
Abstract
Viral and host factors are known to play a role in the different patterns of AIDS progression. The cocirculation of HIV-1 subtypes B, F1, BBR, and BF1; the occasional detection of HIV-1 subtype D; and an increasing prevalence of subtype C and other recombinant forms have been described in Rio de Janeiro, Brazil. The aim of this study was to evaluate the potential association of HIV-1 subtypes circulating among HIV-1+ individuals in Rio de Janeiro with AIDS disease progression. For this purpose, 246 HIV-1 individuals under clinical and laboratory follow-up from 1986 to 2011 were classified according to their progression to AIDS in typical progressors (n = 133), rapid progressors (n = 95), and long-term nonprogressors (n = 18). The env-gp120 region was amplified and sequenced. Neighbor-joining phylogenetic inferences were performed in Mega 6 and bootscan analysis was performed in Simplot 3.5.1. The Kaplan–Meier method and Cox modeling were performed to determine the time until an AIDS-defining event based on the HIV-1 subtypes/variants. Similar AIDS progression rates were observed among individuals infected with HIV-1 subtype B and variant BBR. However, a direct association between more rapid AIDS progression and HIV-1 subtypes, D and BF1, was confirmed in the multivariate analysis, corroborating previous results. Our findings contribute to the investigation of the possible influence of HIV-1 subtypes in AIDS outcome.
Introduction
H
The most striking aspect of HIV diversity could be detected in the envelope (env) gene, which is therefore considered a highly polymorphic region that contains valuable phylogenetic information. This genomic region encodes two viral glycoproteins exposed on the viral surface: gp120, which interacts with the cell receptor CD4, and gp41, which promotes virus fusion to the cell membrane. 4 The env region is a determinant of cell tropism; it contains epitopes recognized by antibodies that neutralize HIV infection in vitro and stimulates a potent cytotoxic and helper immune response by T lymphocytes. 4 Thus, this region provides relevant information to understand the selective forces that may influence the disease progression rate, possibly as HIV subtype-specific differences, 5 –8 and could be extremely useful in molecular epidemiology studies. 9,10
The HIV-1 group M viruses, responsible for the AIDS pandemic, are divided into nine subtypes (A–D, F–H, J, and K), with unique and circulating recombinant forms 11 that are distinctly spread worldwide. In Brazil, for most geographic regions, the HIV molecular epidemic presents a predominance of HIV-1 subtype B (60%–90%), followed by sub-subtype F1 (2%–22.2%) and recombinant genomes BF1 (1.2%–38%). 9,12 –18 However, the southern region depicts a different scenario, where HIV-1 subtype C (3%–66%) and recombinant BC genomes (1.9%–31.8%) cocirculate more frequently. The overall prevalence of these non-B strains, as well as of rare HIV-1 subtypes D and CRF02_AG, has been increasing over time during the AIDS Brazilian epidemic. 9,10,15,19 –22
In addition, previous studies concerning the genetic and antigenic characteristics of HIV-1 subtype B in Brazil allowed the description of a Brazilian variant called BBR. This variant presents the amino acid, tryptophan (W), instead of proline (P) on the top of V3 loop, which is prevalent in the pandemic subtype B. 12,23 –25 Brazil is considered the epicenter of the BBR epidemic, 26,27 but these viruses are occasionally found in other countries. However, this variant is quite prevalent in Brazil, where its frequency ranges from 17% to 50% of the B subtype samples. 9,10,12,28 –30
The association between disease progression and HIV-1 subtypes has been widely documented. 8,20,29,31 –40 In African countries, some studies reported higher morbidity, faster AIDS progression, a more pronounced CD4 count decline, and a higher probability of having X4 virus in individuals infected with HIV-1 subtype D compared with individuals with subtype A infections. 34 –38 Nevertheless, no difference was detected in the plasma viral load between these subtypes. In England, faster CD4 decline and a higher rate of subsequent virological failure were also verified among individuals infected with HIV-1 subtype D. 39
In Brazil, some studies have suggested a slower progression in individuals infected with HIV-1 BBR compared with the pandemic subtype B viruses. 29,31,32,40 A recent study revealed that BF1 recombinants could be more pathogenic than subtype B. 20 Thus, the present study aimed to evaluate the influence of HIV-1 Brazilian subtypes on distinct AIDS progression profiles.
