
Abstract
Little information is available on the molecular epidemiologic profile of HIV-1 in French Guiana, the French department with the highest HIV/AIDS incidence. To follow the evolution of HIV-1 diversity, we carried out a molecular analysis of HIV-1 isolates from 305 treatment-naive patients between 2006 and 2012. Protease and reverse-transcriptase sequences were obtained for subtype characterization, polymorphism analysis, and identification of drug resistance mutations. Of 305 HIV-1 strains, 95.1% were subtype B viruses. The overall prevalence of transmitted drug-resistance mutations (TDRMs) was 4.6% (14/305), ranging from 1.9% to 7.1% depending on the year. This study shows a low level of HIV-1 genetic diversity and a moderate prevalence of TDRMs with no evidence of an increasing trend over the study period. Nevertheless, the strong genetic polymorphism observed on both genes may be of concern for long-term treatment of people living with HIV-1 and thus deserves continuous monitoring.
Introduction
I
Materials and Methods
This study was a retrospective analysis of 305 treatment-naive HIV-1 patients followed in French Guiana between 2006 and 2012. Samples came from two hospitals: Cayenne (Centre Hospitalier Andrée Rosemond, CHAR) and Saint-Laurent-du-Maroni (Centre Hospitalier de l'Ouest Guyanais, CHOG). These two centers give specialized care for ∼75% of the known HIV-infected patients in French Guiana.
For each patient, the variables extracted were age, sex, plasma HIV-1 RNA load at the time of sampling (or within a 3-month time frame before or after sampling), CD4 cell count at the time of sampling (or within a 3-month time frame before or after sampling), and antiretroviral (ARV) treatment at the time of sampling and hospital.
The inclusion criteria were HIV-1-positive patients, aged 18 years or older, naive of ARV treatment, with a CD4 cell count equal to or above 350/mm3, and for whom a genotypic resistance test had been requested by the physician at the time of the diagnosis (all patients are expected to get an initial pretreatment genotype). This CD4 threshold corresponds to the threshold for initiation of HIV-1 treatment under the 2010 WHO ARV treatment guidelines. This threshold was also slightly above the median CD4 count at the time of diagnosis (301/mm3) (M. Nacher, pers. comm.) and was a compromise between having sufficient patient numbers to obtain precise estimates (a CD4 count at 500 cells/mm3 would have eliminated over 75% of the patients) and analyzing the new patients with presumably the most recent infections. Patients for whom the concomitant analysis of the protease (PR) and reverse transcriptase (RT) sequences was not possible were excluded.
This study was approved by the Clinical Research Committee from the Institut Pasteur (CoRC No. 2014-16) and was conducted in accordance with French laws and regulations. No research-specific blood collection was performed for the study. All analyzed data resulted from diagnostic procedures required for the follow-up of HIV-1-infected patients. The epidemiologic data required for the study were extracted directly from eNadis®, a computerized medical record for specialty care and monitoring of patients infected with HIV-1 or hepatitis. All patients were informed of the possible use of data entered in eNadis for epidemiological and clinical research and provided written consent. The eNadis database is approved by the Commission Nationale de l'Informatique et des Libertés, the French regulatory authority for computerized databases.
PR and RT gene sequences were recovered from the Institut Pasteur de la Guyane. They were generated as follows: blood was collected in ethylene diamine tetraacetic acid tubes, and plasma was separated and stored at −80°C until RNA extraction. RNA was isolated from 1 ml of plasma with the NucliSENS® easyMAG® (bioMérieux, Marcy l'Etoile, France) as recommended by the manufacturer. RNA was then reverse transcribed to cDNA and amplified for partial RT and PR genes using the ANRS (Agence Nationale de Recherche sur le Sida) consensus sets of primers (
The PR and RT nucleotide sequences obtained were aligned using MEGA5 software with known reference sequences of group M pooled from the HIV-1 database (
To predict the susceptibility to available protease inhibitors (PIs), nucleos(t)ide reverse transcriptase inhibitors (NRTIs) and non-nucleoside reverse transcriptase inhibitors (NNRTIs), PR and RT sequences were analyzed using the French ANRS HIV-1 genotypic drug resistance algorithm version 24, updated in September 2014 (
The WHO list for surveillance of DRMs was used to estimate the prevalence of TDR. 3 The overall prevalence of TDR was defined as the percentage of isolates carrying any mutation indicative of TDR. To determine if there was a significant temporal change in the prevalence of TDRMs, the linear trend chi-square was used.
