
Abstract
According to 2013 WHO guidelines, tenofovir (TDF) is the preferred first-line regimen for adults and adolescents. A total of 167 HIV-1-infected patients attaining immunological failure after TDF-based first-line HAART were included in this study, RT region of HIV-1 pol gene was sequenced for them, IAS-USA 2014 list and Stanford HIV drug resistance database were used for mutation interpretation. REGA V3.0 was used for HIV subtyping. The predominant NRTI and NNRTI mutations observed were M184IV (59.9%), K65R (28.1%), and thymidine analogue mutations (TAMs, 29.3%) and K103NS (54.5%), V106AM (39.5%), and Y181CIV (19.8%), respectively. Mutational association shows, K65R was negatively associated with TAMs (OR 0.31, p .008), M184V (OR 0.14, p .57), and K70E (OR 0.29, p .02). Genotypically predicted level of drug resistance based on mutation pattern shows 88% can be opted for azidothymidine (AZT) and still 65% can be opted for TDF. Considering the nature of K65R mutation in increasing susceptibility to AZT and its low prevalence, we conclude that in most patients failing TDF-based first-line therapy, AZT can be considered for second-line therapy followed by TDF itself.
E
A total of 167 HIV-1-infected individuals who were on TDF-based first-line regimen attaining immunological failure (IF) were cross-sectionally enrolled in the study; IF is defined as CD4 count falls to the baseline (or below) or as 50% fall from on-treatment peak value or persistent CD4 levels below 100 cells/mm3. HIV-1 pol gene was genotyped by validated homebrew method 4 spanning 20–240 codons of RT, and mutation pattern was examined, sequences having admixture of wild type and mutant residues at single position were considered as mutation. Sequences were aligned (ClustalX) to an Indian subtype C reference (C.IN.AF067155) and examined for HIV-1 subtype using REGA V3 and drug resistance-associated mutations using IAS-USA 2014 and Stanford HIV drug resistance database. Patients were classified into two groups based on selection of K65R: DRMs containing K65R (group A) and DRMs without K65R (group B) were analyzed to identify potential second-line option. Demographics were recorded as number (%) for categorical variables and median [interquartile range (IQR)] for continuous variables.
HIV-1-infected patients (n = 167) with median age of 36 years (IQR 31–40), baseline CD4 of 175 cells/μL (IQR 69–285), and CD4 T-cell count during IF of 197 cells/μL (IQR 95–310) were selected by excluding patients with prior mono/dual ARV therapy other than TDF and were analyzed for their DRMs (Table 1). All infection (100%) was due to HIV-1 subtype C virus. Duration for treatment failure was 78.7 weeks (IQR 50.5–142.5), although it is low compared with other studies among first-line failures of same geographical region (median 160.71, 219 weeks), 5,6 we speculate that in previous studies, time of detection of IF could have been delayed, which is evident by the emergence of high level of DRMs.
Available only for 68 patients.
TDF, tenofovir.
