
Abstract
The aim of this study was to compare the extent of resistance to antiretroviral (ARV) drugs among the population in Mexico before and after 2005. The mutations and drug resistance database of Stanford University were used for analyzing drug resistance tests that had been performed on HIV treatment-naive patients. The sequences obtained were divided into group 1 (isolated in 2002–2003) and group 2 (isolated in 2010–2014). Both groups showed 14% similarity in resistance mutations. In both groups, mutations in N88D protease inhibitor were identified, D67N and T69D were found for nucleoside reverse transcriptase inhibitors (NRTIs), and K103N was found for non-nucleoside reverse transcriptase inhibitors. In both groups, the resistance to ARV drugs was 7.4%. Both groups showed resistance to nelfinavir, efavirenz, and nevirapine. The prevalence of resistance to ARV therapy remained stable from 2002 to 2014. However, a marked reduction in resistance to NRTIs was observed for the same period.
G
The study was conducted from 2002 to 2014 in three specialized public hospitals in western Mexico. Samples were collected from patients naive to ART and with evidence of disease progression (>5,000 RNA copies/ml and CD4 < 500 cells/μl). Signed informed consent was obtained from patients, and then plasma samples were collected and stored at −80°C until genotypic testing.
RNA extraction was performed using the QIAamp viral RNA kit (Qiagen, Hilden, Germany) and following the manufacturer's instructions. Viral RNA was transcribed to complementary DNA, and this was followed by a sequencing reaction that included the protease gene (codons 1–99) and the partial reverse transcriptase gene (codons 40–247) using the TruGene assay (Siemens, Toronto, Canada). The sequencing reaction was direct double-stranded sequencing and performed using an automated sequencer. The resulting sequences were compared with the reference strain HIV-B-LAV1.
Resistance mutations were determined according to the World Health Organization Surveillance Drug Resistance Mutation (SDRM) list (2009) with the Calibrated Population Resistance Tool. 6 Genotypic ART resistance was determined using the HIVdb program, Stanford University. 6 Resistance to ART was classified as high, intermediate, or low. The samples were divided into two groups: group 1 included samples that were collected before 2005 and group 2 included samples collected after 2005. During 2005, the prevalence of drug resistance was reported, 5 and universal access to ART was extended throughout the country. The results were reported as averages and percentages.
From HIV-1-positive patients who were naive to ART, 216 sequences were obtained. Of these, 95 sequences formed group 1 (2002–2003), and 36 (2010), 49 (2011), 17 (2012), 16 (2013), and 3 (2014) sequences formed group 2. Group 1 included 86 males and 9 females, with an average 299,834 copies/ml of HIV-1 RNA and an average CD4 cell count of 214 cells/μl. Group 2 included 101 males and 20 females, with an average 654,551 copies/ml of HIV-1 RNA and an average CD4 cell count of 256.92 cells/μl.
Sequences with SDRM were found in 14.7% (n = 14) of group 1, where 3.2% of mutations were specific for PIs, 11.6% were for NRTIs, 5.3% were for NNRTIs, 3.2% were for NRTI+NNRTI, and 1.1% were for NRTI+NNRTI+PI. Whereas in group 2, 14% (n = 17) of sequences had SDRM, 3.3% were for PI, 4.1% were for NRTI, and 6.6% were for NNRTI, and for the combinations of NRTI+NNRTI and NRTI+NNRTI+PI, no sequences were found (0%). The N88D mutation for PI was found in each group (1.1%) and other SDRMs were found in group 1; D30N, V82A, and I85V, and each for 1.1% of the group. In group 2, F53LY (1.7%) and L90M (1.7%) were found. SDRM for NRTI was found in both groups: D67N (1.1%) and T69D (1.1%). In group 1, other mutations were also found: K70R (1.1%), V75A (2.1%), F77L (3.2%), M184V (3.2%), L210W (1.1%), T215YC (2.1%), and K219N (1.1%). In group 2, M41L (1.7%) and T215SD (2.5%) were found. For NNRTI, K103N was found in both groups with 3.2% in group 1 and 1.7% in group 2. Other mutations found in group 1 included Y181CI (2.1%), and those in group 2 included K101E (0.8%), K103S (1.7%), G190AS (1.7%), and M230L (0.8%).