Results
In the context of our diagnostic activity, we performed thousands of HIV-1 genotypic resistance tests prescribed by Cayenne and Saint Laurent Hospitals between 2006 and 2012: 745 were performed for HIV-1-positive drug-naive patients. Among them, 305 patients (40.9%) had a CD4 count ≥350 cells/mm3 and met all inclusion criteria. Most of them were from Cayenne Hospital (79.0%, n = 241) and the rest were from Saint Laurent Hospital (21.0%, n = 64). With the exception of viral load, which was only obtained for 96.4% of the patients (n = 294/305), equally for females (97.6%; n = 163/167) and males (94.9%, n = 131/138), the rest of the collected data (age, sex, CD4 count, and naive ARV status) were obtained for all patients.
Age ranged from 19 to 77 years with a median age of 36 years. The median viral load (log10 copies/ml) was 4.16 (range: 1.32–7.00), and the median CD4 count (cells/mm3) was 500 (range: 350–2,901). The characteristics of the study population are presented in Table 1. There were as many males as females. Females, who are systematically screened during pregnancy, tended to be younger and to have higher CD4 counts and lower viral loads.
The values are presented as median (range).
HIV-1 subtype determination showed that subtype B accounted for 95.1% of the samples studied (n = 290/305), followed by F (1.3%, n = 4), A (0.3%, n = 1), C (0.3%, n = 1), and K (0.3%, n = 1) subtypes and B/F (0.3%, n = 1) intersubtype recombinants. Among the circulating recombinant forms (CRF), CRF02_AG (1.6%, n = 5) and CRF01_AE (0.7%, n = 2) were identified.
All sequences were analyzed for polymorphism, which was defined as any amino acid change compared to the subtype B consensus sequence HXB2 (Tables 2 and 3). For PR, alignment of the 290 subtype B sequences showed that overall, 61 of 99 (61.6%) amino acid positions presented at least one polymorphism each. In particular, V3 proved to be highly polymorphic with 99.7% of sequences mutated, followed by L63 (80.3%), S37 (75.5%), R41 (58.3%), V77 (40.7%), E35 (30.0%), I15 (29.7%), T12 (27.6%), M36 (26.6%), and I64 (26.2%). Other polymorphic positions were present in less than 25% of cases (Table 2). RT sequences were also highly polymorphic with 151 of 250 (60.4%) amino acid positions presenting at least one polymorphism each. Substitutions found in more than 25% of the study subjects occurred at the L214 (69.0%), E122 (66.2%), Q207 (62.8%), R211 (60.0%), T200 (54.8%), V245 (40.0%), S162 (39.0%), I135 (34.1%), V35 (28.6%), D177 (28.6%), and I178 (25.5%) positions (Table 3). Polymorphic positions on PR and RT of the other subtypes, for which we have far fewer isolates, are not listed here but are presented in Tables 2 and 3, respectively.
n, number of strains.
The gray boxes concern polymorphic positions (>25%) and the boxed columns point to the positions of resistance mutations according to the French ANRS algorithm, version 24, September 2014.
ANRS, Agence Nationale de Recherche sur le Sida; CRF, circulating recombinant forms.
n, number of strains.
The gray boxes concern polymorphic positions (>25%) and the boxed columns point to the positions of resistance mutations according to the French ANRS algorithm, version 24, September 2014.
