
Abstract
Lack of HIV-1 viral load monitoring in resource-limited settings leads to the development of HIV drug resistance mutations, although WHO recommends viral load testing for monitoring as this helps in preserving future treatment options and also avoid unnecessary switching to more expensive drugs. A total of 101 patients attaining first-line treatment failure (FTF) were followed until second-line treatment failure (STF) to study the rate of accumulation of thymidine analogue mutations (TAMs), their future drug options, and genetic evolution. The result shows that predominant nucleos(t)ide reverse transcriptase inhibitor (NRTI) mutations were M184V/I (87.3% in FTF and 79% in STF) followed by TAMs (53.4% in FTF and 54.5% in STF). The rate of accumulation of TAMs was higher for a patient with TAMI [0.015 TAM per person-month (TPPM)], TAMII (0.042 TPPM), and 1 (0.005 TPPM) or 2 TAMs (0.008 TPPM) compared with a patient with both TAMs and 3 or >3 TAMs. Future ART options show that >50% of the patients can be considered for choices to recycle NRTIs in the second-line, and third-line therapy. We conclude that the patients who initiated thymidine analogue-based first-line before 2010 can be very well opted for AZT- and TDF-based second-line regimen in the future.
T
Since 2010, the NRTI backbone tenofovir (TDF) and zidovudine (AZT) have been used for either first-line or second-line HAART; however, in 2013 a WHO guideline recommends TDF as the preferable choice in first-line and AZT in second-line therapy. Before 2010, AZT was used in the first-line and still many patients who initiated ART before 2010 still continue on AZT.
On comparing discriminatory mutations, excision mutation - i.e., thymidine analogue mutations (TAMs) confers resistance to both AZT and TDF. 3 Although many studies have reported the pattern of TAMs, only very few studies have reported the course of TAMs accumulation, which is especially needed in case of AZT-based first-line treatment that will affect future drug options.
We studied the course of accumulation of TAMs in patients who initiated AZT-based first-line therapy and followed them up to see its impact over future drug options and eventually to identify which second-line regimen can be prescribed.
Retrospectively, 101 HIV-1-infected patients on non-nucleoside reverse transcriptase inhibitors (NNRTI)-based first-line regimen attaining immunological failure and their details during second-line failure were included in the analysis. Prevalence of reverse transcriptase (RT) mutations, TAMs accumulation rate, and future drug options were evaluated among the patients.
HIV-1 pol gene spanning 20–240 codons of RT region was genotyped by validated homebrew method as previously described 4 and mutation pattern was examined, and sequence having admixture of wild-type and mutant residues at single position was considered as mutation. Sequences were aligned (Clustal X) to an Indian subtype C reference (C.IN.AF067155) and examined for HIV-1 subtype using REGA V3 and drug resistance-associated mutations (IAS-USA 2014 and Stanford University HIV drug resistance database v7.0). 5 Majority were infected with subtype C 97% (n = 98), whereas few were infected with subtype B 1.9% (n = 2), followed by CRF01_AE 0.9% (n = 1). Phylogenetic analysis, genetic distance, dN – dS, and quality control were performed with molecular evolutionary genetics analysis (MEGA) software version 6. Distance between group mean and pairwise distance was computed using nucleotide substitution type, maximum composite likelihood model using 1,000 bootstrap replicates; for pairwise distance, genetic distance between Indian subtype C consensus and first-line treatment failure (FTF) and second-line treatment failure (STF) was performed. Codon-based Z-test of selection with Nei-Gojobori method using 1,000 bootstrap replicates was used for computing dN – dS. To find statistical significance, Fisher's exact test and Mann–Whitney U test were performed for categorical and continuous variables, respectively.
Out of 101 patients analyzed, majority (n = 77, 76.2%) were male with median baseline CD4 count of 213 (interquartile range [IQR] 97–314), CD4 T cell count during FTF was 143 cells/μl (IQR 67–274), and STF was 150 cells/μl (IQR 53–286). Majority were on thymidine analogue (TA)-based regimen (n = 86, 85.1%) during FTF and TDF-based regimen (n = 77, 76.2%) during STF (Table 1). During FTF any DRM was observed in 95 (94.1%) individuals, and dual class (NRTI + NNRTI) resistance mutation was observed in 76 (75.2%) individuals, whereas in STF it was 94 (93.1%) and 63 (62.4%), respectively, and protease inhibitor (PI) and triple class (NRTI + NNRTI + PI)-resistant mutation was seen in 45 (44.6%) and 33 (32.7%) individuals, respectively.
HAART, highly active antiretroviral therapy; IQR, interquartile range; NRTI, nucleos(t)ide reverse transcriptase inhibitor; NNRTI, non-nucleoside reverse transcriptase inhibitors.
