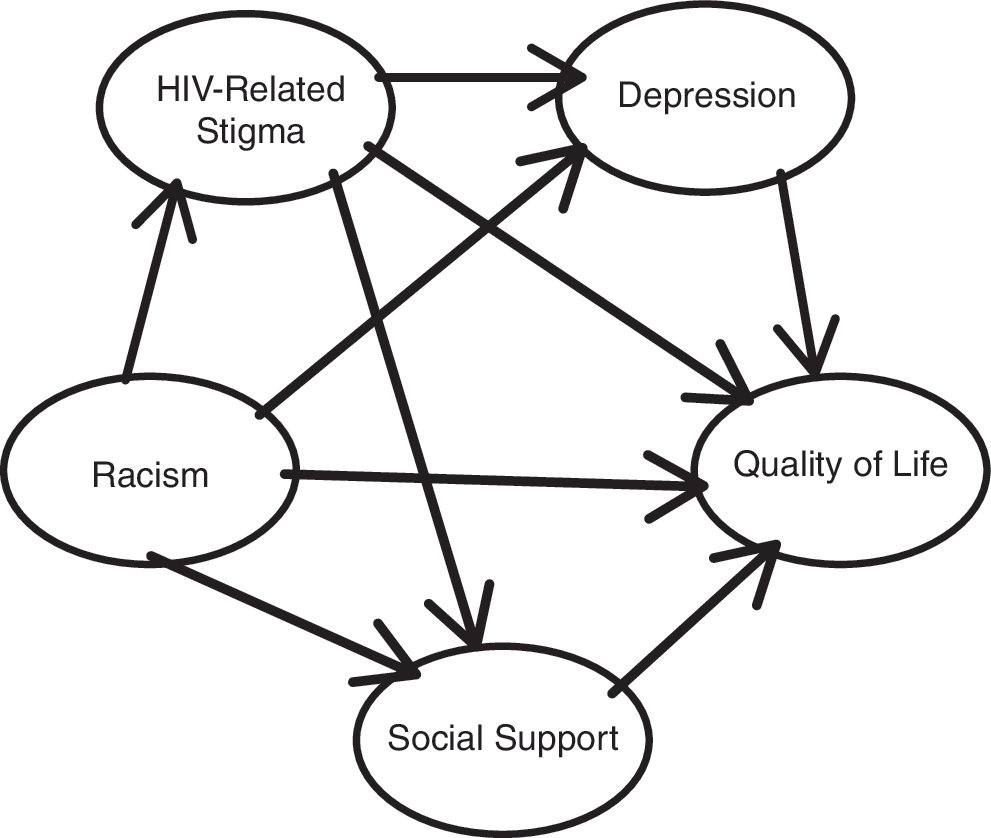
Tested conceptual model of factors contributing to quality of life among African and Caribbean women living with HIV.
Results
Participants
Table 1 portrays sociodemographic characteristics of survey participants (n = 173). The mean age of participants was 40.7 years (SD 8.8). Participants reported an average monthly income of $1,400.00. Most participants (89%; n = 154) were born outside of Canada, 69.5% (n = 107) in 25 different African countries, 29.9% (n = 46) in 7 Caribbean countries, and 0.6% (n = 1) in the United Kingdom. We included 166 participants in data analyses with complete measurement data for key outcomes (HIV-related stigma, racial discrimination, depression, social support, and QOL). There were no significant differences between participants included and excluded from data analyses.
Bivariate analyses
Table 2 summarizes bivariate correlations between study variables. HIV-related stigma positively correlated with racial discrimination and depression, and negatively correlated with social support and QOL. Racial discrimination positively correlated with depression, and negatively correlated with social support and QOL. Depression negatively correlated with social support and QOL, and social support positively correlated with QOL. All correlations were significant at the p < .01 level.
Correlation is significant at p < .01 (two-tailed).
SEM results
Initial modeling results indicated a minimally adequate fit (CFI slightly <0.90) between the model and data. After examining modification indices to assess standardized residuals, we identified a theoretically sound change that added a pathway between depression and the HIV-related stigma subscale “negative self-image.” Adding this pathway improved the model fit.