Drug resistance mutations for PR and RT are presented in bold in Tables 2 and 3, respectively. We determined that 288 out of the 305 patients (94.4%) had viruses harboring DRMs on PR and/or RT. PI mutations were detected in 92.8% of isolates (n = 283/305). The most commonly identified were L63P (45.9%), V77I (39.3%), I15V (29.8%), and M36I (27.5%) followed by I62V (24.3%), H69Q (16.7%), and D60E (14.1%). Additional low-prevalence (<10%) PI-DRMs were found (Table 2). These substitutions corresponded to secondary mutation positions to PIs. Major mutations, such as M46I, V82A, and L90M, which affect the resistance to ARV drugs, were found at a low prevalence (0.3% each, n = 1). NRTI and NNRTI mutations were detected in 24.9% of patients (n = 76/305). A98S (8.2%) and V179I (7.2%) were the two most commonly observed. Additional RTI-DRM positions were identified but at a lower prevalence, below 2% (Table 3). Many of these low-prevalence mutations—K101E, K103N, E138A, M184I, Y188H, G190E, and M230I—correspond to major mutations associated with resistance to one or more ARV drugs.
Of the 305 patients tested, 18 exhibited viruses with drug resistance mutations to at least one ARV drug. All of them were of the B subtype. There were 66.7% females (n = 12) and 33.3% males (n = 6). However, this difference was not statistically significant (p = .3, χ 2 test). Table 4 presents the genotypic profile of the 18 isolates. Three isolates presented a mutation to a PI: two to IDV and one to NFV. Two others presented substitutions at polymorphic positions whose combination confers a resistance to TPV for the first one and to SQV for the second one. These five isolates presented mutations to only one PI and none to RTI. Two isolates presented NRTI mutations (T69D+K219Q) associated with a resistance to DDI without resistance to any other class of ARV. Eight isolates bore NNRTI-resistant mutations: five to EFV+NVP, two to RPV, and one to EFV+NVP+RPV. These eight isolates only presented NNRTI mutations. The last three isolates had mutations associated with resistance to NRTI FTC +3TC plus another NNRTI resistance: EFV+NVP or RPV or EFV+NVP+RPV. No isolate had mutations to the three classes of drugs, NRTI, NNRTI, and PI.
Major resistance mutations are in bold.
According to the French ANRS algorithm, version 24, September 2014.
NRTI, nucleos(t)ide reverse transcriptase inhibitor; NNRTI, non-nucleoside reverse transcriptase inhibitor; PI, protease inhibitor; PR, protease; RT, reverse transcriptase; VL, viral load (log10 copies/mm3).
According to these results, the overall prevalence of TDRM was 4.6% (14/305) in our cohort, ranging from 1.9% to 7.1% depending on the year (Fig. 1). Based on the WHO list, four of the 18 isolates carrying a DRM to at least one drug were excluded: the two isolates (KT998118 and KT998206) presenting a PI resistance due to a combination of mutations on polymorphic positions on PR not indicative of TDR as well as the two (KT998027 and KT998252) bearing the E138A mutation, given that this position is polymorphic. The prevalence of PI, NRTI, first-generation NNRTI (EFV, NVP), and RPV drug resistance mutations was 1.0%, 1.6%, 2.6%, and 1.0%, respectively. There was no statistical trend over the period considered (p = .69 for all resistance statistics and p = .53 for NNRTI, linear trend χ 2).