Materials and Methods
Study population
HIV-1 seropositive individuals (n = 4,015) were retrospectively identified from a cohort followed-up at the National Institute of Infectious Diseases of Oswaldo Cruz Foundation (INI/FIOCRUZ) in Rio de Janeiro, Brazil, from 1986 to 2011. The inclusion criteria were described in Teixeira et al. 22 The HIV-1 infection date was estimated based on the midpoint of the last seronegative and the first seropositive tests and was only considered if ≤36 months. The time to AIDS progression was considered the time elapsed between the estimated date of infection and the first instance of one of the following AIDS-defining events: CD4+ T-lymphocyte count below 350 cells/mm3, AIDS-defining illness (according to the Brazilian Ministry of Health Guidelines), 41 initiation of HIV antiretroviral therapy, or AIDS-related death. Therefore, based on the definition of time to AIDS progression, all individuals were naïve to HIV antiretroviral therapy. Briefly, individuals were classified as (a) rapid progressors (RPs) if presenting an AIDS-defining event within 3 years after estimated date of HIV-1 infection; (b) typical progressors (TPs) if presenting an AIDS-defining event more than 4 years after the estimated date of HIV-1 infection; or (c) long-term nonprogressors (LTNPs) if the individuals had an asymptomatic HIV-1 infection for >10 years after the estimated date of HIV-1 infection. After we defined the inclusion criteria and the parameters to be obtained for the classification according to AIDS progression, we used the INI database, which contained sociodemographic and clinical information, to obtain an automated classification. Based on the evaluated parameters, 3,809 individuals met the inclusion criteria and, of those individuals, 496 could be categorized according to their progression profile, whereas the remaining 3,313 individuals did not fulfill the criteria for the disease progression classification. The 496 classified individuals were categorized as follows: 182 as RPs (36.7%), 289 as TPs (58.3%), and 25 as LTNPs (5.0%).The present study was approved by the INI-FIOCRUZ Ethics Research Committee (Ethics Committee CAE: 0002.0.009.000–08) as an anonymous unlinked study. Because we could not obtain informed consent from all individuals, they were deidentified before analysis. For this study, a confidentiality letter was signed by the research responsible, ensuring the individual's anonymity.
DNA extraction, amplification, and sequencing
For subtype characterization, DNA was extracted from whole blood using a QIAamp DNA Blood Mini Kit (Qiagen, Hilden, North Rhine-Westphalia, Germany) according to the manufacturer's instructions.
The env-gp120 C2-V3 region was amplified by polymerase chain reaction (PCR) using nested primers as described elsewhere. 42 The PCR amplicons were purified using a purification kit (GE Healthcare, Little Chalfont, Buckinghamshire, United Kingdom) and sequenced on an ABI 3100 Genetic Analyzer (Applied Biosystems, Foster City, CA) using the ABI BigDye Terminator v.3.1 Cycle Sequencing Ready Reaction kit (Applied Biosystems).
HIV-1 subtyping
We were able to subtype 246 of the 496 individuals categorized according to their AIDS progression profile. Of these 246 subjects, 186 had biological material available, and HIV-1 characterization was performed by phylogenetic and recombination analyses. The remaining 60 samples had been previously characterized in studies carried out in our laboratory by heteroduplex mobility assay (HMA) of the env-region. 13,43,44 HIV-1 subtype B samples were then subjected to restriction fragment length polymorphism analysis with the FOKI enzyme to discriminate the BBR variant. 13,42
Sequences were assembled and edited using the SeqMan software (DNAStar, Madison, WI) and then aligned with reference sequences from the Los Alamos database (
Statistical analyses
Kaplan–Meier survival analysis and Cox proportional hazard models were used to investigate differences in the elapsed time between the HIV-1 infection date and AIDS-defining event for all classified individuals. Survival curves were plotted using the Kaplan–Meier method, and the categories of each analyzed variable were compared using the log-rank test with a 5% level of significance. To evaluate the factors associated with AIDS progression, variables that had a significant effect on the hazard ratio (HR) with an event occurrence of less than 20% (based on the Wald test) were evaluated in the model. The models were compared using the likelihood ratio test (ANOVA) with significance level of 5%. The assumptions of the Cox models and the quality of adjustment were made, respectively, based on the residuals and coefficients of determination, as well as the likelihood of agreement to evaluate the discriminatory power and predictive accuracy of the model. R software version 2.15.2 with the survival library was used to run these analyses. 47
Results
Clinical and epidemiological characteristics
The 246 individuals who were classified according to their progression profile and who had their subtype determined were categorized as follows: 95 RPs (38.6%), 133 TPs (54.1%), and 18 LTNPs (7.3%).