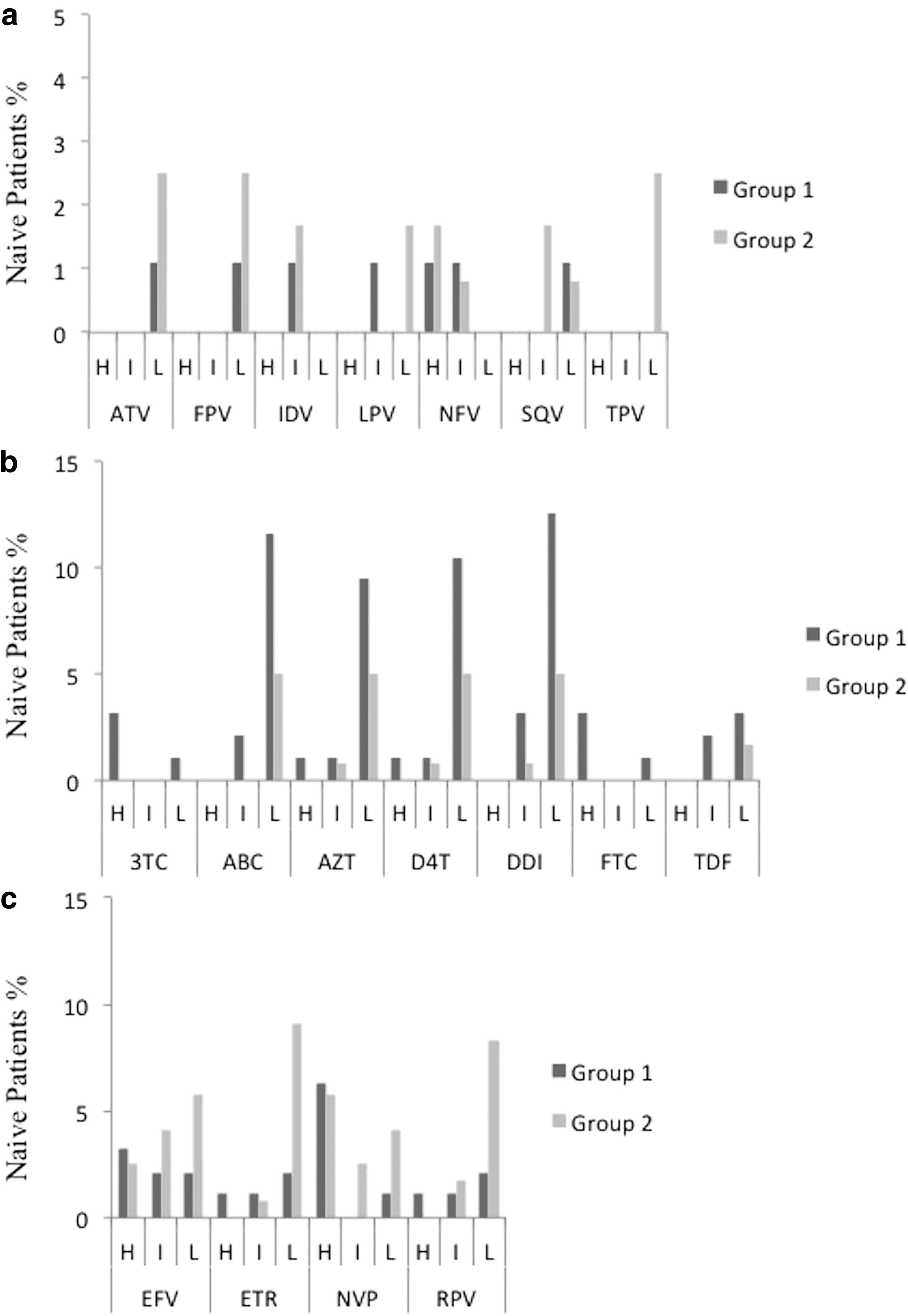
The resistance to ART was determined as 7.4% for both groups. The occurrence of intermediate and low levels of resistance in group 1 was 2.1% and 12.6%, respectively. In group 2, the occurrence of an intermediate level of resistance was 5%, and that for low levels of resistance was 9%. A high level of resistance to PIs was observed for nelfinavir in 1.1% for group 1 and 1.7% for group 2. For the remaining ARVs, intermediate or low levels of resistance were observed (Fig. 1a). No level of resistance was observed for darunavir. In group 1, NRTI resistance was observed in 8.4% of the sequences, where 3.2% exhibited resistance to lamivudine, 1.1% to zidovudine, 1.1% to stavudine, and 3.2% to emtricitabine. In group 2, a high level of resistance to NRTI was not observed (Fig. 1b). A high level of resistance to NNRTI was observed in 11.6% of group 1 and 8.3% of group 2. Group 1 showed levels of resistance to all ARVs, where 3.2% of the group exhibited resistance to efavirenz, 1.1% to etravirine, 6.3% to nevirapine, and 1.1% to rilpivirine. In group 2, the amount of resistance for efavirenz was 2.5% and that for nevirapine was 5.8% (Fig. 1c).
