
Abstract
Preventable cardiovascular disease (CVD) risk factors are responsible for the majority of CVD-related deaths, and are increasingly recognized as a cause of morbidity and mortality for HIV-infected persons taking antiretroviral therapy (ART). Simplified tools such as the American Heart Association's ideal cardiovascular health (iCVH) construct may identify and prognosticate CVD risk in resource-limited settings. No studies have evaluated iCVH metrics in sub-Saharan Africa or among HIV-infected adults. Thus, the central aim of this study was to compare levels of iCVH metrics and their correlations with carotid atherosclerosis for HIV-infected adults versus uninfected controls in a well-phenotyped Ugandan cohort. We analyzed the prevalence of iCVH metrics in a mixed cohort of HIV-infected persons on stable ART and uninfected, population-based comparators in Mbarara, Uganda. We also assessed the validity of iCVH by correlating iCVH values with common carotid intima media thickness (CCIMT). HIV-infected persons had a mean of 4.9 (SD 1.1) iCVH metrics at ideal levels versus 4.3 (SD 1.2) for uninfected controls (p = .002). This difference was largely driven by differences in blood pressure, blood glucose, and diet. In multivariable-adjusted linear regression models, each additional iCVH metric at an ideal level was associated with a significant 0.024 mm decrease in CCIMT (p < .001).HIV-infected persons on ART in rural Uganda had more iCVH metrics at ideal levels than uninfected persons. The difference appeared driven by factors that are putatively influenced by access to routine medical care. Composite scores of iCVH metrics were associated with subclinical atherosclerosis and more predictive of atherosclerosis for uninfected persons.
Introduction
C
As longevity for HIV-infected persons has improved substantially in recent decades due to effective antiretroviral therapy (ART), CVD risk factors are increasingly recognized as a major preventable cause of morbidity and mortality for HIV-infected persons. 16 –20 This is particularly true in sub-Saharan Africa, where HIV-infected persons comprise a substantial minority of the population. 21,22 Although morbidity and mortality due to CVD are thought to be increasing in sub-Saharan Africa and among HIV-infected persons, no studies have explicitly evaluated iCVH metrics or correlations of iCVH scores with subclinical CVD in sub-Saharan Africa or HIV-infected populations in any setting. 23 –28 Thus, understanding the patterns and prevalence of health metrics comprising iCVH among HIV-infected and uninfected persons in sub-Saharan Africa may be an essential initial step in crafting policies and ultimately interventions aimed at improving cardiovascular health in sub-Saharan Africa. Moreover, if simple, low-cost metrics like iCVH prove to be predictive of CVD morbidity, they might fill an important clinical need in low-resource settings. The objectives of this study were to (1) assess the distribution of iCVH metrics in a cohort of HIV-infected persons on stable ART in Uganda with uninfected, population-based comparators from the same clinic catchment area and (2) to validate iCVH metrics by testing their association with common carotid intima media thickness (CCIMT), a validated surrogate marker of CVD. 29,30
Materials and Methods
Study site and participants
Data for this study were derived from the Ugandan Noncommunicable Diseases and Aging Cohort (UGANDAC) Study (NCT02445079), an ongoing cohort study of HIV-infected persons in southwestern Uganda and an age and sex-matched, population-based control group of uninfected persons from the surrounding clinic catchment area. 31,32 HIV-infected study participants were selectively sampled from the Uganda AIDS Rural Treatment Outcomes cohort study, which began in 2005 and consists of HIV-infected persons initiating ART, and has been described in detail previously. 33 Eligibility criteria for HIV-infected participants were age >40 years and at least 3 years of ART use. The control sample was drawn from a whole-population cohort study of adults currently being conducted in Nyakabare Parish, a network of eight villages located ∼25 km from the Immune Suppression Syndrome Clinic. This parish was chosen for the study because it has a sociodemographic composition similar to other parishes in the region and because village leaders described relatively little presence by outside nongovernmental organizations. Of 1,851 persons identified in the population census as eligible, 1,814 consented to participate in the baseline survey, for an overall response rate of 98%. Thus, the control sample was drawn from a population that is representative of rural, southwestern Uganda. The local economy is largely characterized by subsistence agriculture, and food insecurity is pervasive. 34 Nearly all (95%) households in the parish report relying on public, rather than private, sources of water for household use; the median household is located 0.25 km from its primary water source. 35
Ideal cardiovascular health measurements
All study participants completed questionnaires to evaluate dietary, physical activity, and smoking history. Participants also underwent anthropomorphic measurement, blood pressure measurement, and blood collection for lipid profile, hemoglobin A1c testing, CD4+ T-cell count, and HIV viral load. Serum chemistry tests were performed using the Abbott Architect Clinical Chemistry Analyzer (Abbott Diagnostics, Abbott Park, IL). Hemoglobin A1c levels were measured using the Bayer A1c Now+ point of care assay (Bayer Pharmaceuticals, Pittsburgh, PA).
