
Abstract
Successful engagement in HIV care is required to reach UNAIDS targets of 90-90-90. We analyzed routine programmatic data to quantify losses along the HIV care continuum in the country of Georgia. Analysis was limited to diagnosed persons and did not include estimated number of HIV-infected persons. Cascade of HIV care continuum was constructed for adult (age ≥18 years) HIV-infected persons newly diagnosed in Georgia in 2008–2012. Data were extracted from the national AIDS Health Information System as of June 30, 2014. Among 1,931 patients included, the median age was 37 years, 72% were men, and 40.7% had CD4 count <200 cells/mm3. A total of 1,711 (88.6%) were linked to care, 1,333 (69.0%) ever started antiretroviral therapy (ART), 1,044 (54.1%) ever achieved viral suppression, and 792 (41.0%) maintained viral suppression till the end of follow-up. Overall, 1,139 patients were lost from HIV diagnosis to maintaining viral suppression, including 761 (66.8%) patients who remained alive and 378 (33.2%) patients who died. Among 378 deceased patients, 324 (85.7%) died before achieving viral suppression after the median 3.5 months since diagnosis and 54 (14.3%) died after achieving viral suppression after the median 21.2 months since diagnosis. Among 761 alive patients without viral suppression, 297 (39.0%) were fully disengaged, 144 (18.9%) had never been prescribed ART, 161 (21.2) either never achieved suppression or discontinued ART, and 159 (20.9%) experienced rebound while on ART. Efforts are needed to improve earlier HIV diagnosis, to reduce the number of patients not in care, and to extend durability of viral suppression.
Introduction
I
The HIV epidemic in Georgia began in 1989 and since then, and through the end of 2014, a total of 4,695 HIV-infected persons have been reported and 981 deaths were registered among them. The country substantially scaled-up ART since 2004 through the support of the Global Fund to Fight AIDS, Tuberculosis, and Malaria, with 2,541 persons receiving ART by the end of 2014. Previous analysis of the HIV care continuum in the country showed high patient engagement after HIV diagnosis. 7 However, only a minority of them were virally suppressed primarily because of significant gaps in knowledge of HIV serostatus. 7 To better understand contribution of mortality and disengagement from care to continuous retention and viral suppression, we analyzed routinely available program data to quantify losses along the HIV care continuum. Analysis was limited to diagnosed patients only and did not include estimated number of HIV-infected persons.
Materials and Methods
Study design and data source
We conducted a retrospective analysis of routinely available programmatic data that included adult (age ≥18 years) HIV-infected persons newly diagnosed in Georgia in 2008–2012. Data were extracted from the national AIDS Health Information System (AIDS HIS), which is a secure web-based system collecting case-based demographic, clinical, and laboratory data on every reported case of HIV infection. AIDS HIS connects all HIV clinical care providers countrywide and collects all information in real time for each individual from all sites. Quality control mechanisms, including data consistency and missing value checks, as well as verification of entered data against source documents, are performed routinely by the AIDS HIS management team to ensure the accuracy of collected data. Data were extracted as of June 30, 2014. Patients were followed until their last viral load measurement or death, whichever occurred first. Patients not remaining in care by the end of study were followed until their last visit.
HIV care in Georgia
HIV medical care services are provided in five dedicated AIDS treatment centers countrywide. HIV care package in Georgia includes ART, management of opportunistic infections, and comorbidities, including viral hepatitis, tuberculosis, and drug addiction. Until 2011, ART was recommended for patients with a CD4 count <200 cells/mm3, the threshold was moved to <350 cells/mm3 by 2012, and then to <500 cells/mm3 by the end of 2013. The standard of ART monitoring relies on regular monitoring of HIV viral load and CD4 count at least every 6 months. In addition to medical care, support services are also available, including adherence counseling and monitoring. All services are provided free of charge to patients.