The sociodemographic data of the classified and subtyped group are summarized in Table 1. In general, 67.5% were male, 57.7% self-identified as white, 41.1% were older than 30 years, 45.9% had fundamental schooling, and 47.2% self-reported as men who have sex with men or bisexual.
RP, rapid progressor; TP, typical progressor; LTNP, long-term nonprogressor; n, number of individuals; MSM, men who have sex with men; NR, not reported; SD, standard deviation; IDU, injecting drug users; Other, blood transfusion, vertical transmission, and percutaneous exposure.
HIV subtype distribution
Based on either previous HMA assays or phylogenetic and recombination analyses (Fig. 1), 246 individuals had their HIV-1 env viral subtype determined. From these analyses, 147 (59.8%) were classified as subtype B; 61 (24.8%) as BBR variant; 23 (9.3%) as sub-subtype F1; 7 (2.9%) as subtype C; 3 (1.2%) as subtype D; 3 (1.2%) as recombinant BF1; 1 (0.4%) as CRF01_AE, and 1 (0.4%) as recombinant BD (Table 1).

Neighbor-joining phylogenetic tree from 182 HIV-1 C2-V3 pure env sequences (367 bp) and bootscan analyses from the four recombinant sequences (URFs). Black branches represent the reference sequences from HIV-1 group M. Bootstrap values above 70 are represented only in major clusters by asterisks. The scale bar indicates a 3% divergence of the nucleotide sequences. Bootscan analyses were performed on a sliding window of 200 nt by increments of 10 nt. Reference samples from subtype B, subtype F1, subtype D, and subtype C were used for these analyses. Color images available online at
Survival analysis
In the Kaplan–Meier survival analysis, the general median time between the HIV-1 infection date and the AIDS-defining event was 1,804 days (95% confidence interval [CI] 1,596–1,984 days). It is noteworthy that the median survival times of subtypes B and variant BBR were similar (median 1,881 vs. 1,808, respectively). For HIV-1F1 and HIV-1C, the median time was 1,670 days (95% CI 847–2,869 days) and 976 days (95% CI: 144-NA days), respectively. The mean time of the HIV-1 BF1 and D genotypes was 208 and 366 days, respectively, and the time to an AIDS-defining event for HIV-1 BD and CRF01_AE individuals was 2,426 and 563 days, respectively (Table 2 and Fig. 2). The HIV-1 subtypes (p < .01) and the sociodemographic variables, including gender (p < .01), age at date of HIV-1 infection (p < .05), schooling (p < .05), and exposure category (p < .05), were identified as having statistically significant influence on differences in the time to AIDS progression in this analysis (Table 2).
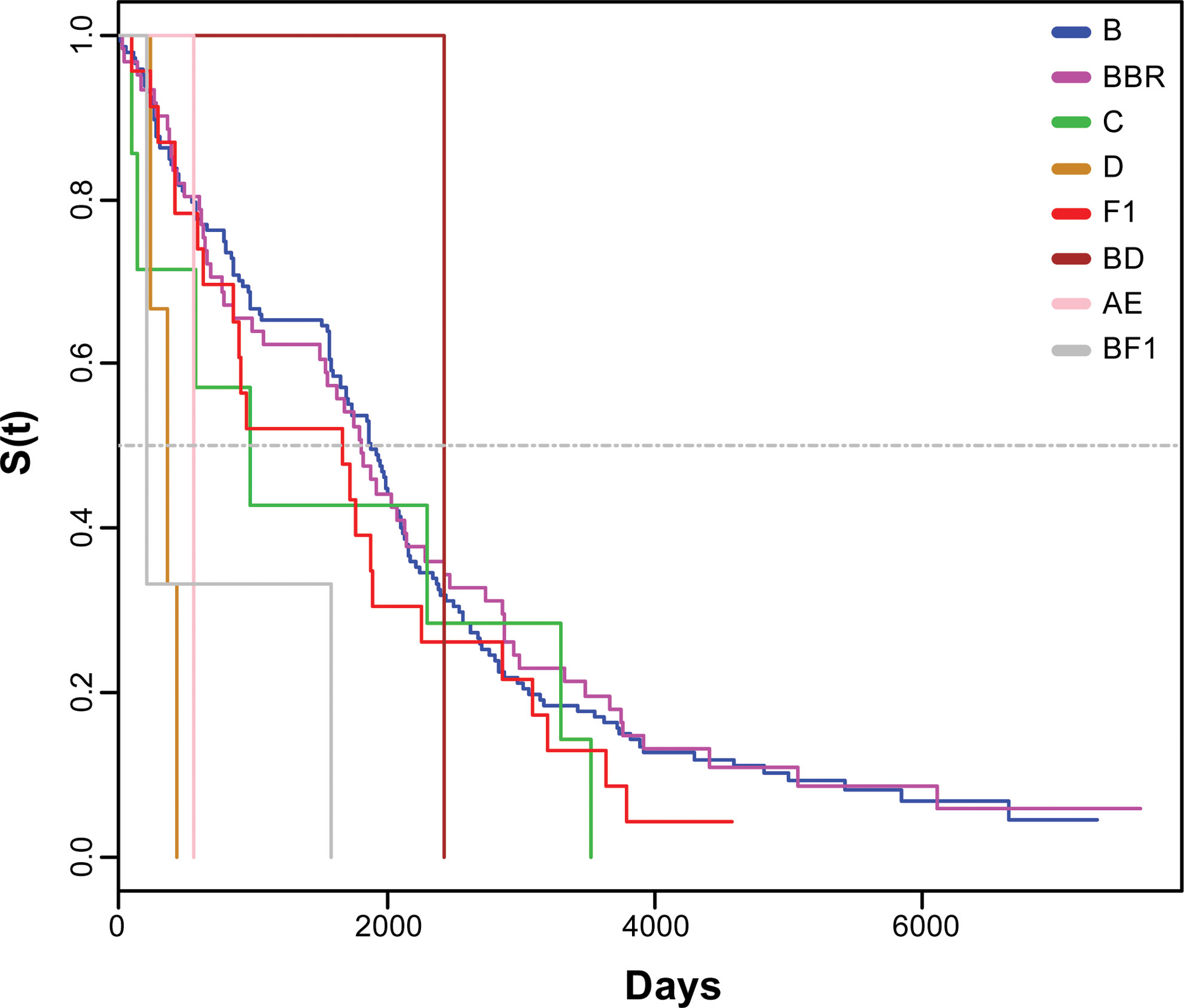