Drug resistance in antiretroviral-naive patients in Mexico.
This is the first report that has analyzed sequences in Mexico since 2002 and provides a recent comparative data set. All sequences were analyzed equally, rather than simply analyzing previously published data in a different way. In this study, it was observed that the prevalence of resistance to ART generally remained stable between 2002 and 2014. This confirms expectations for Latin America. 7,2 However, a higher than expected prevalence was observed for Mexico. 2,8 Prevalence was expected to have decreased with the incorporation of new ARV agents and therapeutic strategies, improved universal access to treatment, the utilization of guidelines for prescribing ART in public medical services, and the use of genotyping for establishing and adapting the treatment regimens for patients. In addition, strategies to reduce HIV transmission through the provision of treatment immediately after initial diagnosis (Test and Treat) have been implemented in Mexico from ∼2010. The United States and Western Europe have reported a stable trend in TDR in recent years, where these developed countries have had a decrease in the rate of transmission. 9
Previously, we described the presence of secondary mutations with a high probability of inducing resistance to PI. 10 Primary resistance to PI has remained stable over the years. Resistance to NNRTIs has decreased from 11.6% to 8.3%. SDRM and resistance to NRTI were observed to have decreased, with the prevalence of resistance to ART decreasing from 8.4% to 0%. These data do not match those reported by Pineda-Peña, 2 whose findings showed an increase in resistance to PI. The findings of this study are consistent with the trends reported in North America and Europe. 4,7 These trends can be explained by the initial prescription of monotherapies and bitherapies of NRTIs, which generated an increased resistance to this group of inhibitors. However, the use of highly active antiretroviral therapy has decreased the resistance observed for NRTI. 2,4,11 Another difference or trend observed in the data was that the sequences from samples collected in 2002–2003 had dual-class drug resistance, which was not observed in samples from 2010 to 2014. Contradictory results on the prevalence of TDR also exist in the literature, 3 with some reports of stable trends in certain countries or decreased transmission in developed countries, 9 and other reports describing an increase 7,12 Therefore, it is necessary to understand the regional and temporal patterns of ARV resistance. 11,13
Why does the prevalence of TDR not decrease, and what is affecting this change? In this sample population from Mexico, a reduced and controlled level of NRTI resistance was observed. Why the prevalence of resistance remains? We understand that there are some problems in the public health system. What can we do to control resistance? With universal access to ART, the goal of reduced resistance should be achieved. However, late diagnosis and lack of physician training remain, resulting in the inappropriate use of treatment guidelines and lack in monitoring of treatment efficacy. 2 Even though there is complicated bureaucracy when referring patients to specialists, the lack of adherence to treatment holds a major influence, and therefore adherence-promoting interventions for the physician and patient are recommended. 8,9,13 Lastly, it is important to have reliable tests for resistance to generate the correct ART regimen.
One limitation of our study was the focus on a geographical area in western Mexico, which has medical services with experience in the care of people living with HIV that is slightly different among the regions of Mexico. In addition to this, there is travel and migration to and from the United States and other countries. Continued vigilance is recommended to achieve a decrease in the prevalence of ART resistance.
Genbank Accession Numbers
EU045452; EU045453; EU045464; EU045466; EU045468; EU045481; EU045490; EU045491; EU045504; EU045506; EU045509; EU045524; GU291863-GU291866; GU291868-GU291895; GU291897-GU291915; GU291917-GU291928; GU291931-GU291932; GU291934-GU291943; GU291945-GU291955; KX253694-KX253940
Footnotes
Author Disclosure Statement
No competing financial interests exist.