We tested three separate models to build the final model; the first model looked at HIV-related stigma and its association with QOL, the second examined depression as a potential mediator of the relationship between HIV-related stigma and QOL, and finally, we tested the full model (Fig. 1). In the first model (not shown), we found that HIV-related stigma was associated with poorer QOL (estimate: −0.232, standard error (SE): 0.069, critical ratio (CR): −3.353, p < .0001, standardized regression weight: −0.333). When we added depression as a potential mediator of the association between HIV-related stigma and QOL in the second model (not shown), HIV-related stigma was still significantly associated with QOL (estimate: −0.125, SE: 0.059, CR: −2.125, p = .034, standardized regression weight: −0.181), but its strength was reduced, suggesting partial mediation. Depression was also significantly associated with QOL (estimate: −0.219, SE: 0.034, CR: −6.464, p < .001, standardized regression weight: −0.540)
In the final structural equation model, we simultaneously estimated coefficients for HIV-related stigma, racial discrimination, social support, depression, and QOL (Fig. 2). The model fit was good: χ 2 = 203.266, DF: 112, p < .0001, CFI: 0.929, TLI: 0.912, RMSEA: 0.071. The significant chi-square result suggests that there is a difference between the hypothesized model and the data; however, the CFI, TLI, and RMSEA indices support the model as a good fit with the data. The coefficients in the final model are presented in Table 3. When social support was added as a potential mediator, the association between HIV-related stigma and QOL was no longer significant, suggesting full mediation. HIV-related stigma was associated with higher depression (standardized estimate: 0.215, p = .015) and lower social support (standardized estimate: −0.302, p = .001), but was not significantly associated with QOL (standardized estimate: −0.018, p = .824). HIV-related stigma had a significant indirect effect on QOL (standardized estimate: −0.241, p = .009); with an increase in HIV-related stigma by 1 SD, QOL is reduced by 0.241 SD.
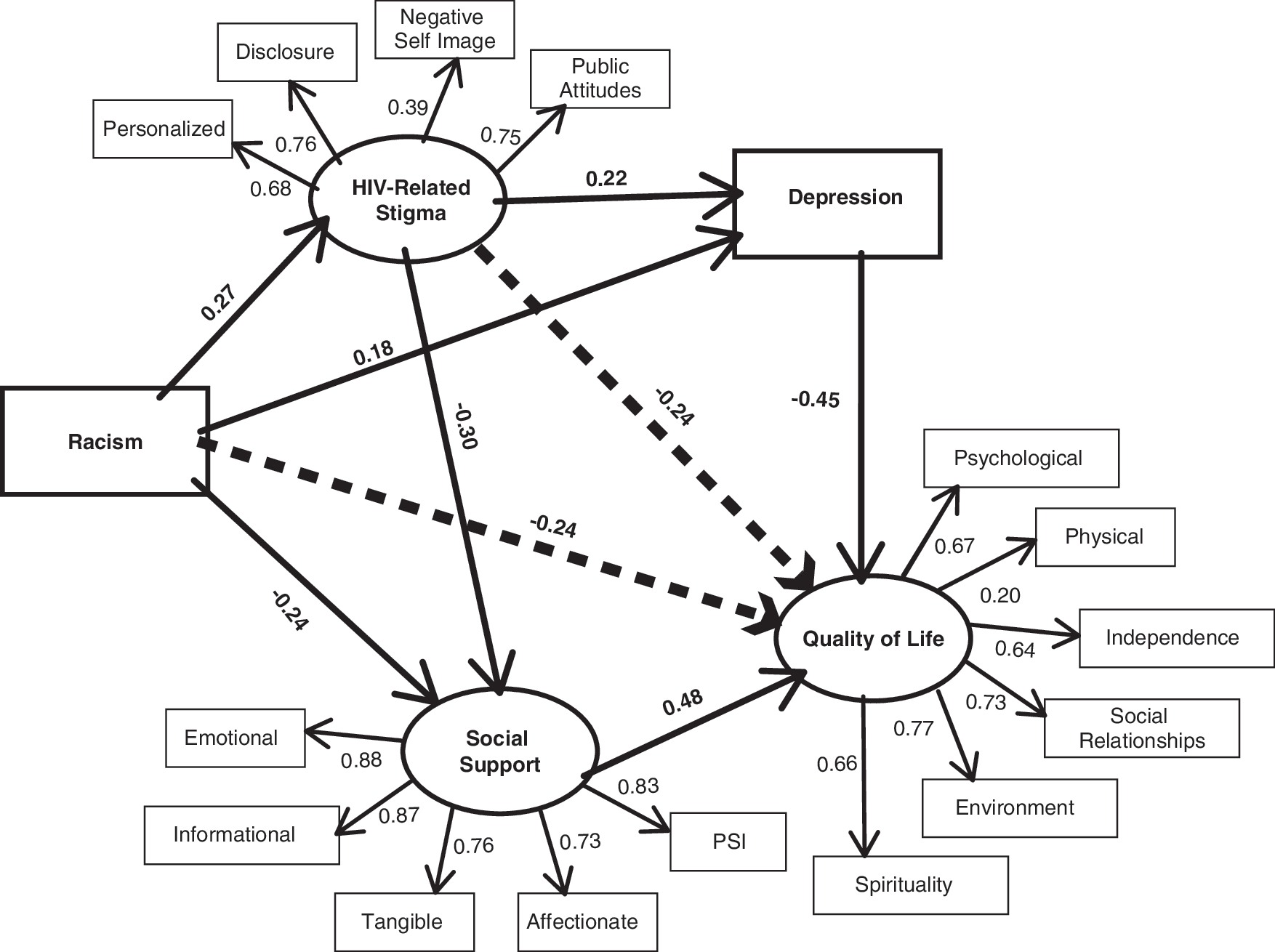
Final model of factors contributing to quality of life among African and Caribbean women living with HIV in Ontario (n = 166).
