
Abstract
HIV-1 incidence and prevalence remain high among men who have sex with men (MSM), and transgender women (TGW), in Thailand. To examine the link between epidemiologic factors and HIV-1 subtype transmission among Thai MSM, we compared covariates of infection with HIV CRF01_AE and other HIV strains among participants in the Bangkok MSM Cohort Study (BMCS). The BMCS was an observational cohort study of Thai MSM and TGW with up to 60 months of follow-up at 4 monthly intervals. Participants underwent HIV/sexually transmitted infections testing and provided behavioral data at each visit. Infecting viral strain was characterized by gene sequencing and/or multiregion hybridization assay. We correlated behavioral/clinical variables with infecting strain using Cox proportional hazards. Among a total of 1372 HIV seronegative enrolled participants with 4,192 person-years of follow-up, we identified 215 seroconverters between April 2006 and December 2014, with 177 infected with CRF01_AE and 38 with non-CRF01_AE subtype. Age 18–21 years (adjusted hazard ratio [AHR] 2.2, 95% confidence interval [CI]: 1.4–3.5), age 22–29 (AHR 1.6, 95% CI: 1.1–2.3), living alone (AHR 1.5, 95% CI: 1.1–2.1), drug use (AHR 2.2, 95% CI: 1.4–3.5), intermittent condom use (AHR 1.7, 95% CI: 1.3–2.3), any receptive anal intercourse (AHR 1.7, 95% CI: 1.2–2.4), group sex (AHR 1.5, 95% CI: 1.1–2.2), anti-herpes simplex virus type 1 (AHR 1.5, 95% CI: 1.1–2.1), and Treponema pallidum antibody positivity (AHR 2.5, 95% CI: 1.4–4.4) were associated with CRF01_AE infection. Age 18–21 years (AHR 5.1, 95% CI: 1.6–16.5), age 22–29 (AHR 3.6, 95% CI: 1.3–10.4), drug use (AHR 3.1, 95% CI: 1.3–7.5), group sex (AHR 2.4, 95% CI: 1.1–5.0), and hepatitis B virus surface antigen (AHR 3.6, 95% CI: 1.3–10.2) were associated with non-CRF01_AE infection. We observed several significant biological and behavioral correlates of infection with CRF01_AE and other HIV strains among Thai MSM. Divergence in correlates by strain may indicate differences in HIV transmission epidemiology between CRF01_AE and other strains. These differences could reflect founder effects, transmission within networks distinguished by specific risk factors, and possibly biological differences between HIV strains.
Introduction
D
Currently, CRF01_AE is the dominant subtype across all high-risk HIV groups in Thailand, while HIV-1 subtype B cocirculates at lower frequency. Coinfection with these two subtypes has led to the emergence of various CRF01_AE/B recombinant forms. 16 –20 Examining HIV subtype distributions and other molecular markers together with behavioral and sociodemographic risk factors within a focused local epidemic can add a greater understanding to transmission patterns within the MSM population. This information can be used to define viral transmission pathways between overlapping risk groups, outline sexual networks responsible for efficient onward transmission of HIV-1 infection, 21 –23 and may contribute to a deeper understanding of the changing trends in the evolution of the HIV epidemic. The uncontrolled HIV-1 epidemic among MSM highlights a critical need to understand factors driving HIV transmission in this group. To this end, we sought to describe the association between HIV subtypes and risk behaviors among urban Thai MSM seroincident HIV cases enrolled in the Bangkok MSM Cohort Study (BMCS).
Materials and Methods
Study population
The BMCS was an open, longitudinal, observational, cohort study conducted at the Silom Community Clinic, located in central Bangkok. Participants were recruited by advertisement at MSM venues and popular Thai MSM Internet sites, during HIV voluntary counseling and testing services provided at the study clinic, and by word of mouth. BMCS eligibility criteria included Thai nationality, male sex at birth, age 18 years or older, residence in Bangkok, history of oral sex with another man within the 6 months before screening, history of insertive anal intercourse (IAI) or RAI with another man within the 6 months before screening, and commitment to a minimum of 36 months of follow-up at 4-month intervals. All participants provided written informed consent before enrollment. At entry, participants completed an audio computer-assisted self-interview (ACASI) to record behavioral and demographic information and underwent baseline testing for HIV and other sexually transmitted infections (STI). Participants completed follow-up ACASI surveys to track behavior changes at 4 monthly follow-up visits and were retested for STI annually. At each visit, participants received 500 Thai Baht (approximately USD16.60) in compensation for time and transportation expenses.
