
Abstract
Plasma gelsolin (pGSN) is a multifunctional protein involved mainly in severing and clearing of actin filaments. Its level correlates with inflammation and several diseases making it a potential biomarker of diagnostic and prognostic values. The pGSN level in groups of treated and untreated HIV-1-infected Indian patients is investigated in this study. This study aims at investigating the levels of pGSN in HIV-1-infected patients across different age, sex, severity of disease, and treatment status. Blood samples of 213 patients were analyzed for CD4 counts by flow cytometry and pGSN was quantified by enzyme-linked immunosorbent assay (ELISA). The level of pGSN is significantly increased in HIV-1 infected patients (227.2 ± 54.3 μg/ml) compared to healthy volunteers (167.9 ± 61.8 μg/ml). The level correlates with CD4 cell counts as patients with lower CD4 counts showed higher pGSN levels and vice versa. Gender does not affect pGSN level; however, antiretroviral (ARV) treatment reduces pGSN toward normal. Within low CD4 cell count group, the untreated patients have 52% higher pGSN than healthy volunteers, whereas with treatment, the difference reduces to 24%. Similarly, high CD4 cell count (>350 cells/mm3) group of patients showed 44% increase in pGSN in untreated patients compared to 21% increase in treated patients. There is an upregulation of pGSN in HIV-1 infection and it is inversely correlated with CD4 cell counts. Treatment with ARV drugs decreases pGSN levels toward normal. The monitoring of pGSN level in HIV-1-infected patients could be an important indicator of severity of disease and recovery during treatment.
Introduction
P
Consistent with these anticipated functions, hypogelsolinemia (20%–50% of normal level) has been reported in many diseases involving tissue injuries and infections. A number of diseases, including major/minor trauma, chronic inflammatory diseases like rheumatoid arthritis, acute injuries of liver, and lung injury, burns, myocardial infarction, septic shock, myonecrosis, severe falciparum malaria, allogeneic hematopoietic stem cell transplantation, and preeclampsia (a pregnancy-related complication), have been associated with a subnormal level of pGSN. 8,10 –17 In hepatitis B virus-related chronic liver disease, the level of gelsolin has been shown to decrease with the severity of pathogenic condition, which becomes lowest for acute-on-chronic liver failure patients. 18 Apart from these, lower level of pGSN has been found to be associated with an increased risk of death for critically ill surgical patients. 19
In contrast to depletion of pGSN levels in infectious diseases, plasma proteome analysis of disease development after infection with Trypanosoma cruzi in a rodent model (Sprague-Dawley rats) of Chagas disease and human failing hearts diagnosed with end-stage ischemic and dilated cardiomyopathy has shown increased level of gelsolin. 20,21 Also, gelsolin protein has been shown to increase in hypertrophic and dilated cardiomyopathic racET mouse hearts. 21 Besides, increased pGSN levels were observed in sera of HIV-1-infected patients who developed dementia compared to patients without dementia, whereas differential expression of pGSN levels were seen in Cerebrospinal Fluid. 22,23
The focus of this study was to estimate pGSN levels in HIV-1-infected patients and correlate it with disease progression. Further investigation was done to ascertain the effect of antiretroviral therapy (ART) on pGSN levels. The outcomes of the study indicated that pGSN levels were increased markedly by 44%–52% in HIV-1-infected patients. Data indicated that the ART brought pGSN levels toward normal values.
Materials and Methods
Study design
The study was conducted at Rajendra Memorial Research Institute of Medical Sciences (RMRIMS; Patna, India). A total of 213 HIV-1-infected patients were enrolled from different districts of Bihar, India. As control subjects, 34 healthy volunteers were enrolled for this study. Out of 213 patients, 114 were males and 99 were females of different ages from 2 to 63 years. This included 105 naive patients who were not treated with any antiretroviral (ARV) drugs. The remaining 108 patients were treated with first-line ARV drugs. These drugs are ZLN (Zidovudine, 300 mg; Lamivudine, 150 mg, and Nevirapine, 200 mg) or SLN (Stavudine, 30 mg in place of Zidovudin in case of anemic patients). In case of patients with coinfection of tuberculosis, Nevirapine was replaced with Efavirenz (600 mg). Liver function tests such as serum bilirubin, alanine transaminase (ALT), aspartate aminotransferase (AST), and alkaline phosphatase (ALP) were performed in patients with hepatic diseases. These tests were regularly performed in patients who were given Nevirapine. The control group of healthy volunteers included 20 males and 14 females between 16 and 48 years of age. The distribution of volunteers was 3/3, 7/4, 5/4, and 5/3 males/females in 0–20, 21–30, 31–40, and above 40 years age groups, respectively. In HIV-1-infected patients, the CD4 lymphocyte count is the most important factor to initiate ARV drug treatment and monitor the disease progression. Based on CD4 cell counts, patients were divided into four groups; treatment-naive HIV-1-infected patients with low CD4 cell count (<350 cells/mm3), treatment-naive HIV-1-infected patients with high CD4 cell count (>350 cells/mm3), HIV-1-infected patients with low CD4 cell count (<350 cells/mm3) on ART, and HIV-1-infected patients with high CD4 cell count (>350 cells/mm3) on ART. The CD4 cell count of children below 5 years is generally very high. Therefore, the ratio of CD4 T lymphocytes to total lymphocyte count was considered while categorizing them in high/low CD4 groups. The children with 25% or more CD4 cells of total lymphocytes were placed in high CD4 group and those with <25% were considered low CD4. Children were treated based on clinical situations irrespective of CD4 cell counts as per recommendations of National AIDS Control Organisation (NACO), Government of India.