Analysis of disease progression. Kaplan–Meier survival curves were used to estimate time to an AIDS progression event according to the HIV-1 subtypes. Color images available online at
Bold numbers indicate significant p value.
CI, confidence interval; NA, not achieved.
In the bivariate analysis, we confirmed that these categories, with the exception of schooling, were associated with AIDS progression (Table 3). Thus, we performed a multivariate analysis to these categories (with the exception of the exposure category because data were missing for 15 individuals) and HIV-1 viral subtypes (B, BBR, C, D, F1, and BF1). This analysis showed significant differences in the fastest time to AIDS progression for males (p < .01), older individuals (p < .05), and HIV-1 subtypes D (p = .001) and BF1 (p < .05) compared with HIV-1B (Table 3). Controlling for these variables, the estimated HR was detected in the multivariate analysis for HIV-1D (HR: 6.88; 95% CI 2.12–22.33; p < .01) and HIV-1 BF1 (HR: 4.69; 95% CI 1.46–15.09; p < .05), as well as for male individuals (HR: 1.56; 95% CI 1.17–2.08; p < .01) and older diagnosed individuals (HR: 1.02; 95% CI 1.00–1.04; p < .05) (Table 3). The variables included in the model complied with the assumptions of the Cox model.
Bold numbers indicate p value ≤ .05.
15 missing data (n = 229).
HR, hazard ratio.
Discussion
Some genetic host factors were associated with HIV-1 acquisition risk and/or might have an important impact on AIDS progression. The influences of HIV-1 genetic diversity, viral fitness, and coreceptor tropism have also been suggested as determinants affecting AIDS progression. 1,35,48,59 The CCR5-delta 32 polymorphism reduces the chance of HIV infection in individuals with a homozygous genotype, whereas the presence of this polymorphism in heterozygotes is associated with slower disease progression. 49 –51 Likewise, some specific HLA class I and KIR alleles, including the HLA-B*27, B*57, B*52, and KIR3DL1 and 2DL2 alleles, have been implicated in HIV control, leading to slower AIDS progression. 22,52 –59 However, alleles, HLA-B*35 and 53, are associated with more rapid AIDS progression. 60,61 Relating to the virus, in vitro studies reveal distinct replicative viral fitness among HIV types, groups, and subtypes. 62 Higher fitness is observed in HIV-1 subtypes B and D infections, followed by subtypes A and C. 63 Regarding coreceptor tropism, R5 viruses usually predominate during primary HIV infection, whereas X4 viruses often emerge in late stages of HIV disease, with the latter being associated with rapid CD4+ T-cell depletion and consequent AIDS progression. 64 –66 Thus, in the present study, we investigated the influence of HIV-1 subtypes prevalent in Brazil on AIDS progression.