Laboratory methods
Participants were tested for HIV infection at each visit using the OraQuick® HIV-1/2 Rapid Test performed on oral fluid samples (OraSure Technologies, Inc., USA; Fig. 1). Positive test results were confirmed according to Thai national guidelines with three other HIV rapid tests (Determine™ HIV 1&2, Abbott, Japan; DoubleCheck™ II HIV 1&2 or DoubleCheck Gold™ Ultra HIV1/2, Organics Ltd., Israel; and Capillus™ HIV-1/HIV-2, Trinity Biotech, USA or Core™ HIV-1/HIV-2, Core Diagnostics, UK or SD Bioline™ HIV-1/HIV-2, Standard Diagnostics, South Korea) on blood samples. Discordant test results were further evaluated by enzyme immunoassay (EIA) or nucleic acid amplification (NAAT). Infection status with Neisseria gonorrhoeae and Chlamydia trachomatis was determined by performing NAAT on rectal swabs. The infection status of hepatitis A virus (HAV), hepatitis B virus (HBV), hepatitis C virus, and anti-herpes simplex virus type 1 and 2 (HSV-1 and -2) were determined by enzyme-linked immunosorbent assay (ELISA). Treponema pallidum antibody was confirmed by immunochromatography.
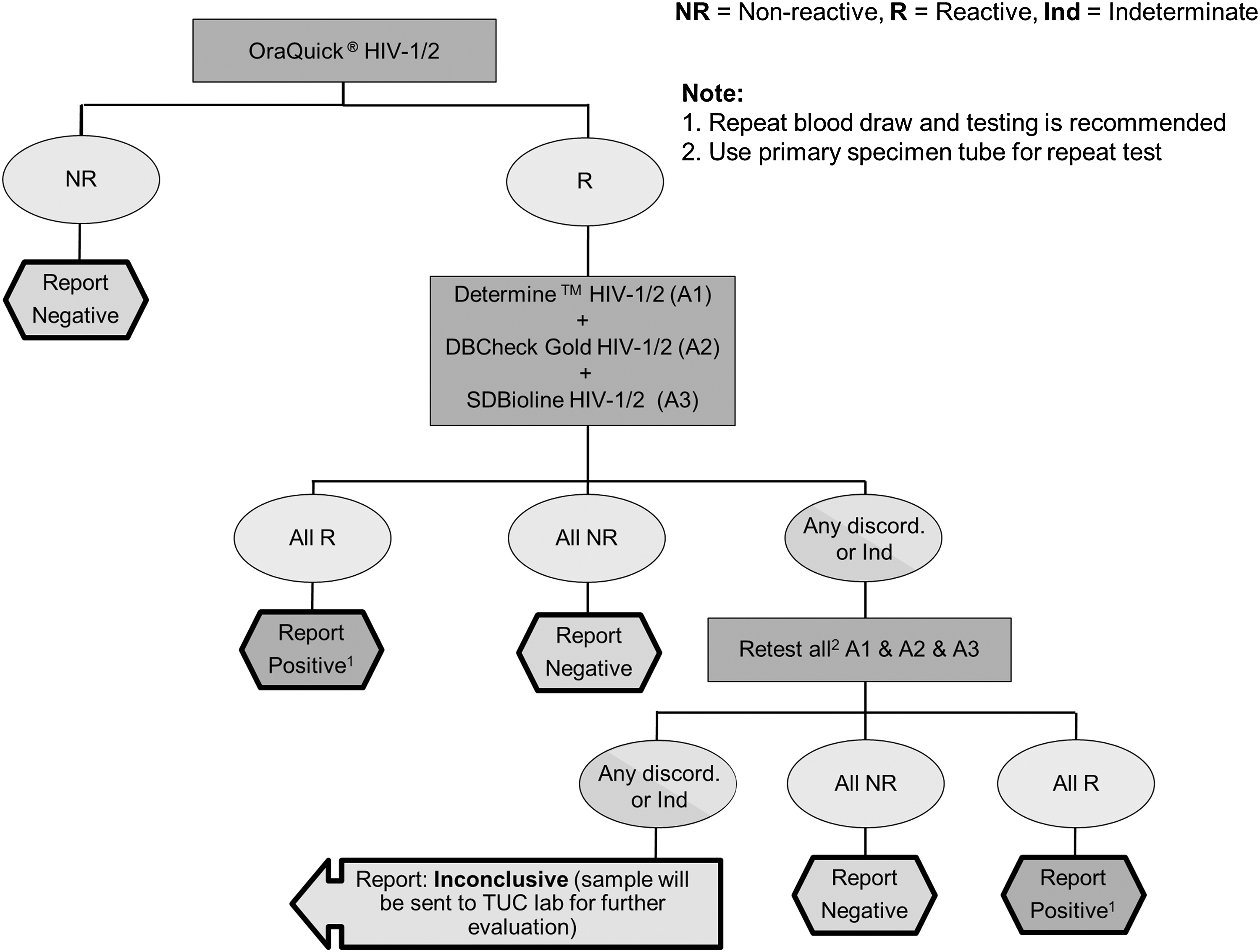
HIV testing algorithm.