Sample collection
After taking written informed consent, blood samples were collected from HIV-1-infected patients at ART centre of RMRIMS. The samples were collected from healthy volunteers at the blood collection center in the out patient department of RMRIMS. Every patient was given a patient identification number and proper records were kept for the date of blood collection, sex, age, and ART drug regimen. Collection of blood was done in sitting position of patients by venipuncture at median cubital vein. Two milliliters of blood was taken from each patient with the help of a single-use plunger attached to an EDTA blood collection tube. In case of children below 10 years, 1 ml of blood was taken. Blood was mixed with EDTA present in the tube by inverting the tube. The blood collection was carried out between 11 AM and 1 PM. For patients on ARV drugs, blood collection was done after 4 weeks of start/change of medication. Blood plasma was isolated immediately and stored at −80°C for estimation of pGSN. CD4 cells were counted within 24 h of blood collection using flow cytometry. The processing of blood was done under biosafety cabinet and all needles, collection tubes, gloves, absorbent cottons, and so on used in the collection and processing the samples were incinerated.
Ethics statement
The approval for study and blood collection from HIV-1-infected patients was given by RMRIMS ethics review board. A written consent was taken from every patient (guardian for patients below 18 years of age), informing the use of blood sample for research purpose.
Plasma isolation
Blood was transferred to 5 ml centrifuge tubes and was centrifuged at 1,000 × g for 10 min in a refrigerated centrifuge at 4°C. The clear supernatant, that is, blood plasma was transferred to 1.5 ml tubes. Tubes were labeled with identification codes and stored at −80°C. The used EDTA tubes, gloves, and other discards were incinerated with proper care.
CD4 T lymphocyte count
The CD4 T lymphocyte count of blood samples were analyzed using flow cytometry (FACS; Becton Dickinson Biosciences). In the FACS tube, 50 μl blood samples were taken and a mixture of CD4-specific surface antibodies (raised against CD3, CD4, and CD45 cell surface markers) was added. The tubes were vortexed and incubated in dark at room temperature. After 20 min of incubation, 1 ml of 1 × FACS lysis buffer was added and mixed by vortexing for 15 s. It was incubated for 10 min in dark at room temperature. After incubation, 2 ml of stain buffer was added and mixed by vortexing. It was centrifuged at 1,200 rpm for 10 min. The solution was decanted from the FACS tube and washed again with the stain buffer. Finally, the stain buffer was decanted and 200 μl of phosphate-buffered saline (PBS) was added to the tube. An isotype control was treated similarly in all the steps except addition of surface antibodies. Readings were acquired and samples were analyzed using CellQuest Pro software on FACSCalibur (Becton Dickinson Biosciences).