Racial discrimination was associated with higher HIV-related stigma (standardized estimate: = 0.268, p = .002), higher depression (standardized estimate: = 0.180, p = .012), and lower social support (standardized estimate: = −0.241, p = .002). Racial discrimination was not significantly associated with QOL (standardized estimate: = −0.086, p = .211). However there was an indirect effect of racial discrimination on QOL (standardized estimate: −0.241, p = .019); an increase in racial discrimination by 1 SD contributed to a reduction in QOL by 0.266 SD. Social support was associated with higher QOL (standardized estimate: = 0.480, p < .001), and depression with lower QOL (standardized estimate: = −0.449, p < .001).
Discussion
To our knowledge, this is the first study to model the relationship between HIV-related stigma, racial discrimination, and QOL among WLWH. Most studies examining stigma and its association with QOL among PLHIV have examined correlations between HIV-related stigma and HRQoL. Our study builds on this knowledge base by using SEM techniques to further explore associations between a multidimensional measure of QOL and look at HIV-related stigma in concert with racial discrimination, among ACB WLWH. We also tested social support and depression as mediators of the relationship between stigma/discrimination and QOL: this has implications for interventions to promote QOL among ACB WLWH.
We found that HIV-related stigma and racial discrimination had significant direct effects on depression and social support, and indirect effects on QOL. These findings corroborate prior research which highlights that HIV-related stigma is negatively associated with QOL 31,44 and social support, and positively associated with depression. 20 HIV-related stigma contributes to feelings of social isolation, and subsequently, exacerbates depression, and compromises well-being. 5 While we did not locate studies that examined associations between racial discrimination and QOL among PLHIV, our finding is congruent with systematic reviews that demonstrate deleterious impacts of racism on health and well-being. 21,45
Social support and depression mediated the association between HIV-related stigma and QOL. These findings align with prior research. Social support has been widely associated with reduced HIV-related stigma as well as positive health outcomes. 31,46 Social support group participation has positive influences in retention in treatment and care, mortality and morbidity, and QOL among PLHIV. 28,34 Conversely, HIV-related stigma may compromise access to social support 47 ; PLHIV with higher internalized HIV-related stigma may also be less likely to attend a support group. 48 Depression is associated with HIV-related stigma 47 –49 and reduced HRQoL. 31,50 Depression reduces HRQoL as it negatively impacts daily living activities and mental health, and is linked with physical health issues such as decreased appetite and sleep. 31 It is therefore important to examine the complex interplay between social contexts (HIV-related stigma, social support) and health outcomes (depression, QOL).
Racial discrimination was associated with lower social support and increased HIV-related stigma. Studies have explored how racism weakens the ability to develop healthy relationships with peers, reducing social capital and consequently harming well-being. 51 Racism also promotes social distancing that can contribute to anxiety about cross-racial interactions. 51 Others posit that social support may buffer the effects of racism, allowing people to understand racism as a shared experience, providing ways for people to cope with and respond to racism, and being involved in positive experiences can mitigate the negative impact of stress, including racism. 52 Further research using longitudinal designs should explore racial discrimination and pathways by which it is connected with lower social support among ACB WLWH.
