
Abstract
Papua and West Papua provinces have the highest prevalence rate of human immunodeficiency virus type 1 (HIV-1) infection in Indonesia; however, data on the molecular epidemiology of HIV-1 are limited. We conducted a genotypic study on HIV-1 genes derived from antiretroviral therapy-naive individuals residing in Sorong, West Papua. HIV-1 genomic fragments were amplified from 43 peripheral blood samples, and sequencing analysis of the genes was carried out. Of the 43 samples, 41 protease (PR), 31 reverse transcriptase (RT), 26 gag, and 25 env genes were sequenced. HIV-1 subtyping revealed that CRF01_AE (48.8%, 21/43) and subtype B (41.9%, 18/43) were the major subtypes prevalent in the region, whereas other recombinant forms were also detected. Major drug resistance-associated mutations for PR inhibitors were not detected; however, mutations for the RT inhibitors, A62V and E138A, appeared in a few samples, indicating the possible emergence of transmitted HIV-1 drug resistance in Sorong, West Papua.
A
HIV-1 is characterized by extensive genetic heterogeneity and is divided into four groups: M (major), O (outlying), N (new or non-M, non-O), and P (pending). The viruses in group M are further classified into a number of subtypes and circulating recombinant forms (CRFs). Of these, subtypes A, B, C, D, and G, as well as CRF01_AE and CRF02_AG, are the major subtypes and CRFs responsible for the worldwide HIV-1 pandemic. 4 Although subtype B of HIV-1 is the predominant subtype in the Americas, Europe, and Australia, there is a growing epidemic of non-B subtypes and CRFs in Africa and Asia. CRF01_AE is prevalent throughout Southeast Asia 4 and is responsible for more than 90% of infection cases in Indonesia. 5 In addition, several recombinant forms between CRF01_AE and subtype B, including CRF33_01B, have emerged in Indonesia. 6,7 Different subtypes and CRFs are considered to show different rates of disease progression, immune responses, responses to antiretroviral therapy (ART), and/or the development of drug resistance 8 ; therefore, it is important to monitor the global prevalence of subtypes and CRFs for HIV prevention and control as well as for vaccine development.
ART has successfully reduced the viral transmission of as well as morbidity and mortality associated with HIV. In Indonesia, 510,000 individuals, whose CD4+ T-cell count was <500 cells/mm3 (WHO criteria), were estimated to be eligible for ART in 2013. The Indonesian national ART program enabled 40% of these individuals to access ART in 2011. 9 The first-line regimen of ART recommended in Indonesia is a combination of two nucleoside reverse-transcriptase inhibitors (NRTIs) and a non-NRTI. Lamivudine (3TC), zidovudine (AZT), tenofovir (TDF), nevirapine (NVP), and efavirenz (EFV) are commonly used. In patients with virological failure or adverse effects, ritonavir-boosted protease inhibitors in combination with two NRTIs are recommended as the second-line regimen. Other drugs, including didanosine (ddI), etravirine (ETR), and rilpivirine (RPV), are uncommon in Indonesia. Although ART is successful in Indonesia, the emergence of drug resistance has been reported among treatment-failure patients. 10 In addition, the emergence of transmitted drug resistance (TDR) as a consequence of ART expansion represents a serious public health issue because TDR affects treatment efficacy and clinical outcomes. 11 After a decade of ART expansion in Indonesia, the emergence of TDR is inevitable; however, limited data are available on TDR among HIV-1-infected individuals in this country.
To clarify the viral subtypes of currently circulating HIV-1 strains as well as to monitor the emergence of TDR in the West Papua province of Indonesia, we performed the genotypic characterization of viral genomes derived from the peripheral blood samples of HIV-1-infected, ART-naive individuals residing in Sorong, West Papua.