Quantification of pGSN levels in plasma using enzyme-linked immunosorbent assay
The antibodies against recombinant human pGSN were raised in rabbit as described previously. 24 An indirect enzyme-linked immunosorbent assay (ELISA) was employed to determine the pGSN levels in HIV-1-infected patients with or without ART having low (<350 cells/mm3)/high (>350 cells/mm3) CD4 cell count. Briefly, plasma was kept at 4°C for thawing. It was sequentially diluted 1:5,000 times in a coating buffer comprising of 100 mM NaHCO3, pH 8.2. On the other hand, recombinant human gelsolin standard (0.3 mg/ml) was diluted with a coating buffer to get concentrations 50, 100, 200, 300, 400, 600, 800, and 1,000 ng/ml. In the 96-well plate, 100 μl of each sample (diluted gelsolin standards and diluted plasma samples) was coated and incubated overnight at 4°C. After 16 h of incubation, the samples were discarded and plates were washed thrice with 1 × PBS. In each well, 300 μl of freshly prepared 3% bovine serum albumin (BSA) in 1 × PBS was added and the plates were incubated at room temperature. After 4 h of incubation, BSA was discarded and the plates were washed thrice with 1 × PBS. Then, 100 μl of rabbit anti-gelsolin polyclonal antibody (1:3,000 in 1% BSA) was added to each well and the plate was incubated at 4°C. After overnight incubation, primary antibody was discarded and the plate was washed thrice with PBS containing 0.1% Tween (PBST) followed by thrice with 1 × PBS. In each well, 100 μl of secondary antibody (anti rabbit, 1:5,000 in 1% BSA) was added and it was incubated at room temperature. After 1 h of incubation, secondary antibody was discarded and plates were washed thrice with PBST followed by washing thrice with 1 × PBS. 100 μl of TMB substrate for ELISA (Thermo Scientific) was added to each well and kept for 2–3 min (till visible color difference appeared). Reaction was stopped with 100 μl of stop solution comprising of 2 M H2SO4. Absorbance was taken in ELISA reader (Bio-Rad) at 450 nm. Unknown concentration of the pGSN in samples was estimated by the linear fit of absorbance values from samples containing predetermined amounts of recombinant human pGSN.
Statistics
The results are expressed as the mean ± standard deviation. The statistical significance of the pGSN levels was evaluated by using one-way analysis of variance followed by the post hoc Tukey's multiple comparison test. The differences were considered significant if the probability values were <.05.
Results
pGSN level in patients with low (<350 cells/mm3)/high (>350 cells/mm3) CD4 lymphocyte counts
CD4 lymphocyte count in HIV-1-infected patients is the most important factor to monitor HIV-1 infection progression and initiate ARV drug treatment. According to 2013 WHO guidelines, the treatment is started in patients with a CD4 threshold of 500 cells/mm3 or less for adults, adolescents, and older children, but priority is given to patients with an even lower CD4 lymphocyte count (<350 cells/mm3). This study was designed to understand the possibility of pGSN, an upcoming marker of health status, as biomarker for HIV-1 infection and/or AIDS therapy regime. Our first target was to analyze the level of pGSN in patients with a critical level of CD4 cells (<350 cells/mm3), where ARV drug treatment generally starts. To investigate this, 213 randomly selected patients were enrolled, which included both males and females within the age group 2–63 years. Blood sample was taken for CD4 cell count as well as for blood plasma isolation. CD4 lymphocyte was counted using FACSCalibur flow cytometer (Becton Dickinson Biosciences) as described in the Materials and Methods section. On the basis of CD4 cell counts, two groups were formed. The first group of 107 patients represented HIV-1-infected patients having CD4 cell count <350 cells/mm3 (low CD4), whereas the second group of 106 patients was formed by patients having CD4 cell count >350 cells/mm3 (high CD4). On the other hand, plasma was isolated from the same samples and the pGSN level estimation assay was performed as described in the Materials and Methods section. The pGSN level of each patient was calculated in μg/ml. A control group of 34 healthy individuals was formed to compare the gelsolin level of HIV-1-infected patients. pGSN levels were analyzed for all the three groups and an average of each group was plotted in graph (Fig. 1). The pGSN level in the control group was found to be 167.9 ± 61.8 μg/ml, and the levels were significantly higher in the HIV-1-infected patients (227.2 ± 54.3 μg/ml). Moreover, a trend was observed in the pattern of pGSN as a function of their CD4 counts. In the HIV-1-infected, high CD4 cell count (>350 cells/mm3) patients, the average pGSN level was 221.3 ± 55.2 μg/ml, while in low CD4 cell count (<350 cells/mm3) patients, it was 233.0 ± 53.1 μg/ml. The percentage increase in pGSN compared to healthy individual controls was calculated. A significant increase of 31.8% was observed in the high CD4 cell count (>350 cells/mm3) group, while a 38.8% increase was observed for low CD4 cell count (<350 cells/mm3) HIV-1-infected patients.