Each of the seven iCVH metrics was evaluated and categorized as being at ideal or nonideal levels for each participant using previously published cutoff values. 8 Ideal smoking status consisted of never smoking or having quit >12 months ago; ideal BMI was <25 kg/m2; ideal physical activity consisted of ≥150 min per week of moderate intensity activity, ≥75 min per week of vigorous intensity physical activity, or a combination thereof; ideal total cholesterol was <200 mg/dl; and ideal blood pressure was <120/<80 mmHg. Ideal diet was adapted from the standard definition of dietary score because full data on the volume of dietary intake were not available. We used fruit and vegetable intake as a proxy for diet score (with ≥20 total servings of fruits and vegetables weekly as the cutoff for ideal intake) because previous studies have demonstrated associations between high fruit and vegetable intake and decreased CVD risk. 36,37 We used hemoglobin A1c rather than fasting plasma glucose as the proxy for ideal glucose status because 40 participants were either not fasting when blood glucose was checked or had missing blood glucose data, whereas all participants had complete hemoglobin A1c data. We used a hemoglobin A1c threshold of <5.7% as a proxy of ideal glucose status in light of current conventions that consider this level of HbA1c to be normal. 38 The only iCVH metrics for which any participants had incomplete data were diet (three HIV-infected and six uninfected persons had missing data) and cholesterol (two uninfected persons had missing data). Given the paucity of missing data and resulting limited impact on overall iCVH scores, we designated these 11 missing values as “not ideal” diet or cholesterol.
Common carotid intima media thickness measurement
CCIMT was measured using a standardized protocol 39 by a single trained operator using a Sonosite M-Turbo (Sonosite, Bothell, WA). A total of six images for each participant were obtained from anterior, lateral, and posterior positions in the left and right carotid arteries. These images were then evaluated and scored by a trained, board-certified cardiologist. Far-wall CCIMT was measured in 1 cm segments proximal to the carotid bulb using clinically available, semiautomated border-detection software (SonoCalc, version 5.0; Sonosite). Mean values of all adequate images were summarized as mean CCIMT for each participant. Study personnel were blinded to participant information and HIV serostatus during image quality assurance and CCIMT measurement. For quality assurance, the ultrasound technologist completed paired, prestudy ultrasonography on two separate days for 10 volunteers and found mean CCIMTs of 0.538 mm (t = 0.0012 and p = .999) on both days; the coefficient of variation was 4.9%.
Statistical analyses
We first summarized levels of each of the seven iCVH metrics for HIV-infected versus uninfected participants and compared the distributions between study groups using student t tests. Next we fit linear regression models to compare mean CCIMT for HIV-infected versus uninfected participants. Finally, multivariable-adjusted linear regression was used to estimate the association between iCVH metrics at ideal levels and CCIMT, stratifying by HIV serostatus. To evaluate the potential utility of a simplified iCVH score without laboratory-based metrics (i.e., that could potentially be used in resource-limited settings), we then repeated these analyses excluding cholesterol and blood glucose (and thus the iCVH score includes only smoking, BMI, blood pressure, physical activity, and dietary intake).
Results
Participant characteristics and prevalence of ideal cardiovascular health metrics
Mean age of HIV-infected and uninfected study participants was 49.3 and 51.8, respectively, and both groups had approximately half female participants (Table 1 and Fig. 1). Only 2.9% of HIV-infected persons and 2.0% of uninfected controls had iCVH, defined as all seven iCVH metrics being at ideal levels. HIV-infected persons had a mean of 4.9 (±1.1) iCVH metrics at ideal levels versus 4.3 (±1.2) for uninfected controls (p = .002). This difference appeared to be driven primarily by substantial differences in ideal blood pressure (66.7% for HIV-infected participants versus 36.0% for uninfected controls), blood sugar (72.4% versus 58.0%), and diet (18.6% versus 7.4%).
