
Abstract
To evaluate the impact of highly active antiretroviral therapy (HAART) on CMV transmission and breast milk level in the context of maternal HIV. Specimens from a randomized trial conducted in Nairobi, Kenya between 2003–2005 were used to compare CMV transmission and breast milk levels between mother-infant pairs randomized to HAART versus short-course antenatal zidovudine plus single-dose nevirapine (ZDV/sdNVP) for prevention of mother-to-child HIV transmission (PMTCT). Fifty-one antiretroviral-naïve women ≤32 weeks gestation, and CD4 between 200–500 cells/mm3 were randomized at 34 weeks to begin either antenatal ZDV/sdNVP, or HAART through 6 months postpartum. Mean breast milk CMV levels and transmission were compared between arms. Age, sociodemographics, CD4%, and HIV plasma RNA viral load were similar between arms at baseline. CMV viral loads were measured from 243 infant plasma and 185 breast milk specimens during the first year postpartum. The probability of infant CMV infection at 12 months was 19% lower in the HAART arm compared to ZDV/sdNVP (75% vs. 94%, p = .04). All women had CMV detected in breast milk, with 72%, 98%, and 97% testing positive during the first, second, and third weeks postpartum, respectively. There was a trend for early higher mean breast milk CMV level in the HAART arm at 1 week (p = .08), and there was significantly slower decline in breast milk CMV levels (area under the curve, p = .01). HAART started during the third trimester may decrease infant CMV infections, by mechanisms independent of breast milk CMV levels. Clinical trials registration: NCT00167674.
Introduction
C
Maternal immunosuppression is associated with an increased risk of infant CMV infection, 9 and with higher CMV levels in the breast milk, cervix, and saliva 12,19 suggesting maternal immune reconstitution during highly active antiretroviral therapy (HAART) may decrease vertical CMV transmission.
Current data on the impact of HAART on vertical CMV transmission are conflicting. A retrospective analysis from the French Perinatal Cohort Study found a decline in the rate of congenital CMV infection with increased use of HAART over time, and less congenital CMV if maternal ART was started in the first or second trimester. 20 Another study reported a higher rate of congenital CMV among women who did not receive antiretrovirals in pregnancy versus those who did. 21 However, an observational study in South Africa found no difference in the rate of congenital CMV infection between women taking antenatal zidovudine versus HAART for the prevention of mother-to-child HIV transmission (PMTCT). 19 The Breastfeeding, Antiretrovirals, and Nutrition Study in Malawi initiated PMTCT in the delivery/postpartum period and did not observe a difference in CMV transmission between study arms. 22 Similarly, an observational study in Malawi found no decrease in breast milk CMV levels with maternal HAART in pregnancy compared to maternal single-dose nevirapine at labor. 23
To simplify the PMTCT cascade, and to maximize efficacy for preventing infant HIV transmission, many countries in sub-Saharan Africa are implementing WHO Option B (HAART for all pregnant women until 1 week after cessation of breastfeeding) or Option B+ (lifelong combination ART for all pregnant women). 24 As more women access Option B/B+ PMTCT regimens, rates of vertical CMV transmission could decline. We hypothesized that maternal HAART would reduce the risk of infant CMV infection and breast milk CMV DNA levels. To test this hypothesis, we compared CMV transmission rates and breast milk CMV DNA levels among women receiving HAART to those receiving short-course antenatal zidovudine plus a single-dose of nevirapine (ZDV/sdNVP) at delivery.
Materials and Methods
Study design
This study utilized specimens and data from a phase II randomized trial comparing the effect of two different PMTCT regimens on breast milk HIV levels (NCT0016767425). The study had 80% power to detect a 0.81-log10 difference in breast milk CMV levels between arms; and 80% power to detect a hazard ratio (HR) of 0.65 or less.
Subject selection, randomization
These studies were approved by the University of Washington Institutional Review Board and the Kenyatta National Hospital Ethics and Research Committee. Pregnant women were recruited and enrolled from the Mathare North Nairobi City Council Clinic from 2003 to 2005, as previously detailed in. 25 Eligibility criteria for the original study included intention to breastfeed, ≤32 weeks gestation, hemoglobin ≥8 g/dl, no previous ART exposure, ≥18 years of age, agreeable to home visits, residence in catchment area, and CD4 > 200 and <500 cells/mm3. Additional criteria for the CMV sub-study included completion of randomization procedures, receipt of intervention, and delivery of a live infant. At enrollment, women provided detailed information regarding sociodemographics, medical and obstetric history, and underwent a physical examination.