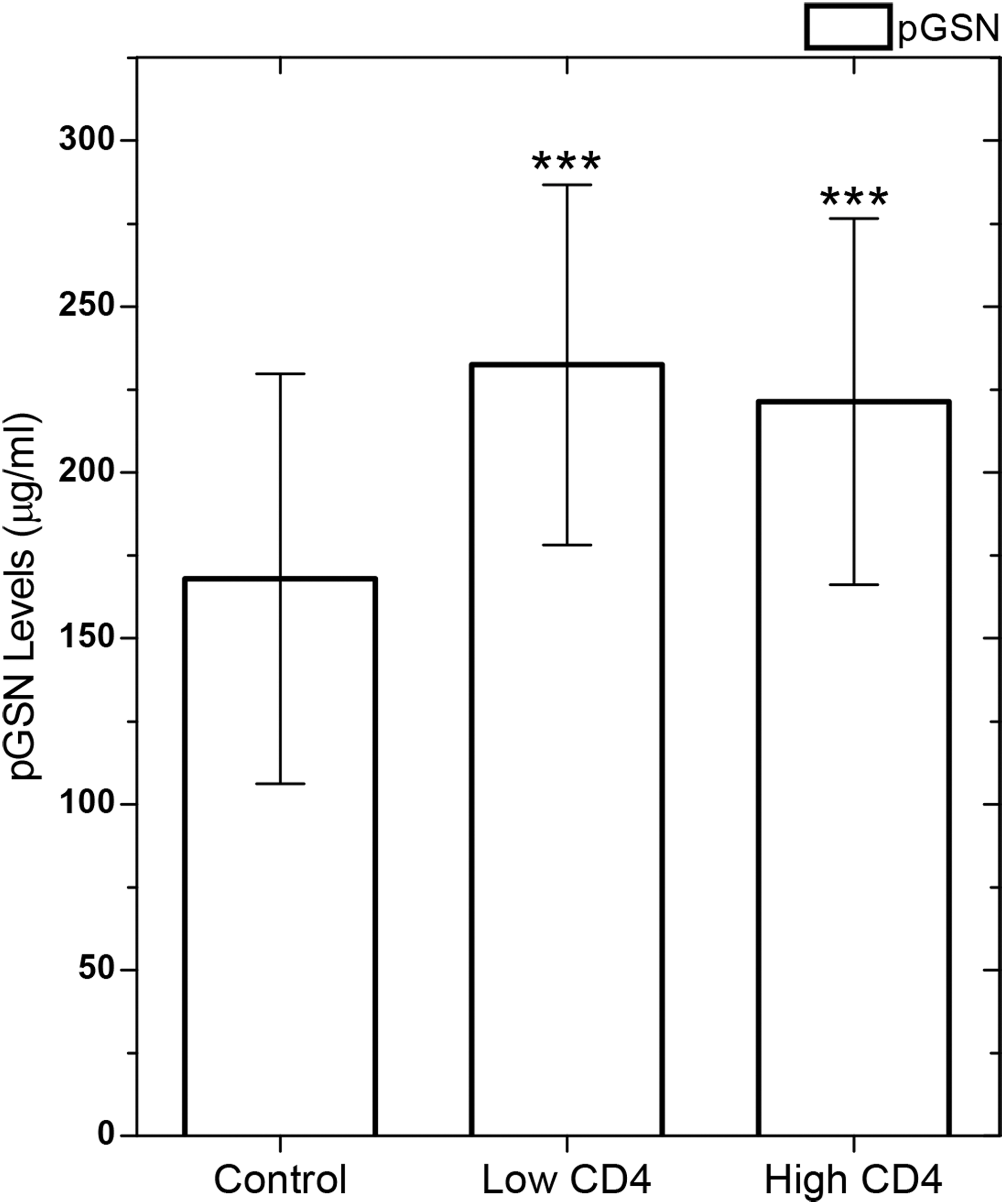
pGSN level in HIV-1-infected patients with low (<350 cells/mm3) and high (>350 cells/mm3) CD4 lymphocyte counts. CD4 cells were counted using flow cytometry and two groups were formed, a low CD4 group having CD4 cell count <350 cells/mm3 and a high CD4 group having CD4 cell count >350 cells/mm3. Control group was formed by healthy volunteers. pGSN level was obtained individually in μg/ml and an average of each group was calculated. Data are represented as average ± SD. The p-values <.001 compared with healthy control values are shown as ***. pGSN, plasma gelsolin; SD, standard deviation.
pGSN level in patients with/without ART
ART is mostly started when CD4 cell count becomes <350 cells/mm3. On ARV drug therapy, the CD4 cell count generally increases or resumes to normalcy. The next step was to analyze the pGSN level in treatment-naive HIV-1-infected patients and patients on ART. Out of 213 patients in our study, 105 patients were treatment naïve and 108 were ARV drug-treated HIV-1-infected patients. The pGSN concentration in treatment-naive HIV-1-infected patients group (non-ART) was 249.0 ± 51.5 μg/ml, which was much higher compared with the ART group of HIV-1-infected patients, 206.0 ± 48.5 μg/ml. pGSN concentrations of treatment-naive and ART groups of HIV-1-infected patients were plotted as a graph with control healthy volunteers' pGSN level (Fig. 2). The pGSN level indicated a significant increase of 48.3% in the treatment-naive HIV-1-infected patients' group, which was much higher than the ARV drug-treated group with a 22.7% increase compared to the healthy control group. The significantly lesser gelsolin level in ART patients compared to treatment-naive HIV-1-infected patients shows the effect of ARV drugs on pGSN levels.