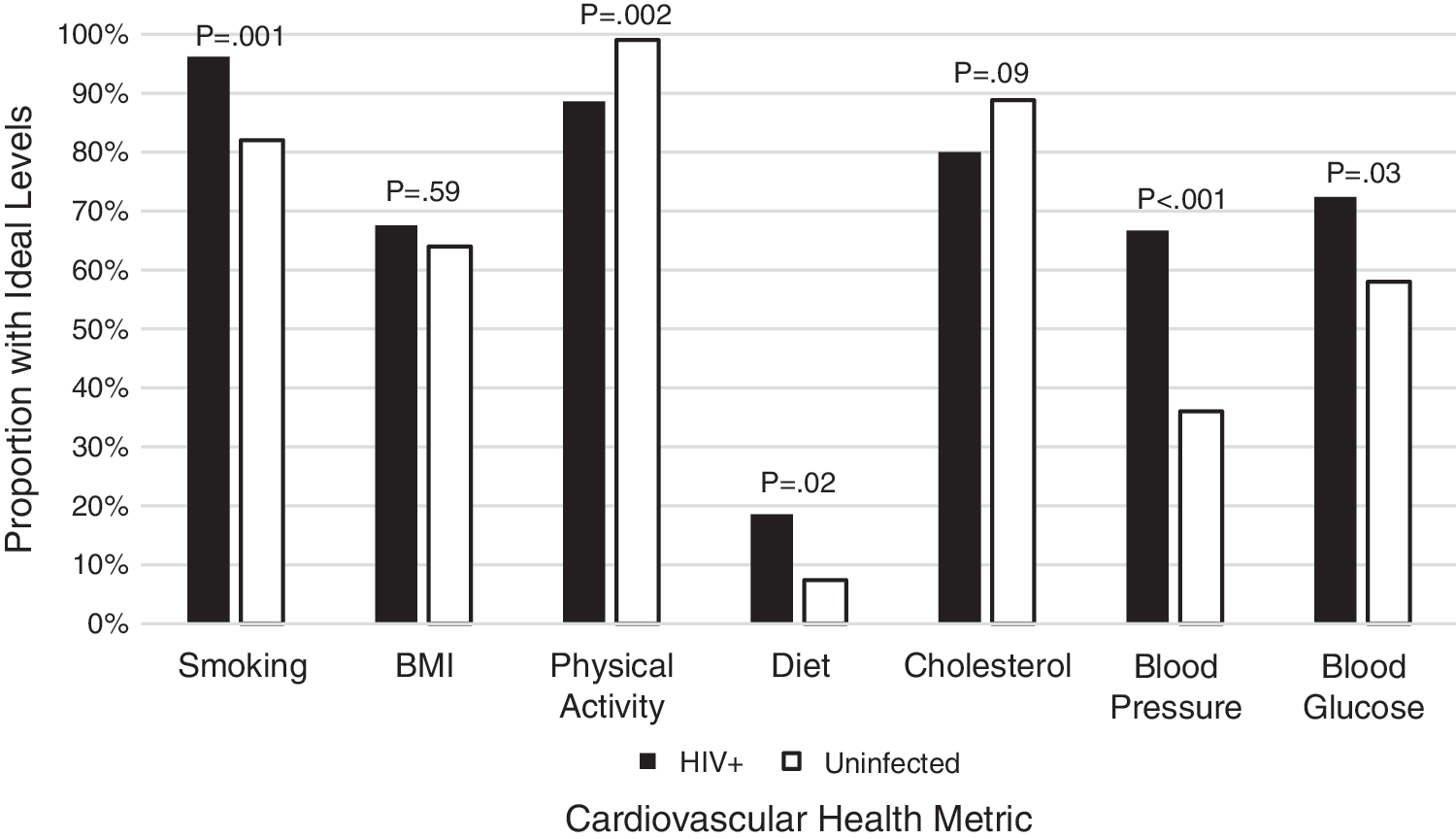
Proportion of HIV-infected and uninfected participants with ideal levels of CVH metrics. CVH, cardiovascular health.
BMI, body mass index; IQR, interquartile range; SD, standard deviation.
Ideal cardiovascular health metrics and common carotid intima media thickness
When we evaluated associations between iCVH metrics and CCIMT, a higher number of iCVH metrics at ideal levels were consistently associated with significantly lower CCIMT (Table 2). In univariate linear regression models, each additional iCVH metric at an ideal level was associated with a −0.027 mm difference in CCIMT (95% CI −0.039, −0.015; p < .001) and HIV serostatus was associated with a −0.038 mm difference in CCIMT (95% CI −0.068, −0.010; p = .009). When iCVH metrics and HIV serostatus were included in a multivariable linear regression model with CCIMT as the outcome, each additional iCVH metric at an ideal level was associated with a −0.024 mm difference in CCIMT (95% CI −0.036, −0.012; p < .001). Thus, for instance, persons with two iCVH metrics at ideal levels had predicted CCIMT of 0.751 mm, compared with a predicted CCIMT of 0.654 mm for persons with six iCVH metrics at an ideal level. Compared with the sample standard deviation of 0.106, this comparison between persons on the lower versus higher end (but not quite the extremes) of the iCVH spectrum represented an effect size of (0.751–0.654)/(0.106) = 0.915 standard deviation units, which represents a large effect size. Notably, in these multivariable models, the association between HIV serostatus and CCIMT was no longer significant (95% CI −0.054, 0.003; p = .08), nor was the interaction term for CCIMT and HIV serostatus (p = .38). The overall correlation (Pearson's r) between iCVH metrics and CCIMT was 0.29 (Fig. 2A) and the correlation was marginally weaker for HIV-infected (r = 0.19; Fig. 2B) than for uninfected (r = 0.32; Fig. 2C) participants.