At 34 weeks gestation, subjects were allocated to the HAART or ZDV/sdNVP arms using computer-generated block randomization. Women in the HAART arm received 300 mg zidovudine, 150 mg lamivudine, and 200 mg nevirapine twice-daily from 34 weeks until 6 months postpartum. Women in the ZDV/sdNVP arm received 300 mg zidovudine twice-daily from 34 weeks until labor, then every 3 h from labor until delivery plus 200 mg of nevirapine at the onset of labor plus a single 2 mg/kg (6 mg if birth weight >2.5 kg) oral dose of NVP suspension to the infant within 72 h of delivery. 25
Specimen collection and follow-up
Blood was drawn for HIV plasma viral load and CD4 measurements at randomization, and women were seen weekly in clinic thereafter until their delivery. Within 48 h of delivery, maternal blood was drawn for CD4 count and HIV RNA levels and infant blood was drawn for HIV testing. Study staff conducted 1–3 home visits per week during the first month postpartum to collect breast milk, up to a total of 10 times; staff observed manual expression of 5–40 ml of milk from a single breast at each visit. Following removal of the lipid layer, breast milk supernatants were frozen at −80°C. Mothers and infants were followed up in clinic at 2 weeks and 1 month, then every 3 months thereafter until 12 months postpartum. In addition to breast milk, mother and infant blood were collected at each clinic visit.
Laboratory procedures
HIV RNA was measured as previously described 25,26 using the GenProbe assay 27 (Gen-Probe Incorporated, San Diego, California); limits of detection were 100 copies/ml in breast milk and 200 copies/ml in plasma. Infant HIV was diagnosed from dried blood spots as previously described. 28 CD4 counts were performed using the Tri-test flow cytometry platform (Becton Dickinson, Franklin Lakes, New Jersey).
CMV DNA was measured from breast milk supernatants and infant plasma using real-time quantitative polymerase chain reaction detecting the glycoprotein B gene as previously described. 9 The limit of detection was 100 copies/ml for both breast milk and plasma.
Statistical analyses
StataSE version 11.2 (College Station, Texas) was used for all analyses. All tests were two tailed with alpha = 0.05. All comparisons between study arms were conducted as intent-to-treat, unless stated otherwise. HIV and CMV viral load measurements below the limit of detection were recoded to the midpoint between zero and the limit of detection for each assay.
The Mann–Whitney U-test was used to make nonparametric comparisons between variables and Chi square or Fisher's exact tests were used to compare proportions. CMV DNA loads in breast milk were compared between arms using the independent t-test.
Time to infant CMV acquisition and probabilities of CMV infection were estimated using Kaplan–Meier survival analysis; survival functions were compared using the log-rank test. The first detection of CMV DNA was estimated as the time of infant CMV acquisition; infants were considered at risk from birth and data were censored at study exit or death, whichever came first. The z-test was used to compare the probability of infant CMV infection at 3, 6, and 12 months of age. Week 1 and week 2 breast milk CMV viral loads were defined as the last measurement for each woman collected during the first 8 days (n = 45) and first 15 days postpartum (n = 46), respectively.
For comparison of breast milk CMV decline over time, area under the curve (AUC) was estimated for each individual woman, and then mean AUC was calculated across randomization arms, and compared using an independent t-test. Visits were limited to ≤100 days postpartum for this analysis since women in the HAART arm had more follow-up visits after this time, which would artificially inflate their AUC.
Results
Cohort characteristics
Patient selection and follow-up are shown in Figure 1. From a total of 58 women randomized in the parent trial, 51 met criteria for the CMV sub-study, 26 were allocated to HAART, and 25 were allocated to ZDV/sdNVP. All mother-infant pairs underwent CMV assays in the HAART arm. In the ZDV/sdNVP arm, one infant died before blood could be collected, and two women had no adequate breast milk volumes remaining for CMV testing. At 6 months postpartum 25 mother-infant pairs were retained in the HAART arm and 23 retained were in the ZDV/sdNVP arm; at 12 months 12 remained in the HAART arm, 10 remained in the ZDV/sdNVP arm.