Major discriminatory mutation observed during FTF and STF was M184V/I, n = 83 (87.3%) and n = 74 (78.7%) followed by K65R, which was seen in n = 4 (3.9%) and n = 6 (5.9%), respectively; TAMs were observed in 54 (53.4%) subjects during FTF and 55 (54.5%) subjects during STF, with major TAMs observed being M41L [FTF, 38 (40%); STF, 40 (42.5%)] followed by T215Y [FTF, 28 (29.4%); STF, 30 (31.9%)]. Although the proportion of TAMs among patients treated with nonthymidine analogue-based regimen is between 8.7% and 27.5%, 6 –8 the high proportion of TAMs in STF is due to the previous exposure to TA drugs, whereas the proportion of TAMs during FTF is in line with the previous finding (47%–63%) 9,10 among patients failing TA-based regimen. Comparison of NNRTI mutation pattern between FTF and STF showed statistically insignificant variation in the proportion of resistance mutations, K103N/S (32.6% vs. 36.1%), Y181C/I/V (27.3% vs. 22.3%), and G190A (31.5% vs. 28.7%), respectively (Fig. 1). Out of 54 with TAMs in FTF, 47 switched to TDF-based second-line; on following them during STF 37/47 retained TAMs and out of 15 who initiated TDF-based first-line, nine had TAMs, while during their STF, seven had TAMs, and out of six without TAMs in first-line, only two acquired TAMs in second-line.
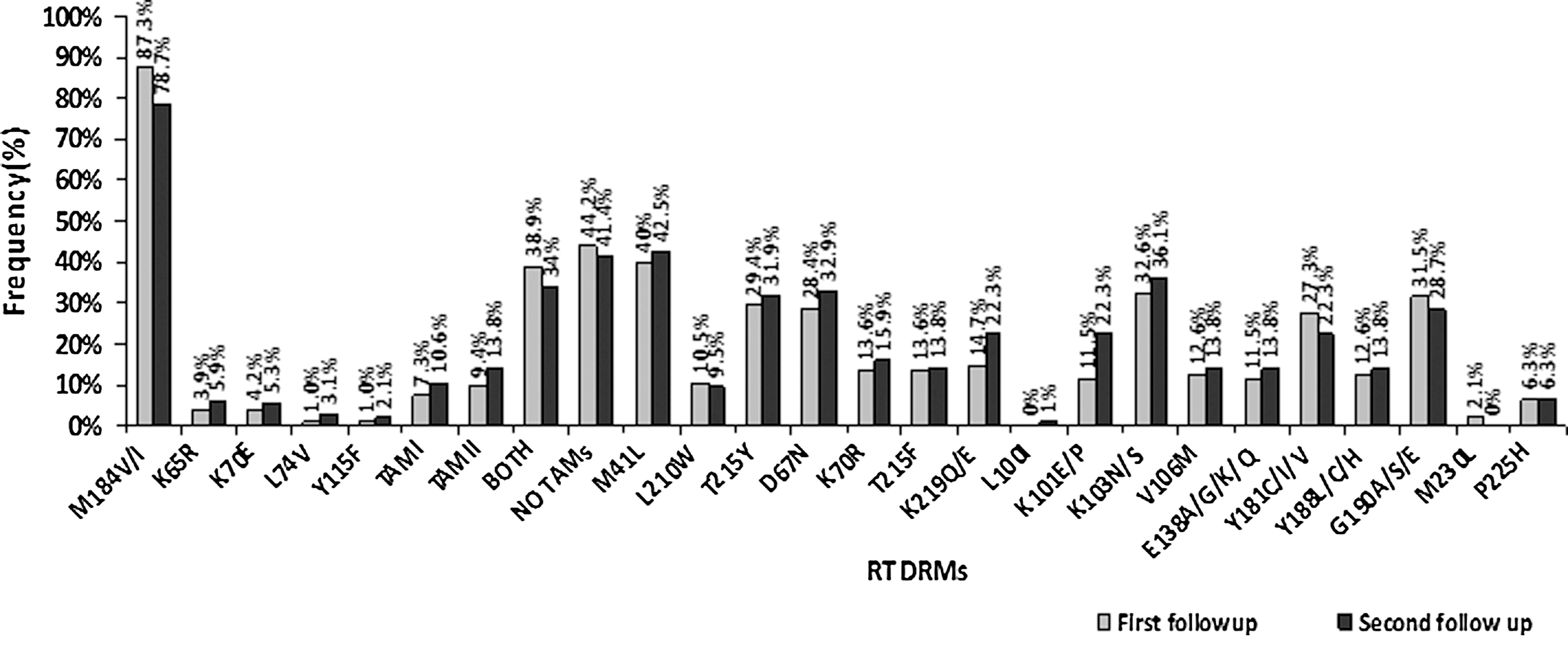
Prevalence of RT DRMs among patients with first and second follow-up. DRM, drug resistance mutation; RT, reverse transcriptase.