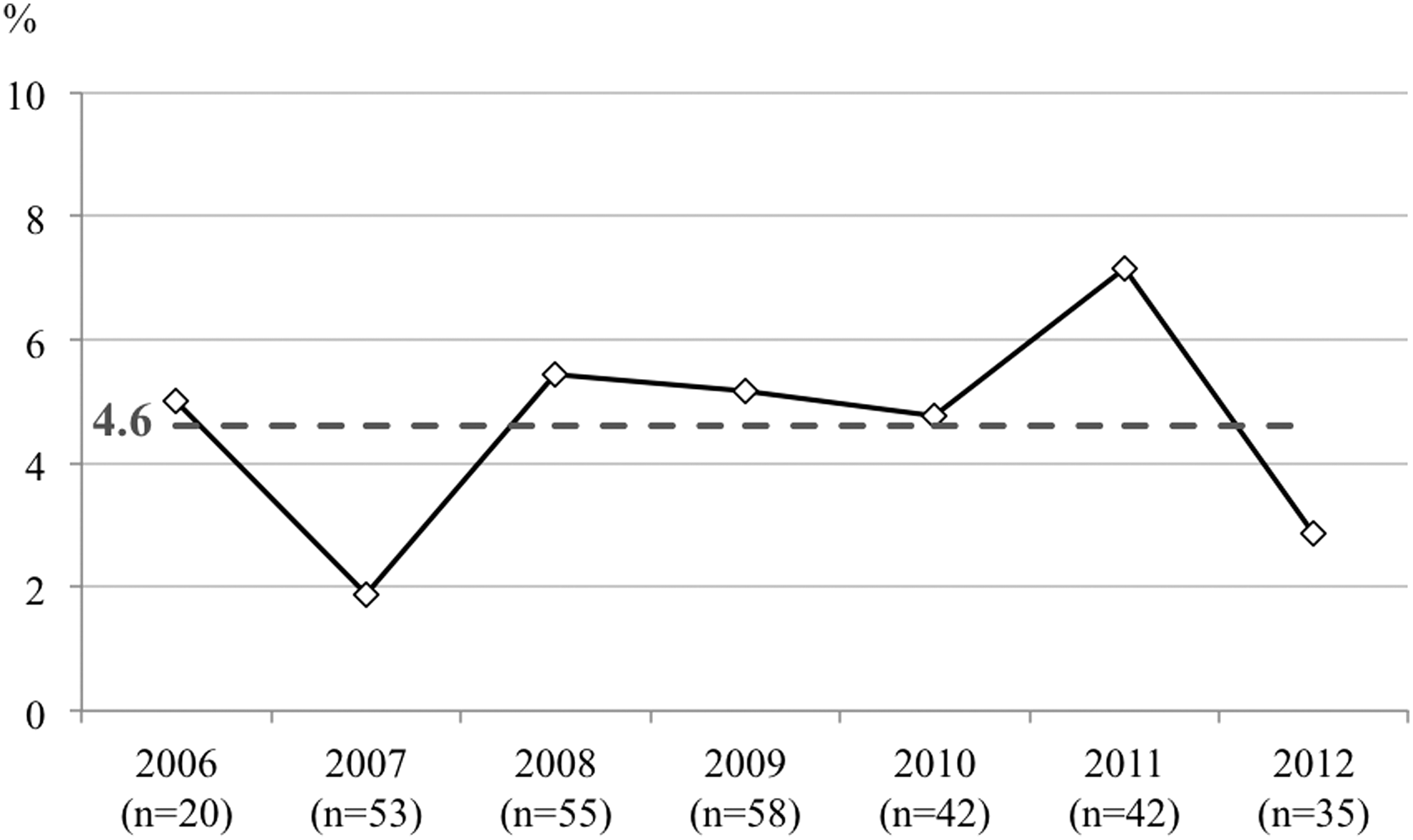
Transmitted drug resistance prevalence (% per year). The dotted line represents the prevalence (%) for the 2006–2012 period. The number of patients was between 20 and 58 depending on the year. n stands for the number of patients.
Discussion
To participate in the improvement of the public health response to the HIV-1 epidemic in French Guiana, since the end of 2005, the Institut Pasteur de la Guyane has implemented the genotypic resistance test of HIV-1 against ARV. Thousands of analyses were subsequently requested by the two main hospitals in French Guiana, of which about 10% concerned drug-naive patients. Since a large proportion of patients (33% in 2013) were diagnosed late (CD4 ≤ 200/mm3), only 305 patients, accounting for 40.9% of the initial drug-naive population, met the inclusion criteria and were included in the study. 1 Despite these constraints, the characteristics of this cohort were similar to French Guiana's overall HIV-1 population in terms of the proportion of men and women as well as age. 1 This study thus allowed us to document the circulating HIV-1 subtypes and to present, to our knowledge, the first data on TDR in HIV-1-infected individuals in French Guiana. Given the intense migrations through the Guiana shield and beyond, these results may reflect broader regional trends.