Forty-nine HIV-1-infected, ART-naive individuals (18 males and 31 females with a mean age of 31 years) were recruited from Sele be Solu Hospital in Sorong, West Papua. Ten milliliters of ethylenediaminetetraacetic acid (EDTA) anticoagulated peripheral blood samples were collected from participants between April 2014 and August 2014. Plasma was then isolated from peripheral blood samples by centrifugation for 10 min at 2,000 rpm. In addition, peripheral blood mononuclear cells (PBMCs) were isolated by density gradient centrifugation using Histopaque 1077 (Sigma-Aldrich, St. Louis, MO). RNA and DNA were extracted from plasma and PBMCs using the QIAamp Viral RNA Mini kit (Qiagen, Hilden, Germany) and GenElute Mammalian Genomic DNA Miniprep kit (Sigma-Aldrich), respectively.
The viral pol genes encoding protease (PR) (PR gene) and reverse transcriptase (RT) (RT gene) as well as partial fragments of the gag and env genes were amplified from DNA extracted from PBMC samples by a nested polymerase chain reaction (PCR) using Ex Taq (Takara Bio, Shiga, Japan) and the following primers. For the amplification of PR gene, the primers for the first PCR were DRPR05, 5′-AGACAGGYTAATTTTTTAGGGA-3′ [corresponding to nucleotide (nt) 2074–2095 of the HIV-1 reference strain, HXB2 (GenBank Accession No. K03455)] and DRPR02L, 5′-TATGGATTTTCAGGCCCAATTTTTGA-3′ (nt 2716–2691), whereas the primers for the nested PCR were DRPR01M, 5′-AGAGCCAACAGCCCCACCAG-3′ (nt 2148–2167) and DRPR06, 5′-ACTTTTGGGCCATCCATTCC-3′ (nt 2611–2592). For the amplification of RT gene, the primers for the first PCR were RT1L, 5′-ATGATAGGGGGAATTGGAGGTTT-3′ (nt 2388–2410) and GPR2M, 5′-GGACTACAGTCYACTTGTCCATG-3′ (nt 4402–4380), whereas the primers for the nested PCR were RT7L, 5′-GACCTACACCTGTCAACATAATTGG-3′ (nt 2485–2509) and GPR3L, 5′-TTAAAATCACTARCCATTGYTCTCC-3′ (nt 4309–4285). For the amplification of gag gene encoding Gag p24, the primers for the first PCR were H1G777, 5′-TCACCTAGAACTTTGAATGCATGGG-3′ (nt 1231–1255) and H1P202, 5′-CTAATACTGTATCATCTGCTGCTCCTGT-3′ (nt 2352–2325), whereas primers for the nested PCR were H1Gag1584, 5′-AAAGATGGATAATCCTGGG-3′ (nt 1577–1595) and G17, 5′-TCCACATTTCCAACAGCCCTTTTT-3′ (nt 2040–2017). For the amplification of the C2-V3 regions of the env gene, the primers for the first PCR were M5, 5′-CCAATTCCCATACATTATTGTGCCCCAGCTGG-3′ (nt 6858–6889) and M10, 5′-CCAATTGTCCCTCATATCTCCTCCTCCAGG-3′ (nt 7661–7632), whereas the primers for the nested PCR were M3, 5′-GTCAGCACAGTACAATGIACACATGG-3′ (nt 6948–6973) and M8, 5′-TCCTTCCATGGGAGGGGCATACATTGC-3′ (nt 7547–7521). We had also attempted to amplify viral gene fragments from plasma samples by reverse transcription-PCR essentially as described 12 ; however, the amplification failed and we attributed this to the inadequate preservation conditions used for the samples. The sequencing analysis of amplified viral gene fragments was performed using the BigDye Terminator v3.1 Cycle Sequencing kit with an ABI PRISM 3500xL genetic analyzer (Applied Biosystems, Foster City, CA). Sequencing data were then assembled and aligned using Genetyx version 10 software (Genetyx, Tokyo, Japan). Regarding the results obtained, sequencing data for the full length of 41 PR genes (297-bp; nt 2253–2549), the N terminus of 31 RT genes (762-bp; nt 2550–3311), the partial fragment of 26 gag genes encoding Gag p24 (382-bp; nt 1627–2008), and the partial fragment of 25 env genes spanning the C2-V3 region (389-bp; nt 7020–7408) were obtained from 43 blood samples. The nt sequences of these PR, RT, gag, and env genes have been deposited in the GenBank database under Accession Nos. KU596419–KU596541.