Statistical analyses
The following stages of HIV care continuum were quantified: diagnosed, defined as positive HIV test result by any method and confirmed by a positive Western blot or nucleic acid-based test; linked to care, defined as at least one documented clinical visit after HIV diagnosis; being on ART, defined as at least one documented prescription refill within 3 months before date of censoring; and viral suppression, defined as plasma HIV RNA level of <1,000 copies/ml in accordance with WHO recommendations. 8 Viral rebound was defined as plasma HIV RNA level of >1,000 copies/ml after achieving viral suppression. Patient was defined as retained in care if he/she had at least one documented clinical visit after linkage and within 12 months before date of censoring. Patients who did not remain in care were regarded as disengaged from care.
Engagement in care was expressed as percentage of diagnosed HIV patients achieving individual stages of care continuum. We constructed the cascade of HIV care continuum, which included all diagnosed HIV patients, including those who died before end of follow-up (June 30, 2014). This allowed us to elucidate contribution of mortality to losses along the continuum and thus to not achieving viral suppression. For temporal comparisons, two cascades were constructed based on period of HIV diagnosis, categorized as 2008–2010 versus 2011–2012.
Mortality rates were calculated for total cohort and separately for various categories as number of events divided by the number of total person-years of follow-up contributed to study period.
Comparisons were tested using Pearson's chi-square test for categorical variables and Mann–Whitney U test for continuous variables. All analyses were conducted using SAS 9.2.
Results
A total of 1,931 adults newly diagnosed with HIV infection were included in the study. Their median age was 37 years and 72% were men. The main modes of HIV transmission were injection drug use (IDU, 49.5%) and heterosexual contact (43.8%) (Table 1). The majority of patients were diagnosed late as evidenced by a low