Of 167 patients, 151 (90.4%) had DRMs, of which any NRTI, NNRTI, and dual mutations (NRTI and NNRTI) were seen in 123 (73.7%), 147 (88%), and 119 patients (71.3%), respectively. Of the 167 patients, the predominant discriminatory mutation observed was M184V, 100 (59.8%) caused high-level drug resistance to 3TC and FTC; however, M184V hypersensitizes and reduces the emergence of resistance to AZT, d4T, and TDF. 7,8 K65R mutation was detected in 47 individuals (28.1%), which was more frequently selected by subtype C than by subtype B virus, causing poor virological response to TDF. 9 Thymidine analogue mutations (TAMs) were observed in 49 patients (29.3%), of which majority, 29 (17.4%), had TAM II, 10 (6%) had TAM I, and 10 (6%) had TAM I and TAM II. Among NNRTI DRMs, Y181C and Y188L were observed in 33 (19.8%) and 20 patients (12%), respectively (Fig. 1); although the proportion is low, co-occurrence of various combinations of K103N, G190A, V106M, P225H, M230L, and K101E/K with Y181C, 32 (97%), and K103N, V106M, and L100I with Y188L, 13 (86.7%), will have adverse impact by generating cross-resistance to second-generation NNRTIs (ETR and RPV). 10 –12
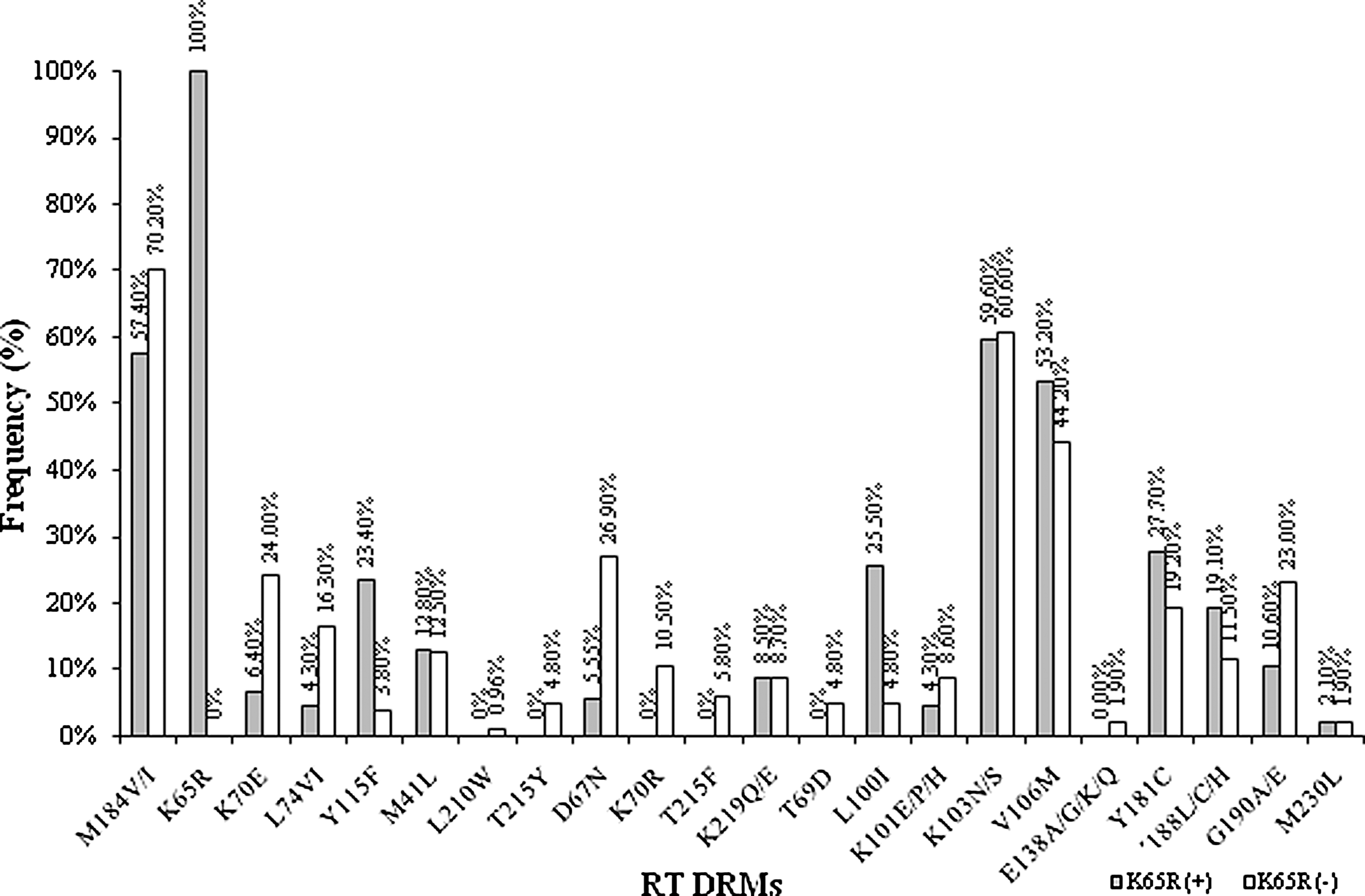
Prevalence of RT DRMs among patients with and without K65R mutation. DRMs, drug resistance mutations.
On analyzing the association between mutations, we found strong negative association between K65R and TAMs (OR 0.31, p .008), in particular K70R and T215F/Y was not observed even in a single patient with K65R mutation (Fig. 1), which is attributed to the in vivo bidirectional phenotypic antagonism and counter selection. Favorably, only the Q151M complex accessory mutation was observed in four individuals (A62V and V75I), which does not cause high level resistance to AZT. 13
Above all, low frequency of M184V (OR 0.14, p 0.57) and K70E (OR 0.29, p .02) was observed in group A than in group B; this seems likely because K65R+M184V reduces the processivity of reverse transcriptase enzyme and the efficiency of tRNA primed ss DNA synthesis, 14 similarly K65R+K70E reduces replication capacity to 2.4 ± 0.9%. 15 Whereas Y115F is more associated with group A (OR 7.6, p .0005). In the same line, of NNRTI mutations, L100I is more associated with group A (OR 6.8, p .0005), although we have found strong association, the mechanism behind this association needs to be resolved.
Based on the mutations seen in group A, we found high level resistance was observed to all drugs, except AZT, as none of the mutations affected AZT susceptibility (Fig. 2). Among group B patients, the mutation patterns demonstrate the following hierarchy of contribution to intermediate to high level resistance to ART: 3TC = FTC (70.2%) >ABC (54.8%) >DDI (51%) >D4T (34.6%) >AZT (19.2%) >TDF (10.6%) (Fig. 2). On combining both groups, although all 167 patients failed on TDF-based regimen, still 109 (65.3%) can be considered for TDF-based NRTI as a second-line option. In a similar way, about 147 patients (88%) can be considered for AZT-based NRTI as a second-line option.
