
Abstract
Introduction
I
For almost 20 years, ART has been used as postexposure prophylaxis (PEP), a 28-day two- or three-drug treatment within 72 h after a sexual or parenteral potential exposure to HIV. Despite the lack of evidence regarding efficacy and effectiveness due to ethics and implementation difficulties, prescribing PEP is well accepted based on animal models and observational studies. 3,4 Awareness and use of PEP are considered low, even though, in a retrospective analysis, a Swiss cohort showed an increase of 850% in PEP demand during 10 years. 5 Dropouts have frequently been described and that problem could limit the potential preventive benefits of this prophylaxis. 6 –8 It has been suggested that PEP availability could attenuate risk perception, but no increase in risk behaviors has been demonstrated. 9
Another more recent preventive strategy using ART is pre-exposure prophylaxis (PrEP) with very encouraging outcomes in randomized clinical trials if high adherence is maintained. 10 –13 PrEP involves daily or intermittent one- or two-drug treatment during an extended period of time in anticipation of sexual or parenteral high-risk exposure. Although in United States this preventive strategy has been implemented with increasing uptake, in Europe it has not been approved yet. However, recent guidelines 14,15 recommend that in high-risk populations, prevention needs to be reinforced and PrEP should be considered. It seems reasonable that transition from PEP to PrEP in patients with repeated risk exposures is considered, 16 although nowadays there are no specific recommendations.
To our knowledge, there are few studies assessing predicting factors of HIV seroconversion among individuals attending a specialized HIV prevention center for HIV risk exposure. No tools have been developed to predict the probability of HIV seroconversion in the high-risk population seeking care at such center even after they have completed the recommended 6 months of follow-up. 17,18 These data would be useful to identify those individuals at a higher risk of infection and therefore facilitate implementation of a more suitable follow-up with probable recommendation of PrEP. The Hospital Clinic of Barcelona has an HIV Unit with a PEP program and, since 2003, it has become the reference center for individuals with HIV risk exposures (occupational, nonoccupational, and sexual assault) in the city. Until December 2013, we have followed up on 3,089 individuals who attended the clinic because of a possible HIV risk exposure and most of them received PEP treatment. We assessed factors associated with HIV seroconversion with the final aim to develop a tool to assess seroconversion probability in this population and improve prevention strategies.
Materials and Methods
Study design
We studied individuals from an HIV Unit's contact risk cohort at a tertiary care hospital in Barcelona, Spain, between 2003 and 2013 and performed a retrospective matched case–control study. To select cases, we crossed two databases of our center: one with 8,795 HIV-infected patients and the other with 3,089 HIV-uninfected individuals from our HIV contact risk cohort who had their first visit between 2003 and 2013. From this HIV-negative contact risk cohort database, we selected controls. Cases or seroconverters were defined as individuals who seroconverted after at least 3 months since first follow-up visit because of a potential HIV exposure, otherwise if an individual seroconverted earlier and PEP was prescribed, the case would be considered as treatment failure and not included in the study. Controls or seronegatives were defined as individuals who attended our center because they were at-risk contacts and to our knowledge, until this revision, were still HIV negative.
HIV-seronegative men and women came to our clinic by two different routes, from our center emergency room and from primary care centers (PCCs) because of a potential HIV risk exposure, as serodiscordant couples, random sexual risk contact, occupational exposure, or other parenteral exposure. All individuals were followed up according to AIDS Study Group recommendations Consensus of Spain. 19 They attended our center at least three times at baseline and at months 1 and 3 after exposure if they received PEP and at least twice, at baseline, and month 3 after exposure if PEP was not recommended. In every case, an additional 6-month visit was programmed. During follow-up laboratory, monitoring and counseling were performed. At least one HIV test and other tests for sexually transmitted infections (STIs) such as hepatitis C virus (HCV), hepatitis B virus (HBV), hepatitis A virus (HAV), and Syphilis were conducted for every individual. Counseling was offered at every follow-up visit and focused on preventative strategies and adherence reinforcement. Once follow-up had finished, we lost touch with uninfected individuals until they came back because of another exposure or confirmed HIV infection.
We pooled patients who had a record in both cohorts (n = 117) using a positive HIV third-generation enzyme-linked immunosorbent assay and positive Western blot as confirmation test. We excluded 48 patients with HIV diagnosed at contact risk baseline visit. The remaining 69 individuals were considered cases and were matched individually by gender, birth date, and date attending the clinic with 69 HIV-negative controls from the same HIV contact risk cohort.
Study population
Cases and controls were classified in two subgroups: patients who received PEP and patients reporting an HIV risk contact, but who did not receive PEP. We recorded demographics, serostatus of sexual partner, exposure risk classified according to the AIDS Study Group recommendations Consensus of Spain 19 (Appendix Table 1), PEP regimen prescribed, previous PEP and STI, previous HIV testing, and results of STI baseline test. In addition, for each case, we recorded elapsed time between first contact risk follow-up visit and HIV-positive test date and CD4 T-cell count and viral load (VL) at diagnosis. Information was collected from patients' medical records.