CD4 cell count at presentation, with 40.7% of patients presenting with advanced immunosuppression (CD4 count <200 cells/mm3) and 20.3% having CD4 count between 200 and 350 cells/mm3. A total of 378 persons died over the median 23.8 (IQR: 7.8–41.0) months of follow-up translating into overall mortality rate of 8.59 (7.76–9.50) deaths per 100 person-years of follow-up. Older persons, men, and IDUs had both lower baseline CD4 cell count and higher rates of mortality (Table 1).
Of 1,931 patients included, 1,711 (88.6%) were linked to care, 1,333 (69.0%) ever started ART, 1,044 (54.1%) ever achieved viral suppression, and 792 (41.0%) maintained viral suppression without experiencing rebound for the median 17.5 (IQR: 8.2–28.3) months (Fig. 1).
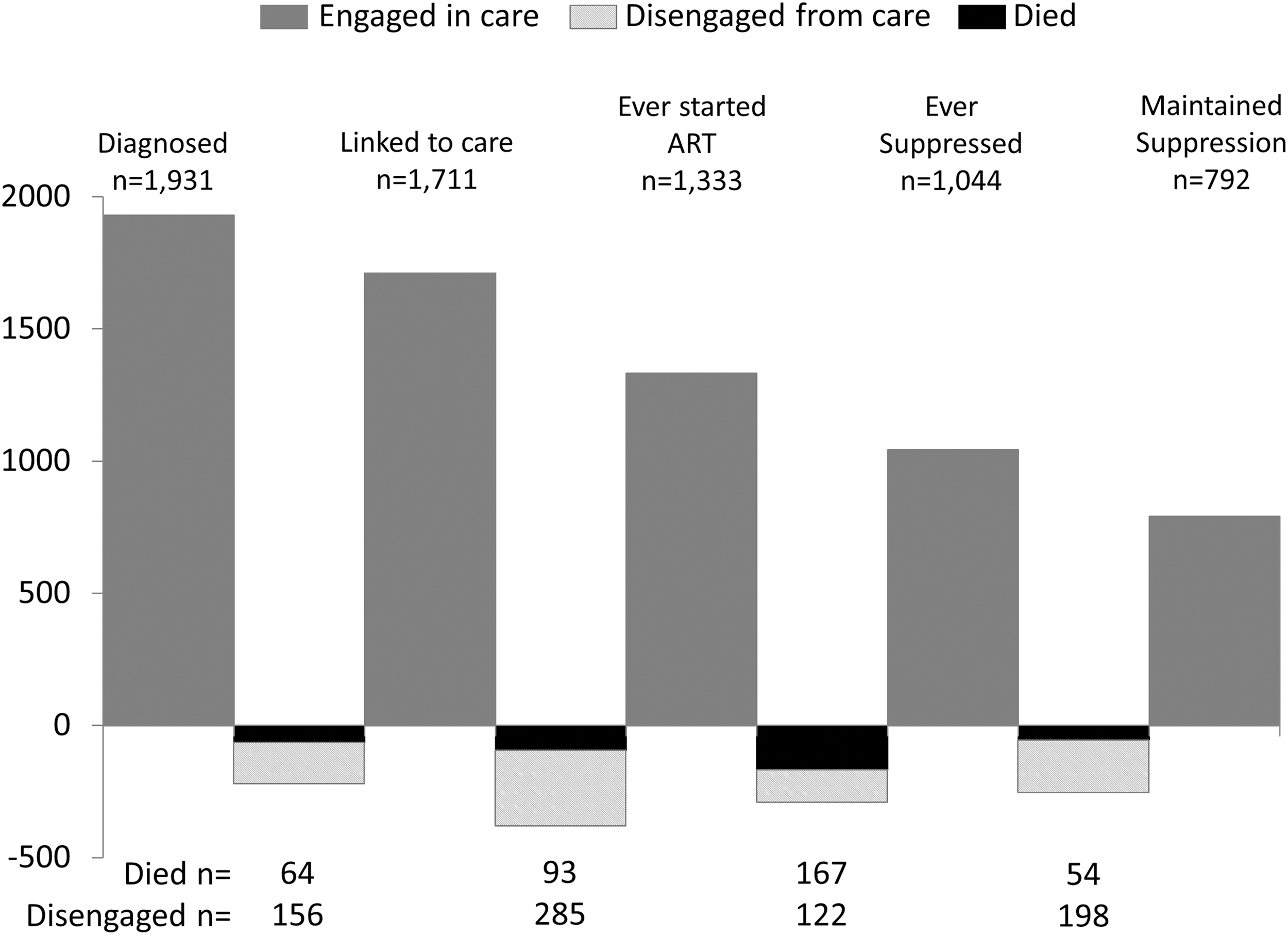
HIV care cascade for the total diagnosed population (n = 1,931).
Overall, 1,139 patients were lost from HIV diagnosis to maintaining durable viral suppression, including 761 (66.8%) patients who remained alive and 378 (33.2%) patients who died (Fig. 1). The majority of deaths (n = 324, 85.7%) occurred before achieving viral suppression after the median 3.5 (IQR: 1.2–11.2) months since HIV diagnosis.
Of 761 patients who were alive and did not maintain viral suppression, 297 (39.0%) were fully disengaged from care before ART initiation, 144 (18.9%) were retained in care, but were not prescribed ART, 320 (42.0%) were lost after starting ART, including 159 patients experiencing viral rebound while remaining on ART. The median time to viral rebound was 10.6 (IQR: 6.3–19.6) months. Of 159 who experienced virologic failure, 110 were able to achieve viral suppression again by the end of follow-up.
Comparison of HIV care continuum by period of diagnosis showed that more patients were lost from HIV diagnosis to maintaining durable viral suppression among those diagnosed in 2008–2010 (64.4%, 690/1072) compared with 2011–2012 (52.3%, 449/859) (p < .0001). Overall, 382 (35.6%) persons in 2008–2010 cohort maintained viral suppression compared with 410 (47.7%) in 2011–2012 cohort (p < .0001) (Fig. 2).