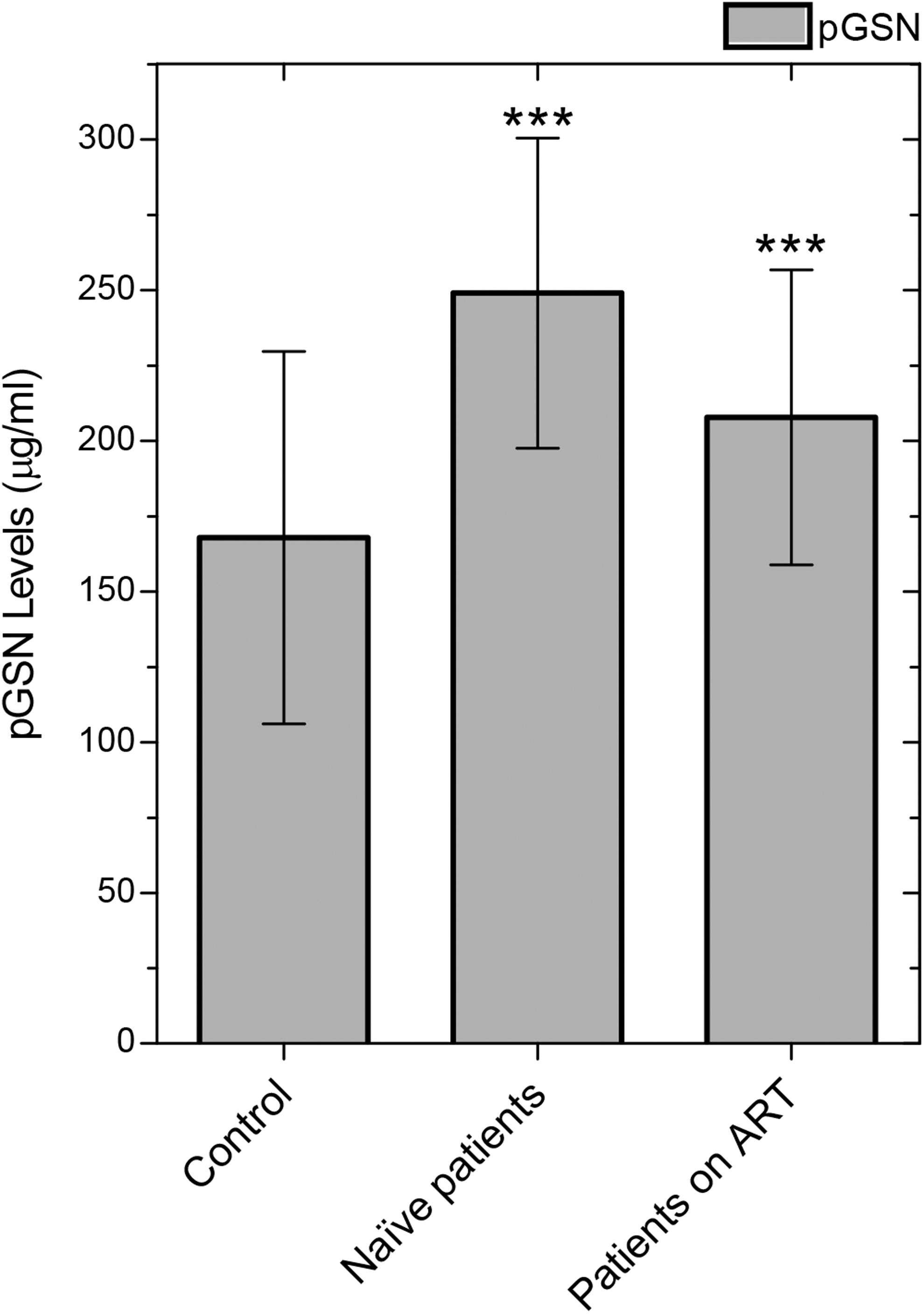
pGSN levels in HIV-1-infected ART/treatment-naive patients. The treatment-naive group was formed by 105 patients who were never given an ARV drug. The other group was of 108 patients who were on ARV drugs. Control group was made by healthy volunteers. Significantly higher gelsolin was observed in treatment-naive HIV-1-infected patients compared to patients on ART. Both the ART and treatment-naive groups exhibited higher pGSN levels than the control group. Data are represented as average ± SD. The p-values <.001 compared with healthy control values are shown as ***. ART, antiretroviral therapy; ARV, antiretroviral.