Statistical analysis
Data were collected from two separated sources: the HIV contact risk cohort for all individuals and the HIV-positive patients' database for cases. Descriptive statistics were calculated for continuous variables and were summarized by medians [interquartile ranges (IQRs)] and categorical variables summarized by frequencies and percentages. All demographic and behavioral data recorded from both cases and controls were compared using a McNemar test assessing factors associated with seroconversion. To establish a model for predicting probability of an HIV seroconversion in the studied population and to calculate a seroconversion index, we utilized clinically significant variables and conducted a logistic regression analysis (using backward conditional selection criteria). To evaluate goodness of fit, we conducted a Hosmer–Lemeshow test. Sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) were calculated. The receiver operating characteristics (ROC) curve was used to plot the sensitivity and 1-specificity of the different seroconversion indices. Patients were also clustered by median elapsed time between first follow-up date and HIV-negative and HIV-positive test date, and CD4 T-cell count and VL at this time point were compared.
Results
Clinical characteristics of HIV contact risk cohort
A total of 3,089 patients were followed up in our center between 2003 and 2013 because of a possible HIV risk exposure (occupational, nonoccupational, sexual assault) and 80% (n = 2,465) were referred due to a sexual exposure. Median age was 37 years, individuals were mainly men (62%, n = 1,927) who had sex with men (MSM) (53%, n = 1,628). Risk assessment was mostly moderate (40%, n = 1,235) and most patients received PEP (68%, n = 2,105).
Factors associated with HIV seroconversion
We found 117 (3.8%) individuals from our HIV contact risk cohort being followed in our HIV unit because an HIV-positive diagnosis (Fig. 1). In 48 individuals (1.5%), HIV infection was detected at the baseline visit, therefore excluded from analysis. The remaining 69 (2.2%) individuals seroconverted after a median (IQR) of 24 (9–34) months from baseline visit. Seroconverters were mostly men (96%, n = 66) with a median age of 35 years (IQR 30–40), and 7 (10%) had a concomitant STI when diagnosed. Among these 69 seroconverters, CD4 T-cell count at HIV detection was significantly higher in patients with HIV detected earlier [median (IQR) 527 (421–734) vs. 421 (317–540) cells/mm3 for patients with HIV diagnosed before (n = 35) and after (n = 34) the median time (24 months) from baseline visit, p = .01], while no differences were found in VL [mean (standard error) log10 copies/ml 4.21 (0.17) vs. 4.53 (0.17), respectively, p = .18].

Subject disposition.
As for both groups, no differences were observed regarding birth place, risk of exposure, PEP prescription, PEP drug regimen, hours from exposure to PEP prescription, PEP adherence, and coinfections at baseline (hepatitis A, B, and C or syphilis). Clinical characteristics of study population are shown in Table 1. Most patients in both groups were MSM, but proportion was higher among cases (94% vs. 70%, p < .0001). Cases also showed a higher proportion of risk contact with a known HIV partner (46% vs. 28%, p = .03), previous PEP use (19% vs. 6%, p = .03), previous STI (54% vs. 16%, p < .0001), and previous HIV testing (58% vs. 41%, p = .04). At baseline visit, we diagnosed two acute HBV infections among cases and one HCV acute infection in the control group that received specialized treatment if indicated. Correct vaccination against HBV was found in 50 (72%) cases and 44 (64%) controls (p = .36).
Case and controls were matched individually by gender, birth date, and date attending the clinic.
Exposure risk: for differences between high- and low-risk exposure, refer to Appendix Table 1.
Ab HBcore, antibodies core hepatitis B; Ab HBs, antibodies surface hepatitis B; Ag HBs, antigen surface hepatitis B; HAV, hepatitis A virus; HCV, hepatitis C virus; IQR, interquartile range; MSM, men who have sex with men; NA, not applicable; PEP, postexposure prophylaxis; STI, sexually transmitted infection.
Predictive factors associated with HIV seroconversion
We conducted a logistic regression analysis to assess factors independently associated with seroconversion after at least 3 months since first follow-up visit because of a potential HIV exposure. Being MSM [odds ratio (OR) 5.2 (1.4–20.2), p = .01], having had a known HIV-positive partner [OR 2.7 (1.2–6.2), p = .02], having previous PEP [OR 3.9 (1.0–15.6), p = .05], and having previous STI [OR 4.6 (1.9–10.9), p = .001] remained as factors independently associated with HIV seroconversion. We obtained the following formula: ln(odds VIH+) = −3.114 + 1.653 (MSM) +0.982 (known HIV positive partner) +1.369 (had previous PEP) +1.528 (previous STI). This analysis permitted us to build a predictive model in study population with a moderate goodness of fit as assessed by the Hosmer–Lemeshow test (p = .4539). Sensitivity, specificity, PPV, and NPV were calculated (Table 2) and an ROC curve was used to plot the sensitivity versus 1-specificity to examine the different seroconversion indices, the area under the ROC curve was 0.777 (95% confidence interval, 0.69–0.84) (Fig. 2).