HIV-1 genotyping
HIV typing was performed by the multi-region hybridization assay (MHA) and gene sequencing, as previously described. 24 Briefly, HIV-1 RNA was extracted from 200 μl of plasma and subjected to multiregion hybridization (MHAbce), optimized for the detection of HIV-1 subtype B, subtype C, and CRF01_AE. 25 Identification of circulating HIV-1 subtypes by MHA was performed according to established criteria. 22 All apparent cases of dual infection were confirmed by cloning of polymerase chain reaction-amplified nucleic acids, followed by repeating the MHA of individual clones. Samples considered to be apparent dual infections, recombinant, and “non-typeable” by MHA were further characterized by targeted genomic sequencing in HIV-1 p17, gag, rt, int, nef, gp41, gp120, and tat. Sequences were aligned with selected reference subtypes from the Los Alamos HIV-1 database and phylogeny inferred by maximum likelihood. Sequences clustering with a reference subtype with a bootstrap value ≥70% were considered to be of the same subtype as the reference subtype in the region examined. 26 Visual inspection of analyzed trees was used to verify apparent HIV-1 recombinant subtypes.
Measures
Participants were categorized by HIV subtype as “CRF01_AE” if only CRF01_AE was detected by all methods in all gene regions, or “non-CRF01_AE” in all other cases, including purely subtype B infections, recombinants, and dual infections. Study variables included HIV subtype, HIV risk behaviors, and STI screening test results. Time-constant variables, measured at baseline, and time-varying variables, measured at each visit, were collected using ACASI. These variables included participant sociodemographic and behavioral characteristics. The outcome variable assessed was a dichotomized measure of HIV subtype, either CRF01_AE or non-CRF01_AE, including HIV-1 subtype B and intersubtype recombinants. Persons with seroprevalent HIV infection were not included in the analysis.
Behavioral variables
We defined “binge drinking” as self-report of alcohol intoxication occurring more than one time per week in the past 4 months. “Asian partners” were defined as partners of Asian ethnicity other than Thai, and “foreign partners” were defined as partners of non-Asian ethnicity. “Club drugs” included cannabis, ecstasy (MDMA), amphetamine, methamphetamine, ketamine, cocaine, and gamma hydroxybutyrate. We characterized individuals as either “insertive only” or “any receptive” anal intercourse for the variable “anal sex position with male.” IAI is considered to be less risky than RAI, 27 and thus was used as the reference category for this variable. Behavioral data collected in the past 4 months before the time of seroconversion were used in the analysis.
Statistical methods
All analyses were performed using SAS (version 9.3; SAS Institute, USA). Means and proportions were used to describe the sociodemographic characteristics and sexual behaviors at baseline and follow-up visits. We used a competing risk model to analyze risk factors for each specific HIV-1 subtype (AE and other), assuming that infection with the two subtypes was independent. 28 When analyzing incidence of one subtype, seroconversion to the other subtype was treated as a censored observation. Crude subtype-specific HIV incidence rates were calculated as the number of positive cases divided by person-years (per 100 person-years, or PY) of follow-up. Exact 95% Poisson confidence intervals (CIs) were calculated for the estimated subtype-specific HIV-1 incidence rates. We used Cox proportional hazard (PH) analysis for competing risk to identify risk factors associated with each HIV subtype. Variables with a p value ≤.20 for CRF01_AE subtype in bivariate Cox PH model analysis were entered into a backward stepwise multivariable Cox PH model. Due to the small analytic sample of non-CRF01_AE seroconverters, variables with a p value of ≤.25 in the bivariate analysis were included in the backward stepwise multivariable Cox regression model.