In Brazil, some studies based on survival analysis showed a slower progression in individuals infected with the HIV-1BBR variant compared with the pandemic subtype B. 31,32,40 It is noteworthy that these studies used a subtyping technique based on a serological test with synthetic peptides, which is less sensitive and which may result in incorrect classification, HIV-1 subtypes F1, and pandemic subtype B have a similar V3 consensus. For example, according to Santoro-Lopes et al., 31 of 331 individuals with an HIV-1B subtype, over 62% were characterized as HIV-1BBR, which is a much higher percentage than expected for this variant based on molecular approaches. 9,10,12 In the present study, we detected similar AIDS progression rates between HIV-1B and BBR, which is in agreement with the findings reported by Sucupira et al., who described similar frequencies of X4 viruses for both clades. 7 To our knowledge, our study is the first to compare distinct clinical outcomes in individuals infected with HIV-1 pandemic subtype B or the BBR variant based on sequence analysis.
In the present study, all individuals infected with HIV-1 subtype D had a rapid AIDS progression profile, which is consistent with previous data that demonstrated a quick decay of CD4+ T cells during the course of HIV infection and high X4 viral proportion since the beginning of infection with this subtype compared with HIV-1 subtype A. It is important to note that HIV-1D has a low prevalence in Brazil, which explains the small number of individuals infected with this subtype herein and the few available studies concerning this subtype in this country. 13,67 –69 In both bivariate and multivariate analyses, we also detected that individuals infected with HIV-1BF1 had rapid progression to AIDS. Corroborating this finding, a recent study demonstrated that this phenomenon is a consequence of an accelerated rate of CD4+ T-cell loss. 20 This recombinant form is most prevalent in South America and its impact on the Brazilian AIDS epidemic is of relevance. Thus, our findings corroborate that HIV-1D and HIV-1BF1 could be more pathogenic compared with HIV-1B and other non-B viruses.
Slower AIDS progression was observed for individuals infected with HIV-1C compared with individuals infected with HIV-1B. This slower progression has been associated with the lower replication efficiency of the virus in macrophages and CD4+ T lymphocytes, as well as reduced common coreceptor switching from CCR5 to CXCR4, which could be associated with more mutations required in the env region of HIV-1C than of other subtypes. 70 –73 However, we detected a minor median time to an AIDS-defining event for this subtype in relation to either HIV-1 subtype B or BBR, although there was no association with AIDS progression.
In general, studies addressing this subject present limitations such as the short time of cohort follow-up, 74 the lack of infection date, 33,35,75 and the analysis of only one HIV-1 genomic region ( 8,39,48 and the present study). Despite having an initially large cohort, because of the retrospective nature of this study, missing epidemiological characteristics and/or dates of clinical events resulted in a large number of nonclassified individuals. Together with the absence of biological material from some classified individuals, these factors led to a reduced final cohort. One of the strengths of this work was the use of rigorous criteria that allowed better classification of the cohort based on their AIDS progression profiles.
In conclusion, we observed similar progression between subtypes B and the variant BBR, indicating the low probability of a relationship between this variant and slower progression to AIDS, and we corroborated evidence that HIV-1D and BF1 are risk factors for more AIDS progression. Furthermore, these and previous findings concerning the role of HIV-1 subtypes in the infection outcome add important pieces to the understanding of HIV pathogenesis, vaccine development, and the complex molecular epidemiological dynamics in regions where these subtypes and recombinant viruses are prevalent, as well as to the value of early initiation of antiretroviral therapy principally for those individuals with HIV-1 subtypes associated with more rapid AIDS progression.
Footnotes
Acknowledgments
The authors acknowledge Dr.Vera Bongertz for her review and suggestions. The authors thank the individuals for consenting to participate in this study. They also thank CNPq and FAPERJ as funding sources. M.L.G. and M.G.M. are recipients of a CNPq scholarship, and Thaysse Cristina Neiva Ferreira Leite is a recipient of a CAPES scholarship. Sequence data: All nucleotide sequences are available in the GenBank database (accession numbers KT595420–KT595605).
Author Disclosure Statement
No competing financial interests exist.