HIV-1 subtyping was performed using the recombinant identification program (RIP), which is available on the website of the HIV sequence database (
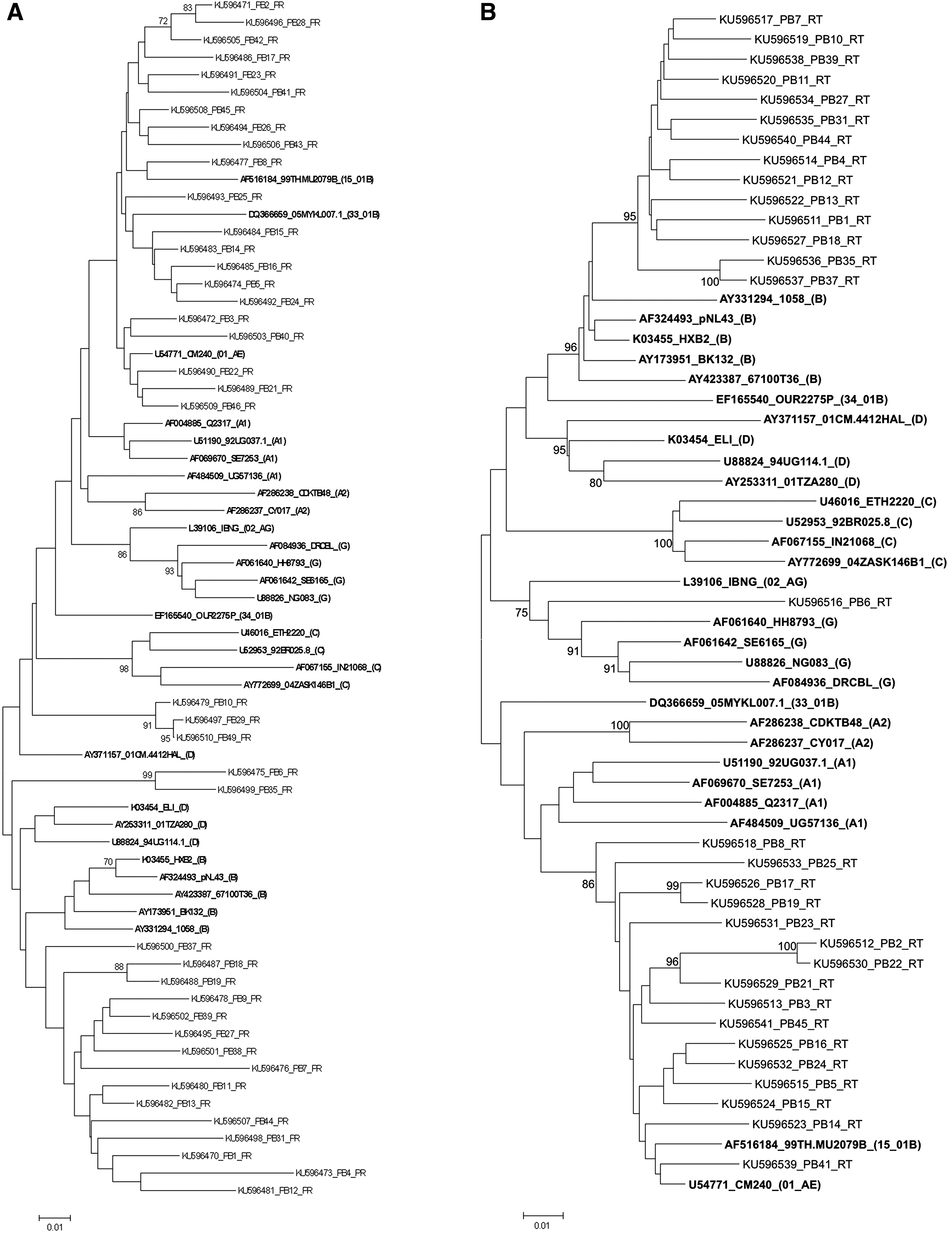
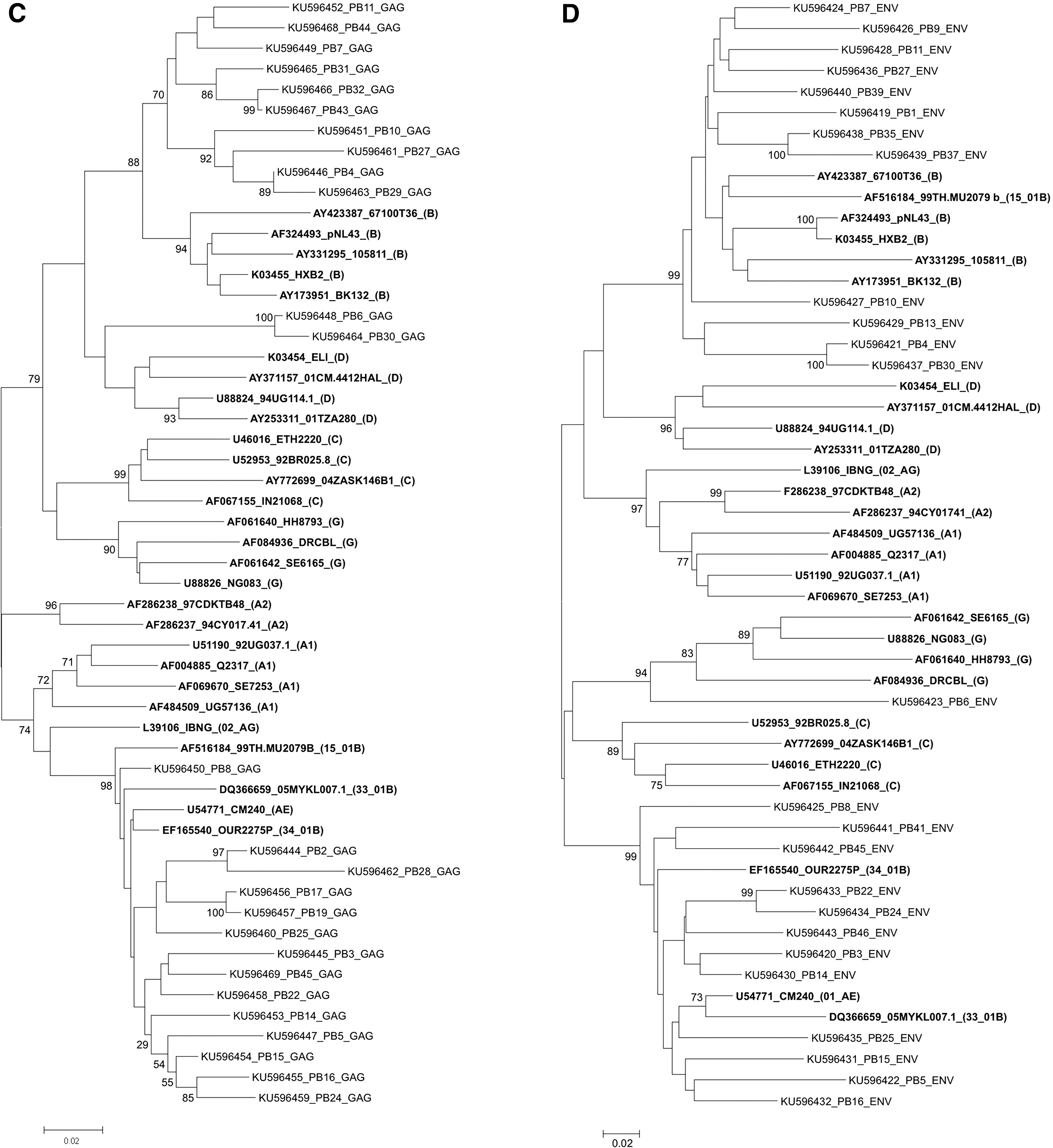
Phylogenetic analysis of HIV-1 PR, RT, gag, and env gene sequences. Phylogenetic trees were generated for the newly sequenced HIV-1 PR
The appearance of drug resistance-associated mutations in the PR and RT genes was studied according to the IAS-USA panel and WHO surveillance list. 14,15 TDR was defined as the presence of at least one major drug resistance mutation listed in the IAS-USA panel or surveillance drug resistance mutation in the WHO surveillance list. 14,15 In addition to TDR, drug resistance-associated minor mutations in the IAS-USA panel were manually detected. 14 In this study, drug resistance-associated major mutations to PR inhibitors were not detected. However, several drug resistance-associated minor mutations were detected in RR genes at various percentages: L10I/V (12.2%), G16E (12.2%), K20R/I (24.4%), L33I/F/V (7.3%), M36I (78.0%), D60E (7.3%), I62V (19.5%), L63P (48.8%), I64V/L (12.2%), H69K (48.8%), A71T (4.9%), L76V (2.4%), V77I (9.8%), L89M/I (58.5%), and I93L (17.1%) (Table 1). Mutations in the PR gene among ART-naive patients potentially affect viral susceptibility to atazanavir (ATV), darunavir (DRV), fosamprenavir (FPV), lopinavir (LPV), tipranavir (TPV), indinavir (IDV), nelfinavir (NFV), and saquinavir (SQV). 