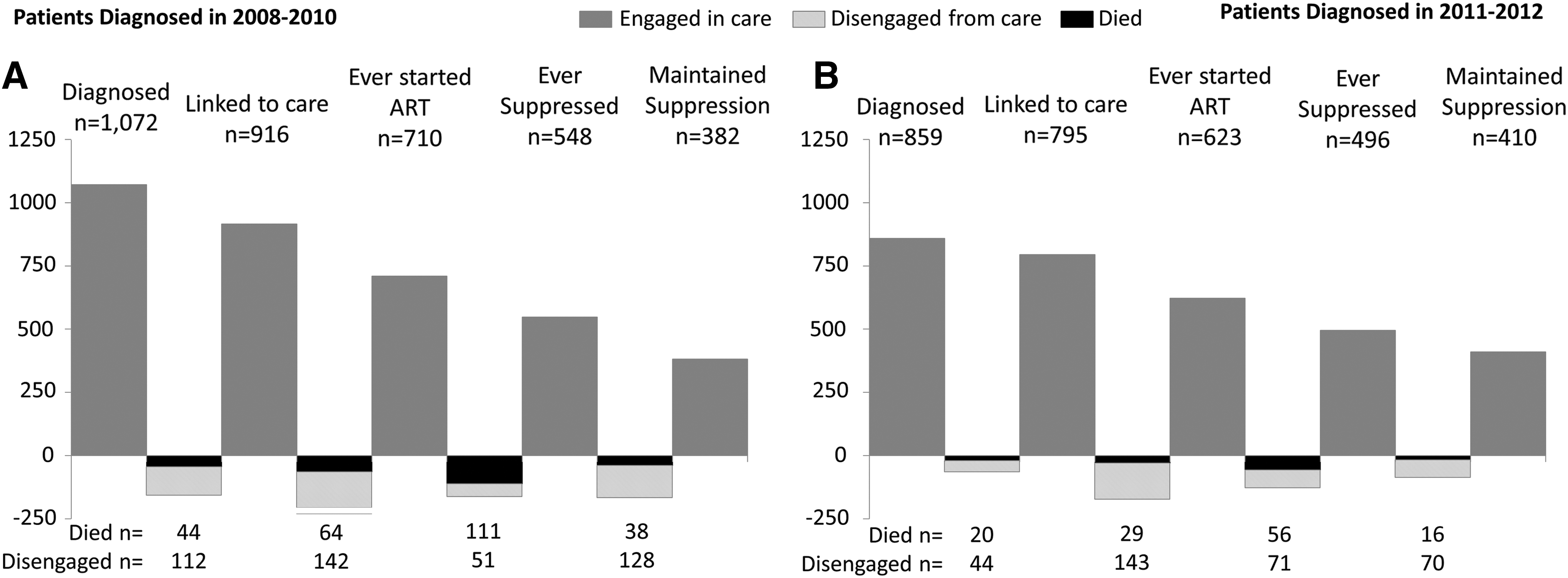
HIV care cascades by period of HIV diagnosis (2008–2010, n = 1,072 vs. 2011–2012, n = 859).
Among 1,553 patients remaining alive at the end of follow-up, 1,397 (90%) were linked to care, 1,011 (65%) were on ART, and 902 (58%) were virally suppressed. Patients without viral suppression had higher CD4 cell count [median 314 (IQR: 154–491) cells/mm3 vs. 216 (IQR: 100–357) cells/mm3, p < .0001]; the highest median CD4 count was among 144 patients remaining in care and not being prescribed ART [median 479 (IQR: 361–625 cells/mm3)], followed by 141 patients disengaged from care between linkage and ART initiation [median 368 (IQR: 258–550 cells/mm3)]. Similar proportion of IDUs and non-IDUs were able to maintain viral suppression (50.9% IDUs vs. 51.0% non-IDUs, p = .97).
Discussion
In this analysis, we used a different approach for constructing HIV care cascade among 1,931 patients newly diagnosed between 2008 and 2012 in Georgia. Important characteristic of our analysis is that we looked at longitudinal maintenance of viral suppression and also elucidated the contribution of mortality to not achieving durable viral suppression.