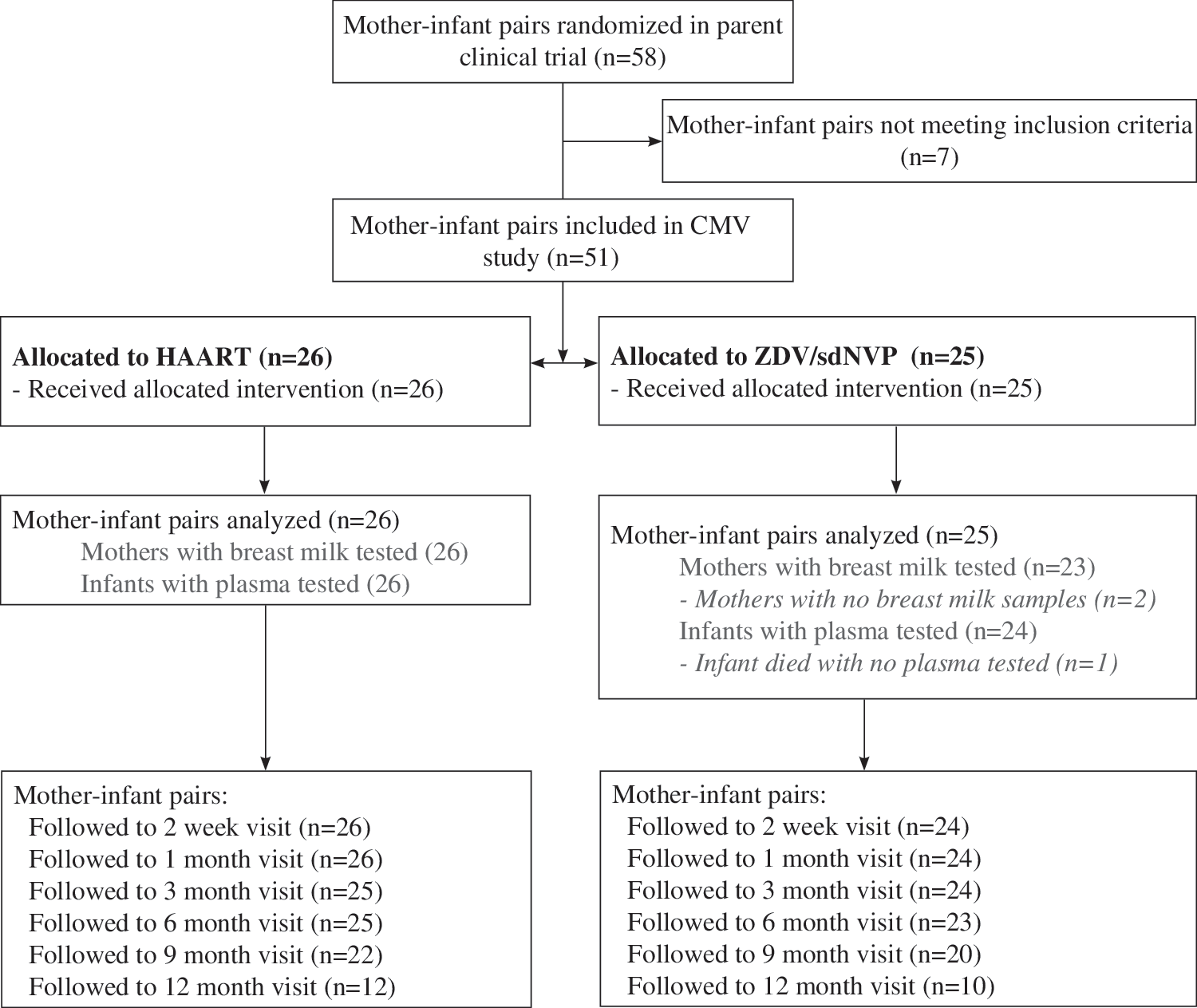
Subject selection and randomization. CMV, cytomegalovirus; HAART, highly active antiretroviral therapy; ZDV/sdNVP, zidovudine plus single-dose nevirapine.