Gelsolin level in treatment-naive and ARV drug-treated HIV-1-infected patients with high (>350 cells/mm3)/low (<350 cells/mm3) CD4 lymphocyte counts
The observations of above two studies individually indicated a higher gelsolin level in the low CD4 cell count group (<350 cells/mm3) as well as in treatment-naive HIV-1-infected patients, who were never given antiretroviral drugs. The next step was to combine these two studies and elaborate the effect of CD4 cell count in treatment-naive and ARV drug-treated HIV-1-infected patients. Four different study groups of HIV-1-infected subjects were formed. First group was of treatment-naive HIV-1-infected patients having a low CD4 cell count (<350 cells/mm3). Second group composed of treatment-naive HIV-1-infected patients having a high CD4 cell count (>350 cells/mm3). Last two groups were of patients on ART with low CD4 cell count (<350 cells/mm3) and ART with high CD4 cell count (>350 cells/mm3). The control samples were obtained from healthy individuals. Out of 213 patients recruited for the study, 56 were treatment-naive HIV-1-infected patients having a low CD4 cell count (<350 cells/mm3), 49 were treatment-naive HIV-1-infected patients with high CD4 cell count (>350 cells/mm3), 51 were ART patients with low CD4 cell count (<350 cells/mm3), and 57 were ART patients having a high CD4 cell count (>350 cells/mm3). An average pGSN concentration was calculated separately for the above four groups. In the control group of 34 healthy individuals, the pGSN concentration was 167.9 ± 61.8 μg/ml. In treatment-naive HIV-1-infected patients, the pGSN level in the low CD4 cell count (<350 cells/mm3) group was 255.1 ± 52.1 μg/ml, whereas in the high CD4 cell count (>350 cells/mm3) group, it was 242.0 ± 50.4 μg/ml. In ARV drug-treated patients, the pGSN concentration in the low CD4 cell count (<350 cells/mm3) group was 208.8 ± 42.9 μg/ml and in the high CD4 cell count (>350 cells/mm3) group, it was 203.5 ± 53.3 μg/ml (Fig. 3). From the above result, it was illustrated that within the treatment-naive and ART groups, low CD4 cell count (<350 cells/mm3) patients have higher gelsolin concentration in their plasma, quantitatively, compared to healthy control group. Treatment-naive HIV-1-infected patients showed 51.9% and 44.1% more pGSN in low and high CD4 cell count (>350 cells/mm3) groups, respectively, whereas in ARV drug-treated patients, a 24.35% and 21.2% increase in pGSN was observed for low (<350 cells/mm3) and high (>350 cells/mm3) CD4 cell groups, respectively.
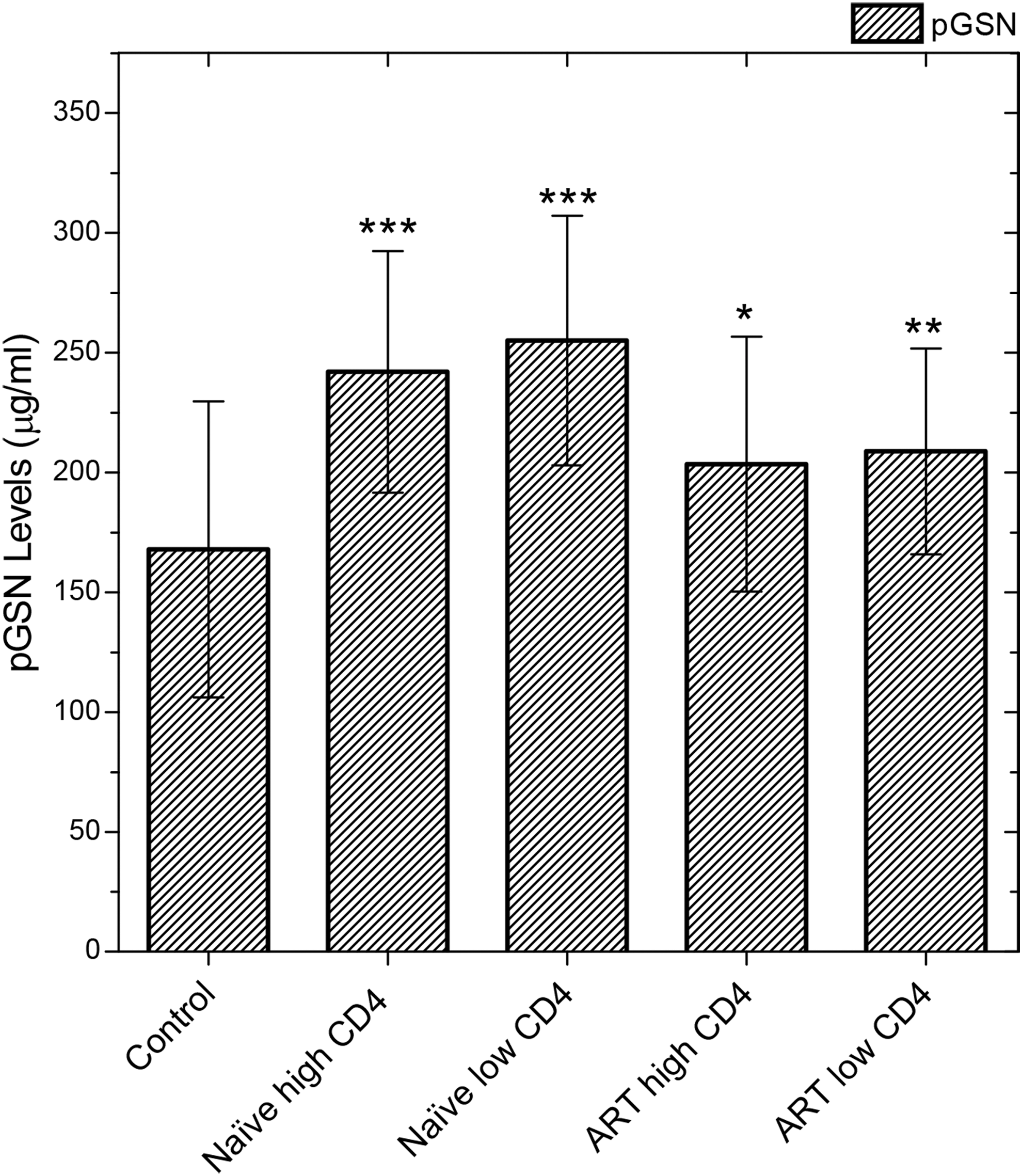