CVH, cardiovascular health; IMT, intima media thickness.
Associations between iCVH metrics and CCIMT remained significant when we excluded laboratory-based iCVH metrics (cholesterol and glucose) and included only smoking, BMI, physical activity, diet, and blood pressure (Table 3 and Fig. 2D). In univariate linear regression models, each additional iCVH metric at an ideal level was associated with a −0.023 difference in CCIMT (95% CI −0.039, −0.006; p = .007). When we added HIV serostatus to a multivariable linear regression model, this association remained statistically significant (coefficient −0.018; 95% CI −0.035, −0.001; p = .04) and the interaction term was not significant (p = .50). In this model, persons with one nonlaboratory iCVH metric at an ideal level had a predicted CCIMT of 0.728 mm compared with a predicted CCIMT of 0.657 mm for persons with five nonlaboratory iCVH metrics at ideal levels, resulting in a moderate effect size of 0.67 standard deviation units. The correlation between nonlaboratory iCVH metrics and CCIMT was marginally weaker (r = 0.19) than that between all seven iCVH metrics and CCIMT (r = 0.29).
Discussion
In this analysis of a well-phenotyped cohort of HIV-infected participants on ART and uninfected controls in rural Uganda, we found that HIV-infected participants have more iCVH metrics at ideal levels. In addition, participants with higher number of iCVH metrics at ideal levels had significantly lower CCIMT. Each additional iCVH metric at an ideal level was associated with 0.024 mm lower CCIMT. Analyses from large observational cohorts have demonstrated that increments in CCIMT ranging from 0.03 to 0.20 mm are associated with 33%–300% higher risk for coronary heart disease and stroke; 29,40 –42 thus, in our study, an additional two to four iCVH metrics at ideal levels (corresponding to 0.048–0.096 mm lower CCIMT) may be associated with a clinically meaningful increment in risk for atherosclerotic clinical events. Longitudinal follow-up will be necessary to better understand the clinical implications of these findings in sub-Saharan Africa. Also of note, the association between iCVH metrics and CCIMT was stronger for uninfected than for HIV-infected participants.
Although the higher number of iCVH metrics at ideal levels for HIV-infected study participants compared with uninfected controls might appear counterintuitive given the association between HIV and CVD, there are several potential explanations for this finding. The iCVH metric with the highest disparity for HIV-infected versus uninfected participants was blood pressure. A total of 66.7% of HIV-infected participants had ideal blood pressure (<120/<80 mmHg) compared with only 36.0% of uninfected controls. This difference was not attributable to disparities in antihypertensive use; more HIV-infected persons (n = 7; 6.7%) than uninfected persons (n = 1; 1%) were taking antihypertensive medications, but this disparity was insufficient to explain the >30% difference between groups in prevalence of ideal blood pressure. Although some studies in sub-Saharan Africa have reported higher blood pressures among HIV-infected persons than uninfected controls, others in sub-Saharan Africa have suggested the inverse. 43 –45 Interestingly, one of these analyses also found that for HIV-infected persons, low blood pressure was associated with a higher mortality risk than high blood pressure. 43 Relatively low blood pressure has been observed among patients with HIV infection—even among those on ART—and is thought to result from concomitant infections, bacterial translocation, autonomic dysfunction, and/or cardiometabolic derangements. 1,20,43,46 Thus, it is possible that HIV-infected participants in our cohort who would otherwise have had higher blood pressures experienced downward influence on blood pressure due to chronic HIV disease. This complicates the interpretation of “ideal” blood pressure (<120/<80) for HIV-infected persons somewhat, as the higher prevalence of ideal blood pressure for HIV-infected participants in this study may simply reflect HIV disease activity.