There were no significant differences in demographics, obstetric history, baseline HIV plasma viral load, or CD4 count between women in the two study arms (Table 1). The duration of follow-up and breastfeeding were also similar between women in the two arms. Adherence to treatment allocation and medication (monitored by pill count) was high in both arms, and is discussed in detail in the primary study report (data not shown). 25 However, women randomized to HAART (median = 4 visits, interquartile range [IQR] = 3–5) had more breast milk samples tested for CMV compared to the ZDV/sdNVP arm (median = 3 visits, IQR = 3–4; p = .01) because they tended to breastfeed longer. Three infants acquired HIV during the study; one in ZDV/sdNVP arm and two in the HAART arm. In contrast to the ZDV/sdNVP arm, in which the last antiretroviral dose was given at delivery, women in the HAART arm continued their antiretrovirals for a median of 205 days overall (IQR = 162–225), and 171 days postpartum (IQR = 145–182). No women in the HAART arm stopped ART before the first month postpartum.
n = 25, b n = 23, c n = 24.
CMV, cytomegalovirus; HAART, highly active antiretroviral therapy; IQR, interquartile range; NA, not applicable; PMTCT, prevention of mother-to-child HIV transmission; ZDV/sdNVP, zidovudine plus single-dose nevirapine.
CMV transmission by randomization arm
A total of 243 CMV viral loads were measured from infant plasma specimens. Among the 50 infants evaluated, 42 acquired CMV (84%) by 1 year of age. Two CMV infections were detected at birth (4.0%), and both were in the HAART arm. Figure 2 shows Kaplan–Meier survival curves for CMV DNA detection in the two groups in the intent-to-treat analysis. The curves are similar until 3 months of age, at which time they diverge. The probability of infant CMV infection was significantly lower in the HAART arm compared to the ZDV/sdNVP arm at 6 and 12 months of age (Table 2, p = .04 and p = .04, respectively); with a 1-year probability of CMV infection of 0.75 in the HAART arm and 0.94 in the ZDV/sdNVP arm (Table 2). The median time to CMV infection was 3.0 months (95% confidence interval [95% CI] = 3.0–3.2) in the ZDV/sdNVP arm, and 3.1 months (95% CI = 2.9–6.1) in the HAART arm (p = .2). HAART was associated with an HR of 0.69 in unadjusted analyses (95% CI = 0.37–1.3; p = .2), and an HR of 0.52 (95% CI = 0.26–1.0; p = .06) and 0.57 (95% CI = 0.30–1.1; p = .09) when adjusting for week 1 and week 2 maternal CMV breast milk levels, respectively. We did not find an association between infant risk of CMV acquisition and breast milk CMV levels (week 1 or week 2), baseline maternal plasma HIV viral load, or baseline maternal CD4 percent (data not shown).
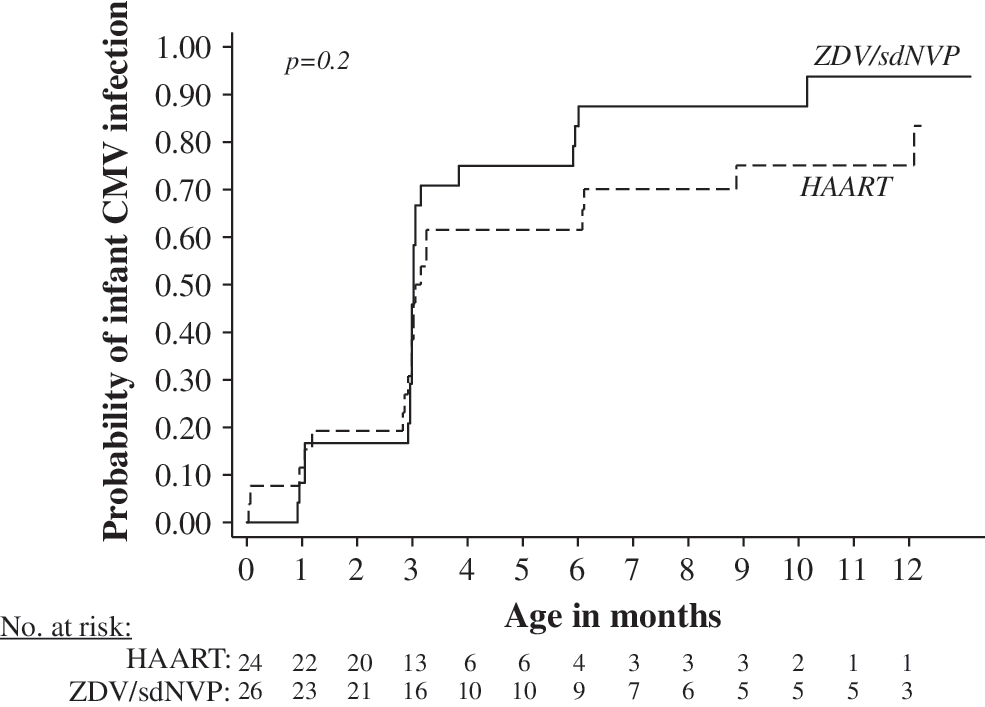
CMV DNA levels and transmission. Kaplan–Meier survival functions show the probability of infant CMV infection by prevention of mother-to-child HIV transmission treatment in randomized infants (47 HIV-exposed uninfected and 3 HIV-infected). p-Value for log-rank test.