Human subjects review
The Thailand Ministry of Public Health Ethics Review Committee for Research in Human Subjects and the CDC Institutional Review Board reviewed and approved this study.
Results
Descriptive analyses
Between April 2006 and December 2014, 1,744 participants were enrolled and followed up in the BMCS, of whom 1,372 were seronegative at enrollment, totaling 4,192 person-years of HIV-free follow-up time. Among the 1,372 participants, 53 (3.9%) identified as TGW. Of these, 2 (3.77%) seroconverted during follow-up, compared to 16.1% that seroconverted among cisgender males. Due to the small numbers, there was insufficient power to analyze TGW separately, and we included these individuals with the MSM in this study. We included a total of 215 seroconverters determined by rapid serologic tests in this analysis with no exclusions: 177 were infected with CRF01_AE (AE subgroup) and 38 were infected with a non-CRF01_AE subtype (i.e., 13 subtype B, 6 CRF01_AE/subtype B dual infections, and 19 CRF01_AE/subtype B recombinants). Mean age among seroconverters was 28 years (range 18–52 years).
CRF01_AE seroconverters
In the AE subgroup, the mean age was 26 years (range 18–48 years), and 38 (21.5%) were 21 years old or less. In sum, 75 (42.4%) had a university education or higher, and 119 (67.2%) lived away from the family (Table 1). During the 4 months before seroconversion, 26 (14.7%) reported using drugs (24/26 to enhance sexual pleasure), 60 (33.9%) reported having 6 or more sexual partners, 82 (46.3%) reported consistent condom use, and 130 (73.4%) engaged in receptive only or both IAI and RAI (combined as “any receptive”). Having a non-Thai Asian partner was reported by 17 (9.6%) in this subgroup, having a non-Asian foreign partner by 14 (7.9%), having been coerced into sex by 33 (18.6%), and participating in group sex by 43 (24.3%). The HBV surface antibody was present in 70 (39.5%) of AE subgroup, HBV core antibody in 68 (38.4%), and HSV-1 antibody was present among 114 (64.4%) at enrollment with 38 (21.5%) having HSV-2 antibody.
Time-varying behavioral variables used in the past 4 months before visit: engaged in binge drinking, used drugs, used club drugs, inhaled nitrates (poppers), drug use to enhance sexual pleasure, used erectile dysfunction drugs, number of sexual partners, condom used with male partners, anal sex position with male partners, Asian partner (not Thai), foreign partner, coerced into sex, paid for sex, received money for sex, group sex; Time-varying laboratory variables used, in the past 4 months before visit: HIV status at time of visit, rectal N. gonorrhoeae, rectal C. trachomatis, HAV antibody, HBV surface antigen, HBV surface antibody, HBV core antibody, HCV antibody, HSV-1 antibody, HSV-2 antibody, T. pallidum antibody; Time-constant variables: age at time of seroconversion, educational level, and living situation at baseline.
Alcohol intoxication 2 to 3 times a week or more.
Club drugs include cannabis, 3,4-methylenedioxy-N-methylamphetamine (MDMA or ecstasy), amphetamine, methamphetamine, ketamine, cocaine, and GHB.
For our Cox models we placed “no anal sex partner” with “condom use always” since there is only one event for AE.
AHR, adjusted hazard ratio; CI, confidence interval; GHB, gamma hydroxybutyrate; HAV, hepatitis A virus; HBV, hepatitis B virus; HCV, hepatitis C virus; HR, hazard ratio; HSV, herpes simplex virus; REF, referent.