14 In addition, drug resistance-associated mutations in the RT gene appeared in five samples (Table 2). The drug resistance-associated major mutations were A62V (3.2%) and E138A (12.9%), whereas the minor mutations were V106I (3.2%) and V179D/T (9.7%) (Table 2). These mutations were associated with drug resistance to ETR or RPV or with multi-NRTI resistance. 14
The determination of drug resistance mutations was based on the guidelines published by the International AIDS Society United States (IAS-USA).
The subtype of PR genes was assigned based on RIP and phylogenetic analyses.
PR, protease; RIP, recombinant identification program.
The subtype of RT genes was assigned based on RIP and phylogenetic analyses.
The determination of drug resistance mutations was based on the guidelines published by the International AIDS Society United States (IAS-USA). Drug resistance-associated major mutations are shown in bold.
CRF, circulating recombinant form; ETR, etravirine; NRTI, nucleoside reverse-transcriptase inhibitor; nNRTI, non-nucleoside reverse-transcriptase inhibitor; RPV, rilpivirine; RT, reverse transcriptase.
In summary, the genotypic study revealed that CRF01_AE and subtype B were the major subtypes prevalent in Sorong, West Papua, and the proportion of subtype B viruses prevalent in the region appeared to be higher than that in other regions in Indonesia. In addition, recombinant forms including the viral gene fragments of CRF01_AE/subtype B, subtypes B/D, or subtypes C/D/G appeared in this region. Moreover, the drug resistance-associated major mutations, A62V (3.2%, 1/31) and E138A (12.9%, 4/31), for RT inhibitors appeared, suggesting the possible emergence of transmitted HIV-1 drug resistance in Sorong, West Papua. We consider continuous surveillance to detect TDR to be necessary in this region.
Sequence Data
Nucleotide sequences are available under GenBank Accession Nos. KU596419–KU596541.
Footnotes
Acknowledgments
This work was supported by the program of the Japan Initiative for the Global Research Network on Infectious Diseases (J-GRID) by the Japan Agency for Medical Research and Development (AMED) and the Institute of Tropical Disease as the Center of Excellence (COE) program by the Ministry for Research and Technology (RISTEK) of Indonesia. The article was proofread by Medical English Service, Kyoto, Japan.
Author Disclosure Statement
No competing financial interests exist.