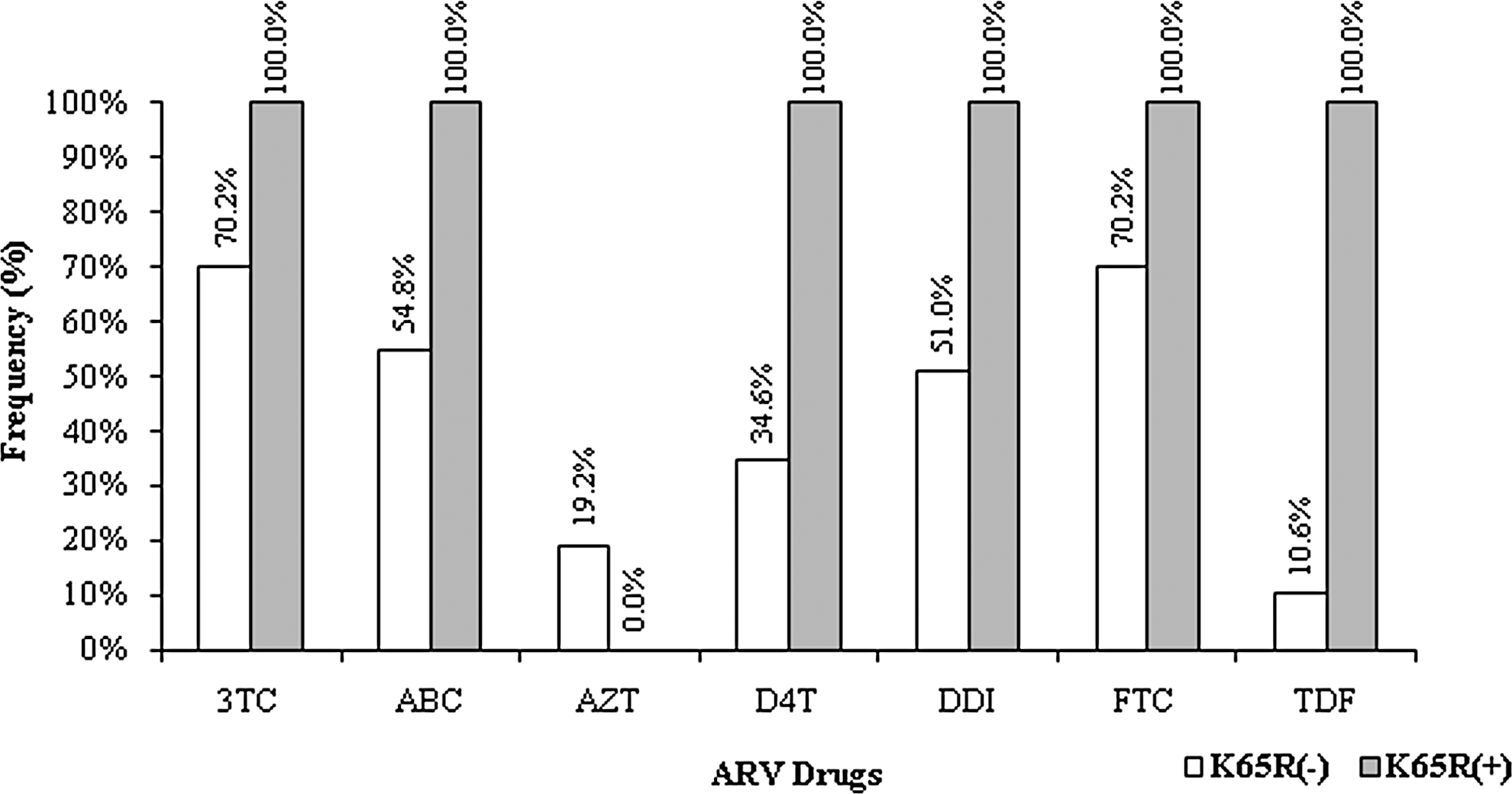
Level of resistance to various drug regimens conferred by DRMs.
DRM pattern demonstrates, the prevalence of K65R mutation was low among patients failing TDF, despite self-reported good adherence. Thus, considering the nature of K65R mutation in increasing susceptibility to AZT and its low prevalence, we conclude that in most patients failing TDF-based first-line therapy, AZT can be considered for second-line ART regimen, followed by TDF itself.
Sequence Data
Sequences were deposited in GenBank under accession numbers KX275045– KX275211
Footnotes
Acknowledgments
We sincerely thank the study participants, YRG CARE laboratory, and clinical staff for their support. We also thank DST-INSPIRE, New Delhi, for providing financial assistance to D.T.R. This work was supported by a grant-in-aid from the YRG CARE Medical, Educational and Research Foundation, Chennai, India. This work received ethical approval from the Institutional Review Board of YRG CARE, Chennai, India.
Disclosure Statement
No competing financial interests exist.