Non-CRF01_AE seroconverters
The mean age in the non-AE subgroup was 24 years (range 18–31 years), and 9 (23.7%) were 21 years old or less. In sum, 17 (44.7%) had university education, and 24 (63.2%) lived away from the family (Table 2). During the 4 months before seroconversion, 7 (18.4%) reported using drugs (7/7 to enhance sexual pleasure), 14 (36.8%) reported having 6 or more sexual partners, 18 (47.4%) reported consistent condom use, and 27 (71.1%) engaged in any RAI. During the same time period, having a non-Thai Asian partner was reported by 4 (10.5%) and having a non-Asian foreign partner by 5 (13.2%), having been coerced into sex by 7 (18.4%), and participating in group sex by 12 (31.6%). At enrollment, the HBV surface antibody was present among 21 (55.3%) and HBV core antibody among 11 (28.9%) of non-AE subgroup.
Time-varying behavioral variables used in the past 4 months before visit: engaged in binge drinking, used drugs, used club drugs, inhaled nitrates (poppers), drug use to enhance sexual pleasure, used erectile dysfunction drugs, number of sexual partners, condom used with male partners, anal sex position with male partners, Asian partner (not Thai), foreign partner, coerced into sex, paid for sex, received money for sex, group sex; Time-varying laboratory variables used in the past 4 months before visit: HIV status at time of visit, rectal N. gonorrhoeae, rectal C. trachomatis, HAV antibody, HBV surface antigen, HBV surface antibody, HBV core antibody, HCV antibody, HSV-1 antibody, HSV-2 antibody, Treponema pallidum antibody; Time-constant variables: age at time of seroconversion, educational level, and living situation at baseline; REF, referent.
Alcohol intoxication 2 to 3 times a week or more.
Club drugs include cannabis, 3,4-methylenedioxy-N-methylamphetamine (MDMA or ecstasy), amphetamine, methamphetamine, ketamine, cocaine, and GHB.
For our Cox models we placed “no anal sex partner” with “condom use always” since there were no events for non-AE.
There were no statistically significant differences in the prevalence of STIs, except for HBV surface antibody (p = .04), between the CRF01_AE and non-CRF01_AE seroconverters (39.5% vs. 55.3%, respectively).
Bivariate analysis
In the AE subgroup, the overall HIV incidence (Table 1) was 4.2 PY; among participants aged 18–21 years, the incidence was 6.1 PY. Bivariate analyses suggested that younger age, lower educational level, living alone, reported drug use especially to enhance sex, erectile dysfunction drug use, reported having six or more sex partners, high-risk sex behaviors such as sex without a condom, any RAI, receiving money for sex, group sex, rectal C. trachomatis, HBV surface antibody, HSV-1, HSV-2, and T. pallidum antibodies were associated with incident CRF01_AE seroconversion.
The overall HIV incidence in non-AE seroconverters (Table 2) was 0.91 PY. Among 18- to 21-year olds, the HIV incidence was 1.45 PY. Younger age, reported drug use especially to enhance sex, engaging in high-risk sexual behaviors such as sex without a condom, group sex, and positive tests for HAV antibody and HBV surface antigen were independently associated with non-CRF01_AE seroconversion.
Multivariable analysis
In the multivariable model for infection with CRF01_AE, there were significant associations with age between 18 and 21 years (adjusted hazard ratio [AHR] 2.2, 95% CI: 1.4–3.5), age between 22 and 29 years (AHR 1.6, 95% CI: 1.1–2.3), living alone (AHR 1.5, 95% CI: 1.1–2.1), use of drugs to enhance sexual pleasure (AHR 2.2, 95% CI: 1.4–3.5), intermittent condom use (AHR 1.7, 95% CI: 1.3–2.3), any RAI (AHR 1.7, 95% CI: 1.2–2.4), group sex (AHR 1.5, 95% CI: 1.1–2.2), HSV-1 (AHR 1.5, 95% CI: 1.1–2.1), and T. pallidum seroreactivity (AHR 2.5, 95% CI: 1.4–4.4) (Table 1). In the second multivariable model, infection with non-CRF01_AE (Table 2) was significantly associated with age between 18 and 21 years (AHR 5.1, 95% CI: 1.6–16.5), age between 22 and 29 years (AHR 3.6, 95% CI: 1.3–10.4), use of drugs to enhance sexual pleasure (AHR 3.1, 95% CI: 1.3–7.5), group sex (AHR 2.4, 95% CI: 1.1–5.0), and HBV surface antigen (AHR 3.6, 95% CI: 1.3–10.2).