Overall, 20% of the study population was lost between diagnosis and maintenance of viral suppression due to death. Plotting these deaths as occurring at different stages of HIV care continuum showed that 86% of patients died a median of 3.5 months after diagnosis before being able to achieve viral suppression on ART. The main reason for excess early mortality was late HIV diagnosis. This finding is in line with previous data showing that late diagnosis is the major risk factor for death among people living with HIV (PLHIV) in Georgia. 9,10 In addition to negative effect on survival, late diagnosis has implications on transmission of HIV as people unaware of their status are major contributors of new infections. 11 Despite improvements in HIV testing, recent data suggest that in Georgia, there still is low HIV testing coverage among key populations and particularly among IDUs with only 15% of them reporting having had an HIV test in the prior 12 months. 12 As a result, IDUs had the lowest median CD4 cell count and the highest mortality in our study.
Findings related to viral suppression indicate that patients experienced transitions in their suppression status over time. By the end of follow-up, 902 patients (58% of alive patients) were virally suppressed, but only 792 of them (51% of alive patients) were able to maintain suppression since the first episode through the end of follow-up. Viral rebound has important public health and clinical implications. From the public health standpoint, viremic patients are a potential source of new infection. Clinical implications of rebound include the risk of HIV drug resistance and this is particularly important for Georgia as Efavirenz remains the preferred first-line option following the WHO recommendations.
In our study, being fully disengaged from care (patients never linked to care or not retained in care after initial linkage) was the major reason for not having viral suppression, accounting for 39% of that segment. This is particularly worrisome in light of recent data indicating that persons not retained in care are major sources of new HIV infections. 13
In some cases, disengagement from care can be attributed to the fact that the analysis covered the period when ART was initiated at relatively advanced stages of disease. For example, 144 patients remained in care, but never started ART because of eligibility criteria. Another group of 141 patients with high CD4 cell count were lost before becoming eligible for ART and the majority of them were diagnosed in 2008–2010 when ART was recommended at CD4 count <200 cells/mm3. This is in line with our previous finding showing higher attrition of patients with CD4 count >350 cells/mm3. 7 Studies from sub-Saharan Africa also indicate that higher baseline CD4 cell count is an independent risk factor for lost to follow-up in pre-ART care. 14,15 Since 2011, Georgia increased CD4 threshold for treatment initiation to 350, which might have contributed to better engagement among those diagnosed in 2011–2012. Following the landmark START trial and updated WHO recommendations, Georgia recently adopted a treat all policy, which is expected to have a positive impact on the cascade. 16,17
With regard to achievement of 90-90-90 targets, given that our analysis included only a subset of PLHIV diagnosed between 2008 and 2012, we were not able to assess the first target on diagnosis. The second target on ART coverage needs to be substantially improved as only 65% of diagnosed PLHIV were on treatment. Better retention in care and earlier ART initiation will be the key factors toward reaching the target. Our data show that the target of viral suppression was nearly achieved with 89.2% of those on treatment being virally suppressed by the end of follow-up. However, as described above, efforts are needed to sustain virologic suppression over the long periods of time.
Our study has strengths and limitations. The use of national AIDS HIS that collects information on every reported case of HIV infection from all dedicated AIDS centers throughout the country provides advantage in terms of capturing situation on national level. The major limitation of our study is its retrospective design that used basic programmatic data. Additional information on comorbidities, treatment regimens, and adherence could have been helpful for better explaining observed outcomes. Our cascade of HIV continuum of care does not include the estimated number of PLHIV because our analysis focused only on a subset of patients diagnosed within a specific time period. We calculated the percentage of virally suppressed persons out of diagnosed persons, and this should not be directly compared with studies that included estimated number of PLHIV. Despite several limitations, our analysis demonstrates that routinely available data can provide important information on delivery of HIV care services with no additional resources.
In summary, the Georgian model of service delivery ensures that majority of diagnosed HIV patients are engaged in HIV care; however, improvements are needed at every stage of care continuum to achieve 90-90-90 targets. Efforts are needed to improve earlier HIV diagnosis, to reduce the number of patients not in care, and to extend durability of viral suppression.
Footnotes
Acknowledgment
This work was supported, in part, by the Emory AIDS International Training and Research Program, grant no. D43 TW01042.
Author Disclosure Statement
No competing financial interests exist.