Infants also received a single dose of NVP at birth in this treatment group.
95% CI, 95% confidence interval.
Results were similar when excluding the three infants who acquired HIV infection (data not shown), and when analyzing the data “as-treated,” where women were censored when if they stopped taking HAART early (data not shown).
Breast milk CMV detection and levels
A total of 185 CMV DNA measurements were conducted in breast milk from 49 women. CMV DNA was detected at least once in the breast milk of all women studied. Breast milk CMV was detected as early as 1 day postpartum (3/4 women screened in the first day postpartum), and was detected in 72% of women providing specimens during the first week of life. By 2 weeks postpartum, 98% of women had detectable CMV DNA in breast milk.
During the first week postpartum, there was a trend for more frequent detection of CMV DNA (p = .06) and higher CMV DNA levels (p = .08) in the breast milk of women randomized to HAART compared to ZDV/sdNVP (Table 3). CMV viral loads peaked at ∼3 to 4 weeks and slowly declined thereafter in both groups (data not shown). Peak breast milk CMV loads were similar between the two arms (ZDV/sdNVP mean = 5.2 ± standard deviation [SD] = 1.1 log10 CMV DNA copies/ml, vs. HAART mean = 5.4 log10 CMV DNA copies/ml, ±SD = 0.94; p = .5). CMV loads in the HAART arm declined more slowly than in the ZDV/sdNVP arm, as reflected by higher mean AUC (p = .01).
Each woman is represented once per time interval, using the value collected closest to the midpoint of the interval. At each interval, some women are missing a breast milk CMV measurement due to missed visits or inadequate volumes for CMV testing (week 1: n = 2; week 2: n = 9; week 3–4: n = 13). p-Values for comparison of ZDV/sdNVP and HAART arms.
Fisher's exact test.
t-test.
SD, standard deviation.
Discussion
As more women begin taking HAART before or during pregnancy, there is the potential for a secondary impact on vertical CMV transmission. In this small randomized trial, maternal HAART was associated with a lower risk of infant CMV infection at 6 and 12 months of age, but was not associated with lower maternal breast milk CMV levels. In contrast to our hypothesis, there was a trend for modestly increased breast milk CMV levels in women receiving HAART. Together these data suggest that maternal HIV treatment lowers the risk of CMV infection, but this effect is not mediated by reduction of breast milk CMV replication.
There was a lower risk of CMV infection in the HAART arm at 6 and 12 months. This observation is consistent with reports from observational studies reporting lower rates of CMV transmission in cohorts following the introduction of HAART, 20 and our own observation of later CMV transmission in successive cohorts studied over secular time, who were exposed to increasingly efficacious PMTCT regimens. 9,11,29 Our study is also consistent with a study in Malawi that found no difference between breast milk CMV DNA levels at 4–6 weeks postpartum in HAART-treated women compared to women receiving single-dose NVP. 23
Our data suggest the risk of CMV transmission was modified through mechanisms distinct from reducing breast milk CMV levels, such as maternal antibodies. Placental transfer of antibodies to several bacterial and viral antigens are reduced in HIV-infected women, 30 and in a separate Kenyan cohort, maternal HIV viral load was inversely associated with passively transferred measles antibody titers. 31 We thus hypothesize maternal immune reconstitution during HAART could improve passive CMV antibody transfer and reduce infant infection risk without necessarily reducing breast milk CMV levels.