pGSN levels in HIV-1-infected treatment-naive and ART patients having low (<350 cells/mm3) or high (>350 cells/mm3) CD4 count. Four groups were made by dividing treatment-naive and ART groups on the basis of CD4 cell count. First two groups were of treatment-naive HIV-1-infected patients having low (<350 cells/mm3) and high (>350 cells/mm3) CD4 lymphocyte counts, respectively. Third and fourth groups were of ART patients with low (<350 cells/mm3) and high (>350 cells/mm3) CD4 counts. The control samples were obtained from healthy volunteers. Data are represented as average ± SD. The p-values <.001, <.01, and <.05 compared to treatment-naive patients with healthy control and ART patients with treatment-naive patients are shown as ***, **, and *, respectively.
An important aspect of the result is the decrease in pGSN level toward normalcy for patients on ART even with CD4 cell count <350 cells/mm3. Gelsolin starts decreasing immediately with the ARV drug treatment. Therefore, the level of pGSN is an early indicator of health improvement even before restoration of CD4 cell count.
Gelsolin level in male/female with high (>350 cells/mm3)/low (<350 cells/mm3) CD4 cell counts in treatment-naive and ART HIV-1-infected patients
Above experiments clarified a regular trend that treatment-naive HIV-1-infected patients have a higher concentration of pGSN than ARV-treated patients and within these groups, low CD4 cell count (<350 cells/mm3) is associated with higher pGSN. Furthermore, we wanted to understand the gender dependence of pGSN within the above groups. Revisiting the pGSN data obtained for 114 males and 99 females who participated in the above study, we compared the pGSN concentration between male and female for each group separately. Average pGSN concentrations obtained with number of male and female in the groups are given in Table 1. Importantly, we found that there was no significant difference in average pGSN levels of males and females within the groups.
ART, antiretroviral therapy.
Gelsolin level in HIV-1-infected patients of different age groups
To understand the impact of age of HIV-1-infected patients on pGSN concentration, we segregated data as per age of patients. Patients were divided into four groups; 18 patients of 0–20 years, 69 patients of 21–30 years, 70 patients of 31–40 years, and 56 patients above 40 years. Graph was plotted for pGSN concentration against each age group (Fig. 4). It was observed that the concentration of pGSN was 242.5 ± 50.1 μg/ml for 21–30 years age group, while for other three groups, the concentration was almost equal (221.6 ± 49.7 μg/ml for 0–20 years, 220.6 ± 54.3 μg/ml for 31–40 years, and 218.5 ± 58.3 μg/ml for the above 40 years age group).