Discussion
In this study, we examined the relationship between infecting HIV strain and correlates of HIV infection among seroincident HIV cases occurring in Thai MSM and TGW enrolled in the BMCS. We found several biological and behavioral factors that were significantly associated with infection due to the recombinant HIV strain CRF01_AE, and with infection due to other HIV strains. Young age and use of drugs to enhance sexual pleasure were associated with seroconversion of any subtype group. Specifically, CRF01_AE infection was significantly associated with age 18–21 years, any RAI, irregular condom use, use of drugs to enhance sexual pleasure, HSV-1 seropositivity, and T. pallidum seropositivity. In contrast, infection with non-CRF01_AE strains was only associated with age <30 years, use of drugs to enhance sexual pleasure, and active HBV infection.
The factors linked with HIV infection in this study are readily understandable in the context of an epidemic among young Thai MSM and TGW that is largely driven by sexual exposure coupled with suboptimal use of measures to limit transmission risk. RAI is recognized as riskier than insertive intercourse, 29 while regular condom use has been established as a means of reducing the likelihood of infection. 30 Younger age is recognized as an important risk factor for high HIV incidence in previous studies, 31,32 possibly due to larger social networks and/or lack of knowledge about HIV transmission risk in these groups. Impaired judgment due to drug abuse could also lead to increased risk-taking behavior, 6 including IAI in MSM and TGW. 33 –35 HIV infection has also been associated with people who inject drugs (PWID) in Thailand. 36 In Asia, use of methamphetamines and other drugs is an emerging risk factor for HIV among MSM. 3,31,34 HIV and T. pallidum infections may be present simultaneously in infected individuals, and it has been recognized that syphilis aids in the transmission and acquisition of HIV. 37
As noted above, in our population, the associations observed with CRF01_AE infection differed from those that emerged for infection with other viral strains. The reasons for these differences are unclear and could represent selection bias or other forms of sampling error in this study, or true epidemiological differences between viral strains. During the early phases of the HIV epidemic in Thailand, HIV-1 subtype B was the predominant strain among PWID, 38 whereas CRF01_AE was the most common subtype among those exposed through sexual contact. 19 As the epidemic unfolded, CRF01_AE became increasingly prevalent among PWID, and the intermixing of these two common HIV subtypes led to the development of new CRF01_AE/B recombinant subtypes. 20 –23 However, remaining founder effects may underlie strain differences between partially overlapping transmission networks distinguished by particular behavioral and biological risk factors. In local epidemics where multiple subtypes cocirculate, the HIV subtype may therefore be a virologic marker distinguishing diverse groups at risk of HIV infection.
The results presented must be interpreted with some important limitations in mind. The participants in this study were all participants in the BMCS and may not accurately represent MSM or TGW in Bangkok as a whole. In addition, we did not have information on the transmitting partner, which could have been helpful in understanding the link between risk factors and subtype of the transmitting strain. Viral genotyping was performed by MHA and targeted genomic sequencing, and may have failed to detect recombinants with contributions from another subtype in some genomic regions. Finally, the relatively small number of pure subtype B infections seen in our cohort precluded a direct comparison of associations between strain types and may have limited the power to observe associations linked with subtype B infection. Future studies in this area would benefit from larger numbers but may be complicated by the declining incidence of pure subtype B infections in Thailand.
Our analysis furthers our understanding of demographic and behavioral factors associated with HIV transmission among Thai MSM and TGW in Bangkok, where high transmission rates remain a major concern. Reducing the incidence of new infections will require focused efforts in high-risk populations, including those with recent STIs, young MSM, and transgender individuals, for whom epidemiological data are particularly scarce. In these groups, emphasis should be placed on consistent condom use, screening, public health messaging, and education on the hazardous links between recreational drug use and unsafe sexual practices.
Footnotes
Acknowledgment
The authors thank Patrick Sullivan for his support during this analysis, and to Silom Community Clinic staff for their hard work and dedication.
Disclaimer
The findings and conclusions presented in this article are those of the authors and do not necessarily represent the views of the U.S. Centers for Disease Control and Prevention.
Author Disclosure Statement
No competing financial interests exist.