The finding that racial discrimination was associated with increased HIV-related stigma corroborates prior research, which demonstrated that Black WLWH in Ontario experienced among the highest HIV-related stigma in comparison with other PLHIV. 33 Racist stereotypes have been embedded within HIV-related stigma since the epidemic's beginning, when HIV was socially constructed as a “Haitian/African” disease. 53 –56 Findings from a study on differences in perceptions and experiences regarding HIV-related stigma between White and Black participants found that Black participants were attuned to discrimination—regardless of their HIV serostatus. 57 These findings highlight the need to further assess intersectional stigma among WLWH, 9 and future research could measure stigma associated with other intersecting identities, including poverty, mental health, sex work, sexual orientation, and gender identity, among others.
Our findings, in conjunction with prior research, underscore the salience of addressing both social support and HIV-related sigma among PLHIV to promote QOL. Prior work with PLHIV found instrumental social support and perceived that community support from organizations buffered the impact of anticipated HIV-related stigma on HIV symptoms, 58 highlighting the importance of considering multiple sources of social support and their relationship to QOL. Interventions aimed at reducing HIV-related stigma and racial discrimination have the potential to improve health and overall QOL among PLHIV. A recent systematic review of stigma reducing interventions for ACB WLWH revealed limited interventions that assessed multiple forms of stigma and discrimination, such as racism and HIV-related stigma. 5 Future studies should explore the causal pathways by which ACB WLWH who experience more racial discrimination also experience more HIV-related stigma.
There are several study limitations. Due to the small sample size, nonprobability sample and cross-sectional design, generalizability is limited. Future studies should use larger, more representative samples of ACB WLWH. Survey participants were recruited from organizations providing social support, and therefore could represent WLWH who are more isolated and experience greater stigma and depression. Conversely, it is possible that ACB WLWH who experience greater stigma would be less likely to access HIV-specific services, and we could therefore be missing perspectives from WLWH who are more isolated. We assessed social support as a mediator; as prior research has highlighted that different sources of social support may moderate the impacts of HIV-related stigma on health, 58 future research could examine social support as both a moderator and mediator of the influence of HIV-related stigma on QOL, and explore multiple sources of social support. The racial discrimination measure did not consider the multiple dimensions of stigma integrated in the HIV-related stigma latent construct. We did not assess HIV clinical outcomes (e.g., CD4 count, viral load) and their association with QOL, and this is an important area for future research. Future research should use scales that capture latent constructs of racism that include dimensions such as internalized, enacted, and perceived racial stigma and discrimination.
Conclusion
Study findings reinforce the importance of attending to racial discrimination, in addition to HIV-related stigma, to understand QOL among WLWH. The associations between racial discrimination and HIV-related stigma highlight the urgency to address racism and HIV-related stigma and the ways in which racism is reproduced in HIV discourse, media representations, and constructions. Causal pathways to QOL are complex, and QOL is produced by a combination of cumulative influences. 31
Interventions require multilevel tactics to promote QOL among ACB WLWH. On an intrapersonal level, addressing internalized stigma and depression can contribute to improved QOL. 31 Interpersonal interventions could involve social support groups; these groups should address the links between racial discrimination and HIV-related stigma. 5 Social support interventions could be multilevel and target significant others as potential sources of instrumental support, as well as community agencies as a source of collective support. 58 Community-level campaigns can aim to reduce HIV-related stigma through a combination of factors and pay particular attention to challenging racist stereotypes embedded within HIV stigma. 55 On a structural level, healthcare providers and ASOs can be trained to address racial discrimination and HIV-related stigma in healthcare and policy. Understanding the complexity of stigma, and pathways that lead to QOL, can result in creative change processes to promote health and well-being among ACB QOL.
Footnotes
Acknowledgments
We acknowledge all of the women who participated and shared their time, knowledge, and experiences as peer research assistants and survey participants. We are grateful to the E.D., staff, and research coordinators at Women's Health in Women's Hands Community Health Centre and other community collaborators, including the Black Coalition for AIDS Prevention (BlackCAP). This study was supported by grants from CIHR, the Canadian Institutes of Health Research, as well as funds from the Ontario AIDS Bureau and the Ontario Ministry of Health and Long-Term Care. The funders had no role in study design, data collection, and analysis, decision to publish, or preparation of the article.
Author Disclosure Statement
No competing financial interests exist.