Although migrations (80% of patients are immigrants) may lead to temporal evolution of the HIV-1 subtypes in the region, the analysis showed that subtype B still predominated, accounting for more than 95% of subtypes, as was reported 15 years ago. 2 The remaining 5% exhibited F, A, C, and K subtypes, the B/F intersubtype, as well as CRF02_AG and CRF01_AE. Our proportion of subtypes was coherent with recent publications in neighboring countries showing that HIV-1 subtype B was the most prevalent in Latin America and the Caribbean, although subtype C and B/F recombinants have made significant contributions. 4 –6 This stability of HIV-1 subtypes in French Guiana is in agreement with the fact that even if the migratory flux can substantially vary according to socioeconomic or political issues from 1 year to another, the main migratory sources (Haiti, Brazil, Suriname, and Guyana) remain the same over time.
The prevalence of TDR is highly variable worldwide, with rates ranging from 0% to over 25%. 6 The highest prevalence rates are reported in countries with a long-standing use of ARV therapy. In addition, during the last 10 years, the number of resistant strains has increased over time in these countries. 6,7 We report here an average prevalence of 4.6%, which is coherent with the prevalence described in Latin America and the Caribbean, ranging from 0% to 12% depending on the year and drug prescription patterns. 6 –8 The yearly TDR prevalence in French Guiana fluctuated between 1.9% and 7.1%. Although it reached 7.1% in 2011, no significant trend was observed. However, the limited number of patients infected with a virus harboring DRM per year in our cohort (one to three per year) and the 7-year period may have been insufficient to detect a gradual increase of TDR.
For PR, the high degree of polymorphism at key amino acid positions known to be associated with drug resistance in HIV-1 subtype B is thus a concern for long-course PI treatment of people living with HIV. For NRTI, the M184I transmitted drug mutation (TDM), which confers high-level resistance to 3TC and FTC, was observed in three isolates. With M184V, this is the most commonly reported NRTI TDM in HIV-1 B subtype in the regions of the world where highly active antiretroviral treatment has been used for years, as in French Guiana. Nevertheless, for two of the three isolates, the M184I was associated with the M230I mutation. Co-occurrence of these two mutations in the same sample suggests that they may have been generated through APOBEC3G/F editing. 9 Finally, most isolates bearing TDM (64%) presented NNRTI resistance to EFV and NVP and to RPV. Among them, the K103N mutation was observed in five isolates. These results are consistent with other studies showing that K103N is one of the most commonly transmitted mutations. 6,7 A high correlation has been demonstrated between the prevalence of NNRTI TDM in drug-naive patients and the ARV-treated individuals in the same region. 7,10 Moreover, recent data pointed out the existence and the impact of low-frequency NNRTI-resistant mutations on future virologic failures. 11 –14
In conclusion, in the context of social and adherence difficulties, and of migrations from countries with a limited number of ARVs, the concern was that resistant viruses would be increasingly frequent in French Guiana. The present study shows that the prevalence of ARV resistance is consistent with other studies conducted in Latin America and that there is no evidence of an increasing trend. Nevertheless, this study also reveals a strong genetic polymorphism on both genes. Taken together, these results imply that PR and RT DRMs deserve continuous attention in the future, notably in treatment-naive individuals, to optimize first-line ARV regimens in this territory.
Footnotes
Acknowledgments
This work was funded by the Institut Pasteur de la Guyane. It has also benefited from a European commission REGPOT-CT-2011-285837-STRonGer grant within the FP7. The authors thank Nathalie Jolly from the Institut Pasteur Clinical Research Department (PIRC, Pôle Intégré de Recherche Clinique) for her help in the ethical aspects of the project. They also thank Ketty Bienvenu, Lidia Saint Louis, Sergine Soyon, and Karine Verin for their invaluable assistance.
Sequence Data
The GenBank accession numbers for the sequences are KT998002 to KT998288 and KU052741 to KU052759.
Author Disclosure Statement
No competing financial interests exist.