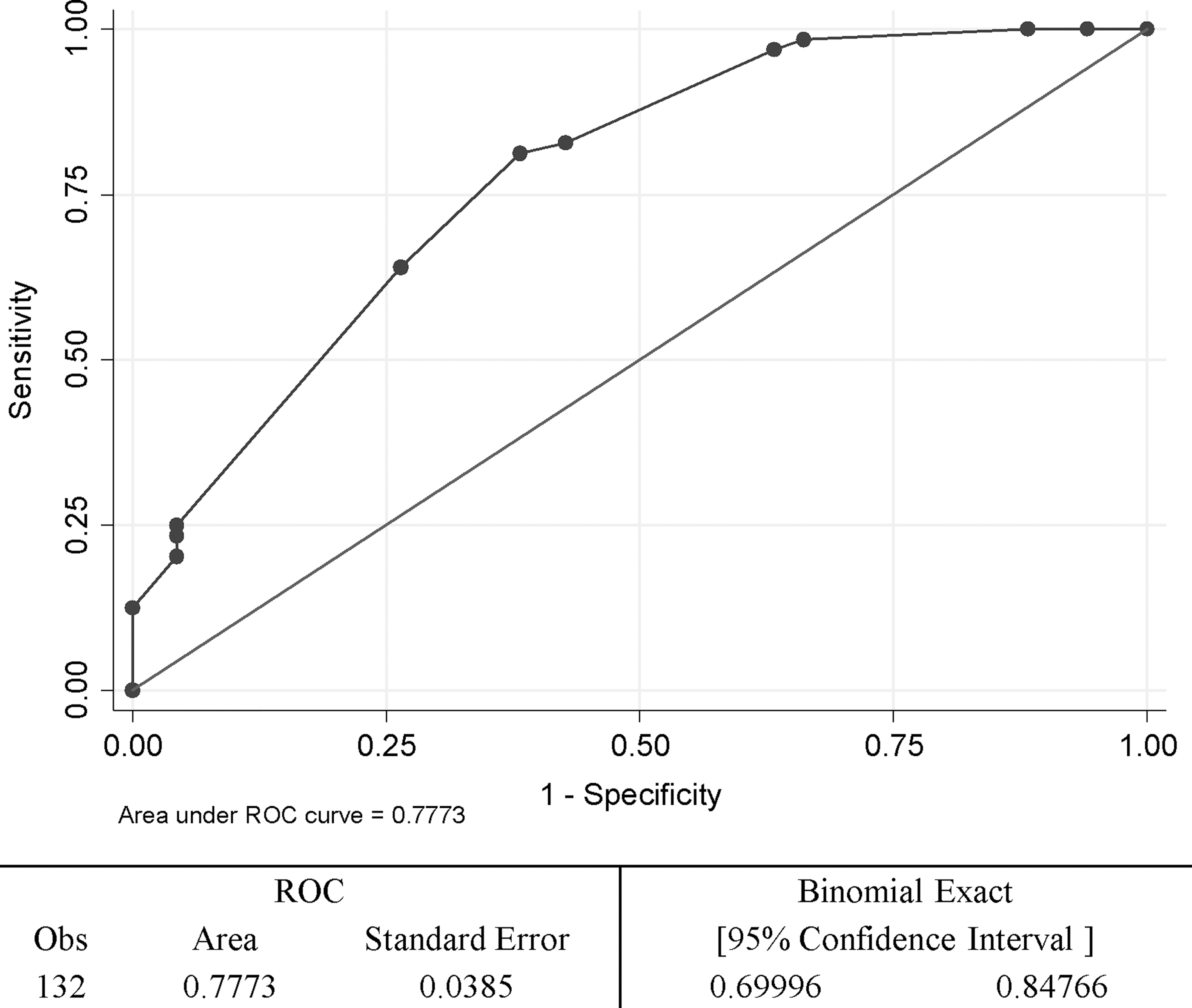
Area under ROC curve indicates the probability that an individual with the outcome had a higher predicted probability than an individual without the outcome for random pairs of individuals with and without the outcome. ROC, receiver operating characteristic.