An alternative, perhaps complementary, explanation for why HIV-infected participants were more likely to have ideal blood pressures is they may be more likely to have access to primary care services than uninfected controls in our sub-Saharan Africa setting. At the Mbarara Regional Referral Hospital Immune Suppression Syndrome Clinic, where participants in this cohort receive care, blood pressure is checked at each visit, and patients routinely see both a nurse and clinical officer. If HIV-infected participants in care in the region are seeing physicians more often than uninfected controls, they are likely to have higher opportunity to access both preventive and therapeutic health services. Although rates of hypertension treatment were low in both groups, 7 of 105 participants in the HIV-infected group versus only 1 of 100 in the uninfected group had an active prescription for an antihypertensive at the time of the study. This possibility is also supported by our finding that HIV-infected participants were more likely to have ideal levels of blood sugar (72.4% versus 58.0% ideal) and smoking (96.2% versus 82.0% ideal). If this is the case and HIV-infected persons have more iCVH metrics at ideal levels because they are more closely linked to care, it underscores both the value of HIV-care programs in the region and the need to translate these services into access to appropriate noncommunicable disease screening and care for uninfected populations in sub-Saharan Africa.
The association we identified between iCVH metrics and CCIMT is the first in sub-Saharan Africa to validate the iCVH scale and is consistent with previous studies in European and North American cohorts of uninfected persons. Prior studies have similarly demonstrated that persons with more iCVH metrics at ideal levels have less subclinical CVD. Although our study did not include overt CVD, others have reported associations. 14,15 The stronger correlation between iCVH metrics and CCIMT for uninfected persons we noted is potentially attributable to the lack of inclusion of HIV-specific risk factors that have been associated with CVD risk, such as CD4 count and ART regimen. 47 The consistent association of iCVH metrics at ideal levels with lower CCIMT in both groups lends support to the use of the iCVH scales as a relatively simple and potentially scalable approach to evaluating CVD risks in sub-Saharan Africa. Moreover, the five-item iCVH score, which excluded laboratory-based parameters (cholesterol and glucose), remained associated with CCIMT and is potentially advantageous due to easier application in resource-limited settings.
This study's findings should be interpreted in the context of its limitations. Given the relatively small size and cross-sectional nature of our study, we were unable to evaluate CVD outcomes and thus relied on CCIMT as a surrogate endpoint. However, CCIMT has been strongly associated with CVD in several populations, and the effect sizes we reported have been clinically predictive of CVD events. 48 –52 Moreover, the richness of phenotypic data in this cohort enabled us to capture all seven iCVH metrics and composite iCVH scores—something that, to our knowledge, has not been done in an HIV-infected nor sub-Saharan Africa cohort. The cohort we analyzed is largely representative of HIV-infected persons in rural Uganda with well-controlled disease on ART and uninfected persons (matched controls) from the same region. Our findings are therefore generalizable to this population, and data from other subpopulations on the continent will be necessary to describe these relationships more broadly.
Another limitation of this study is its cross-sectional nature, which prevented us from evaluating prospective associations of iCVH metrics with incident CVD. Our cross-sectional approach assumes that levels of iCVH metrics tend to be consistent over time and predate carotid atherosclerosis, which we believe to be a reasonable assumption given consistency of CVD risk factors seen in population-based cohorts. 53 Finally, an important consideration about the iCVH metric approach, in general, is the equal weighting given to each factor and the resulting effect on risk prediction. For instance, although being a current smoker likely has a higher detrimental impact on CVD health than having a BMI ≥25 kg/m2, each of these would equally result in having one less point in an iCVH score that simply counts number of iCVH metrics at ideal levels. Although this conflation of risk factors with different effect sizes may limit the predictive utility of these iCVH metrics, our data demonstrate that it has important value as a simplified tool for health status assessment and risk prevention.
Future studies in well-phenotyped cohorts in sub-Saharan Africa are needed to confirm our findings and investigate the extent to which iCVH metrics correlate with overt CVD. If correlations between iCVH scores and CVD are consistently weaker in HIV-infected versus uninfected cohorts in sub-Saharan Africa, it would be reasonable to evaluate whether adding clinical (e.g., duration of HIV infection and ART) and/or laboratory-based (e.g., CD4+ T-cell count) HIV-specific parameters improves the validity of iCVH scores for this population. Ultimately, the use of a relatively simple, scalable approach to capturing CVD risk factors for both HIV-infected and uninfected persons in sub-Saharan Africa and similar settings would serve the important goal of improving cardiovascular health surveillance and prevention globally.
Footnotes
Acknowledgments
The authors wish to thank all study participants and personnel from the UGANDAC study. This work was supported by several grants from the National Institutes of Health (P30 AI027763, R01 MH054907, and R21 HL 124712).
Author Disclosure Statement
No competing financial interests exist.