CMV DNA was detected at high levels in the breast milk of most women sampled during the first week postpartum, and peaked at ∼1 month postpartum, following a pattern similar to that observed in HIV-uninfected women. 32,33 Contrary to our hypothesis, women randomized to HAART for PMTCT had a trend for higher CMV DNA levels in the breast milk during the early postpartum period, and had a significantly slower decline in CMV levels. Fortunately, this paradoxical increase did not result in greater CMV transmission risk for women on HAART. Higher CMV loads in the HAART arm were unexpected, but may be explained by changes in the inflammatory environment following HAART initiation. Gianella et al. reported a paradoxical increase in vaginal CMV shedding in nonpregnant Ugandan women starting ART 34 ; the women started ART according to immunologic/clinical criteria and the authors hypothesized that CMV reactivation could be due to inflammation induced by immune reconstitution, which could be conducive to localized CMV replication. Reactivation secondary to ART initiation has also been observed for HSV-2 in the vagina. 35 It is possible that localized inflammation secondary to immune reconstitution in the breast tissue or the milk could explain the increased CMV replication observed in our study. If this is the case, earlier initiation of HAART may provide more time for inflammation to decline before lactation. However, starting HAART earlier in early pregnancy is a challenge for sites where many women do not present for antenatal care until the third trimester. Like many African countries, Kenya national guidelines recommend starting lifelong HAART as early as possible in pregnancy (WHO Option B+), treatment as prevention for discordant couples, and treatment initiation for nonpregnant adults when CD4 counts reach <500 cells/mm3. 36 These programmatic changes may expand earlier HAART initiation in pregnancy, and increase the proportion of HIV-infected women who are already on HAART before conception.
Our study has several important strengths, including longitudinal assessment of early breast milk viral levels and infant CMV. Limitations include the narrow range of maternal CD4 counts and late initiation of HAART, which reduces generalizability and may have attenuated our ability to detect differences between study arms. Inclusion of highly immunosuppressed women may have revealed a greater effect of HAART on breast milk CMV viral load and/or transmission. Similarly, inclusion of women starting HAART over a wider range of gestational ages would better inform how time on HAART affects breast milk CMV levels and transmission risk. Finally, reduced drug adherence or early treatment cessation could attenuate our point estimates, however, censoring of the seven women in the HAART arm who discontinued treatment early did not affect our results in an as-treated analysis (data not shown).
In summary, although our study was small, our data suggest HAART reduces the risk of CMV transmission from HIV-infected women. As WHO Option B+ becomes available to an increasing number of women in sub-Saharan Africa, it will be important to determine the impact of longer-term maternal HAART on CMV transmission and maternal CMV replication.
Footnotes
Acknowledgments
We would like to acknowledge the contributions of the research personnel, laboratory staff, and data management teams in Nairobi, Kenya and Seattle, Washington; the Mathare North City Council Clinic for their participation and cooperation; the Divisions of Obstetrics and Gynaecology and Paediatrics at Kenyatta National Hospital for providing facilities for laboratory and data analysis. We thank the Kizazi Working Group and the UW Global WACh for comments and insights provided during article development. Most of all, we thank the women and children who participated in the study. This publication was made possible with support from the National Institutes of Health (NIH) awards K01AI087369 and K23AI065222 from the National Institute of Allergy and Infectious Diseases (NIAID, PIs JAS, and MHC), and K24HD054314 from the National Institute of Child Health and Disease (NICHD, PI GJ-S); and the Elizabeth Glaser Pediatric AIDS Foundation Scientist Award (#11-03, PI GJ-S). VCE was supported by the University College London Medical Research Council (MRC) Centre for Medical Molecular Virology. This research was also supported by the University of Washington Center for AIDS Research (CFAR), an NIH funded program (P30AI027757). Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the funders.
Conference presentation: These data were presented in part, as a poster at the 8th Annual International AIDS Society (IAS) Conference on HIV Pathogenesis, Treatment and Prevention, Vancouver, 19–22 July, 2015.
Author Disclosure Statement
No competing financial interests exist.