pGSN concentration in HIV-1-infected patients of different age groups. Four groups were made with the age range 0–20, 21–30, 31–40, and >40 years. Slightly higher concentration was observed in 21–30 years age group and all other groups showed comparable pGSN values. Data are represented as average ± SD. The p-values <.001 and <.05 compared with healthy control values are shown as *** and *, respectively.
Discussion
In last few years, pGSN has emerged as an important biomarker candidate for several diseases. Its level has been shown to decrease significantly in most of the diseases except in Chagas and end-stage ischemic- and dilated cardiomyopathy-related human failing hearts. 20,21 In falciparum malarial condition, the pGSN level decreases with disease severity and reverts back to normal level on treatment, which makes it an important biomarker candidate to examine disease progression and recovery. 13 Lee et al. have indicated a higher risk of death in critically ill surgical patients on dropping pGSN below 25% of normal value. 19 Also, in allogeneic hematopoietic stem cell transplantation, the drop in pGSN level was responsible for increased mortality and fatal complications like idiopathic pneumonia syndrome (IPS). 16 Although, Boukli et al. have indicated an upregulation of gelsolin in HIV-1-infected patients, the quantitative variation in relation to disease severity has not been reported. 25 The purview of this study is to propose pGSN as a biomarker candidate for HIV-1 infection. Our results indicate an increased pGSN level in HIV-1-infected patients, which shows an inverse variation with CD4 lymphocyte counts.
In case of HIV-1 infection, the entry of virus is facilitated by the interaction of viral envelop protein Env-gp120 with various receptors and coreceptors of target lymphocytes, its attachment, and pore formation. It has been reported that cellular form of gelsolin restricts HIV-1 infection of CD4 lymphocytes by severing of cortical actin and, therefore, limiting its reorganization for viral attachment and entry at the prefusion step. Also, GSN overexpression or silencing modulates receptor clustering of CD4-CXCR4 and CD4-CCR5 to one pole of cell, which is induced by viral proteins. 26 In HIV-1-infected and HIV-/HCV-coinfected patients, the gelsolin level has been shown to be upregulated. 25 The increased concentration of gelsolin may be induced by increased viral infection. Consistent with these observations, our results show a higher pGSN concentration in 213 HIV-1-infected patients compared to control healthy volunteers, but this only signifies the increased level of pGSN in HIV-1 infection, not the disease progression. Correlation of pGSN level with the CD4 lymphocyte count was important to understand its relationship with the severity of disease as CD4 cell count decreases with disease progression. Our results indicate a higher pGSN level in low CD4 cell count (<350 cells/mm3) patients and vice versa. Therefore, our result specifies a relationship of a higher pGSN with an increasing severity of HIV-1 infection.
Patients having HIV-1 infection are treated with ARV drugs. Therefore, it was interesting to observe the effect of ART on pGSN level. Starting with 105 nontreated (treatment-naive HIV-1-infected patients) and 108 ART patients, we observed higher pGSN concentration in treatment-naive HIV-1-infected patients. Our data of ART patients indicated a normalization of pGSN level toward control value. Also, in both the treatment-naive and ART groups, low CD4 cell count (<350 cells/mm3) patients have higher pGSN compared to high CD4 cell count (>350 cells/mm3) patients, showing consistency with severity in both the groups separately. Also, we report for the first time that upon ART, pGSN values lower toward normalcy before restoration of CD4 cell counts. Therefore, pGSN increases with severity and decreases as health improves.
Difference in the pGSN concentration by gender was evaluated, which illustrated no significant difference between male and female groups, and the values were similar to the observations made for critically ill patients. 19 The observation was consistent with treatment-naive and ART HIV-1-infected patients with high (>350 cells/mm3)/low (<350 cells/mm3) CD4 lymphocyte counts. Also, variance in the pGSN level was insignificant in different age groups of HIV-1-infected patients. The unbiased pGSN value with gender and age signifies its prospective of direct correlation with disease severity and treatment.
pGSN is a potential marker of health or injury recovery in various diseases. No condition is known where excess pGSN is present in circulation. Excess pGSN in body fluid is an imbalance created during pathogenic conditions. In HIV-1-infected patients, treatment with antiretroviral drugs is monitored by CD4 lymphocyte count. Our study of pGSN in relation to CD4 cell count indicates the significance of pGSN level in examining the severity and treatment. pGSN level normalcy could be an early indicator that ART is helping in recovery.
Footnotes
Acknowledgments
The authors acknowledge the help of Imran Khan, PhD student at NIPER, Hajipur, and Vijay at RMRIMS in blood collection and sample handling.
Author Disclosure Statement
No competing financial interests exist.