Analysis of the patients with and without TAMs during FTF showed that patients without TAMs (n = 47) had very less number of mutations compared with patients with TAMs, predominant mutation being M184IV (n = 31, 66%), followed by K65R (n = 4, 8.5%). On following them, seven with NRTI mutation had no mutation during STF, 12 retained the same mutation during STF, and 11 acquired TAMs during STF. On analyzing PI mutations, we found that a patient without TAMs (n = 14) had less PI mutations, and predominant mutations observed were, V82A (25.5%), M46I/L (12.8%), L10I/F/V (10.6%), and A71I/T/V (6.4%) compared with patients with TAMs (n = 36) (p < .05), mutations, such as M46I/L and V82A (38.8%), L10I/F/V (20.3%) and A71I/T/V (14.8%), were frequently seen among them. The impact of mutation shows that ATV/r and LPV/r are less affected among patients without TAMs compared with patients with TAMs (14.9% vs. 48.1%) and (14.9% vs. 50.7%) (p < .05); this is because high level of NRTI mutations in a patient with TAMs would have reduced NRTI efficacy and thus PI should be acting as mono drug, which would have led to the high selection pressure on PR gene. This phenomenon is also evident from our result showing more genetic distance in PR gene of patients with TAMs (median 0.049, IQR 0.029–0.069) compared with patients without TAMs (median 0.027, IQR 0.02–0.054), p .0014. Although the level of mutation was low among patients without TAMs, time taken for failure was early for them (median 21.7 months, IQR 12.5–29.1) compared with a patient with TAMs (median 36.7 months, IQR 16–52.6) (p < .05). Among patients without TAMs low number of mutations during FTF and STF and less time taken for failure shows that this patient could have poor adherence for ART, which has led to the emergence of less mutation and early failure.
On analyzing TAM accumulation, during FTF, TAMI mutation (n = 20) was observed in 12 (11.9%), TAMII (n = 18) in 11 (10.9%), and both TAMs (TAMI + TAMII) (n = 112) in 31 (31.7%) individuals, with mean TAM of 1.66, 1.63, and 3.61, respectively. On following the respective group for 321.8, 304.2, and 1200.6 person-months, that is, until STF, we observed that 5 and 13 TAMs were accumulated among patients with TAMI and TAMII with the accumulation rate of 0.015 and 0.042 TPPM, however, 36 TAMs in patients with both TAMs dissipated with the TAM dissipation rate of 0.03 TPPM.
On analyzing patients based on the number of TAMs, we found that n = 12 had 1 TAM, 13 had 2 TAMs, 10 had 3 TAMs, and 19 had >3 TAMs (n = 82); on following them until they failed the second-line regimen, that is, 342.83, 610, 369.56, and 700.2 person-months, we observed 2, and 5 TAMs were accumulated for patient with 1 TAM and 2 TAMs in their first visit, with TAMs accumulation rate of 0.0058 and 0.008 TPPM, respectively. For patient with 3 and >3 TAMs, 9 and 4 TAMs dissipated with the dissipation rate of 0.024 and 0.0057 TPPM, respectively.
On comparing TAMI mutation, TAMII confers reduced negative virologic outcome, 11,12 similarly 1 or 2 TAM has reduced negative virologic outcome compared with 3 or >3, 13 and this phenomenon mirrors that the patient with fewer TAMs at baseline genotypic resistance testing had a greater risk of developing additional TAMs. On the other hand, patients with more TAMs are less likely to mediate the emergence of additional TAMs due to the cost of replicative fitness of the virus. 14
Based on the mutation pattern observed in both follow-up, we analyzed the impact of DRMs on future therapy and found that in FTF, high level of resistance was observed to all drugs, and mutation pattern demonstrates following hierarchy of contribution to future ART options: TDF (64.4%) > AZT (53.5%) > ABC (44.6%). In a similar fashion, when the same patients were followed up until STF, their future ART options were: TDF (57.4%) > AZT (50.5%) and > ABC (42.6%) (Fig. 2). Although patients were initiated with TA-based first-line therapy, accumulation of DRMs especially TAMs was apparent, and cross resistance to other NRTIs were also seen; nonetheless, >50% of the subjects can be considered for choices to recycle NRTIs in third-line and salvage therapy. Based on the analysis of second generation NNRTI, still 69% and 52% patients can be considered in future for ETR and RPV-based therapy, respectively.