Discussion
The objective of this study was to analyze factors associated with HIV seroconversion between individuals attending an HIV prevention clinic after at least 3 months of contact risk follow-up comparing cases with individually matched control individuals from the same cohort to develop a model capable of predicting probability of HIV seroconversion in this population. We found that being MSM, having a known HIV-positive partner, having previous PEP, and having previous STI were predictive factors associated with an HIV seroconversion in this population. In addition, we were able to build a predictive model with a moderate goodness of fit, all with the final aim to improve the detection of high-risk population to improve preventive strategies and PrEP implementation.
Seroconversions during contact risk follow-up have been described, reporting an incidence between 0.2% and 8.9%. 5,13,20 In Amsterdam, a cohort of patients receiving PEP was followed up to assess seroconversions after 6 months of follow-up and it was found that 2% individuals seroconverted. 17 This rate is similar to our findings, although we did not actively follow patients once the recommended follow-up finished after the initial HIV exposure. Seroconversions have also been studied in other types of cohorts, Puro 21 studied seroconversions in 1,324 individuals attending a clinic for counseling and HIV testing (142 had taken PEP) and found that at the end of follow-up, 102 (7 with previous PEP) had seroconverted (7.7%). Poynten et al. 18 studied a cohort of 1,427 MSM in Australia and found 53 seroconverters (3.7%).
To target those individuals with higher risk of seroconversion, we have analyzed factors associated with seroconversion. As previously reported, our logistic regression model confirms that being MSM, having known that a sexual partner was infected with HIV during the risk encounter, taken previous PEP, and had an STI history were risk factors for HIV seroconversion. 17,22,23 Contrary to expectations, we did not find that high risk assessment according to recommendations in Spain (Appendix Table 1), which are similar to other ones, 14 was related with seroconversion; it is possible that this assessment is not an adequate surrogate marker in this population. It is estimated that as many as half of people with HIV who are in a long-term sexual relationship have an HIV-negative partner and that a large proportion of new HIV infections in generalized epidemics occur within these serodiscordant relationships. 24 Considering all these findings, it seems that reinforcing legally approved and sanctioned prevention strategies in this high-risk population, as prescribing PrEP, are necessary.
Our study has limitations. We only assessed seroconversions followed in our center; therefore, it is possible that we have underestimated the true rate of seroconversions. We have selected cases assessing only our HIV cohort, and although it is an important limitation, in Barcelona according to government regulations, it is mandatory that HIV-infected patients should be attended to and following a domicile sectorial approach; therefore, it is most probable that seroconverters after a sexual exposure would be attended in our center if they do not change their home address.
In conclusion, HIV seroconversions are quite common between MSM attending specialized centers with known HIV-infected sexual partners and previous and repeated sexual exposure. We offer a seroconversion index to better predict the risk of seroconversion in this population. This index could be helpful to detect those patients with higher risk and therefore reinforce prevention strategies in this group by closer and longer follow-up and the prescription of PrEP to prevent new HIV infections.
Footnotes
Acknowledgments
Authors would like to thank all the patients contributing to this study. This study was partially supported by grant nos. SAF 2012–3907, FIS PI070291, FIS PI12/00969, and RIS RD12/0017/001.
Authors' Contributions
L.L., B.T., J.M.G., and F.G. contributed to the design of the study. L.L., F.G., and E.L. performed analysis. All authors contributed to the manuscript writing and revised and approved the final manuscript.
Author Disclosure Statement
The authors do not have a commercial or other association that might pose a conflict.
| Source serostatus | Risk assessment | ||
|---|---|---|---|
| HIV positive | Considerable risk (0.8%–3%) | Low risk (0.05%–0.8%) | Minimum risk (0.01%–0.05%) |
| RAI and ejaculation a | RVI and ejaculation a | Oral intercourse without ejaculation a | |
| RAI without ejaculation a | |||
| RVI without ejaculation a | |||
| IAI a | Female oral sex a | ||
| IVI a | |||
| ROI and ejaculation a | |||
| HIV unknown b | RAI and ejaculation a | RVI and ejaculation a | |
| RAI without ejaculation a | |||
| RVI without ejaculation a | |||
| IAI a | |||
| IVI a | |||
| Oral intercourse with or without ejaculation a | |||
| Female oral sex a | |||
Without condom, condom breakage, or condom misuse.
Added risk factors: in case of sexual assault or if any of the following risk factors are present, a reevaluation of the overall risk will be necessary and it will be considered as a higher grade:
(1) Viral load of source individual is ≥5,000 copies/ml or the presence of any sign of acute infection or advanced infection or AIDS.
(2) Active sexually transmitted infection either in source individual or individual exposed.
(3) Bleeding during intercourse.
If source individual belongs to a population group where HIV prevalence is ≥15%.
HIV, human immunodeficiency virus; IAI, insertive anal intercourse; IVI, insertive vaginal intercourse; RAI, receptive anal intercourse; ROI, receptive oral intercourse; RVI, receptive vaginal intercourse.