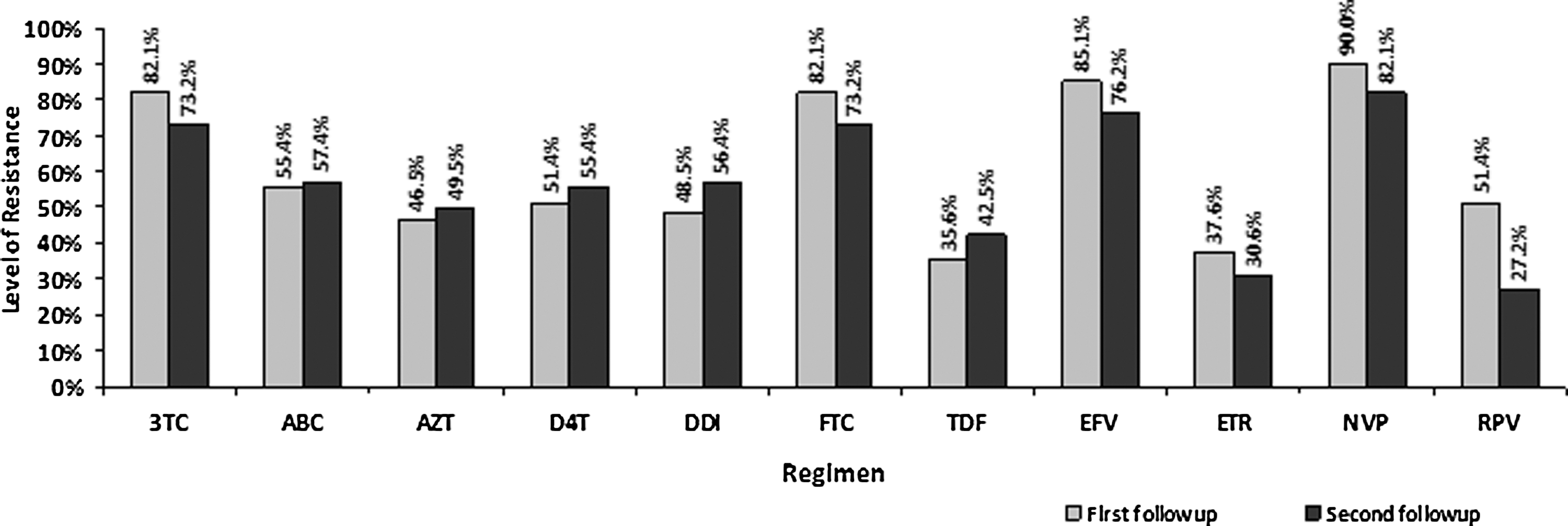
Level of resistance to various drug regimens conferred by DRMs.
We calculated the level of evolution between FTF and STF by estimating genetic distance and dN – dS. Genetic distance between Indian naive consensus and FTF, STF showed mean value of 0.767 and 0.766, respectively (p .8708); on estimating dN – dS between first and second follow-up, we found 49 (48.5%) had purifying selection (dN – dS <1) and 26 (25.7%) each had adaptive selection (dN – dS >1) and neutral selection (dN – dS = 0). This result shows low rate of genetic divergence and evolution, which is in line with the previous evidence stating very low rate (1%) of viral divergence even after 9-year follow-up. 15
In conclusion, the low proportion of adaptive evolution, no significant difference in genetic distance between FTF and STF, and low rate of TAM accumulation shows very low rate of viral emergence. Although the proportion of HIV DRMs differs between FTF and STF, patients failing TA-based first-line regimen when opted for TDF-based second-line therapy, there was no big impact on future drug options. In addition, in this study treatment outcome was monitored immunologically, when virological-based treatment monitoring comes into practice in resource-limited settings, further emergence of DRMs can be avoided by early switching. Thus, patients who initiated TA-based first-line before 2010 can be very well opted for AZT and TDF-based second-line regimen in the future.
Footnotes
Acknowledgments
The authors sincerely thank study participants, YRG CARE laboratory, and clinical staff for their support. They also thank DST-INSPIRE, New Delhi for providing financial assistance to one of their authors (T.R.D.). This work was supported by a grant-in-aid from the YRG CARE Medical, Educational, and Research foundation, Chennai, India. This work received ethical approval from the Institutional Review Board of YRG CARE, Chennai, India.
Sequence Data
Sequences have been uploaded in GenBank under accession number KX583027 - KX583228.
Author Disclosure Statement
No competing financial interests exist.