
Abstract
The molecular epidemiologic profile of HIV-1 in Suriname was determined through protease (PR) and reverse transcriptase (RT) sequences obtained from HIV-1 strains collected from 100 drug-naive HIV-1-infected persons. Subtype determination revealed that most viruses were of subtype B (94.9%) in both PR and RT genomic regions, followed by B/D recombinants (5.1%). Analysis of drug resistance mutations showed only one transmitted dug resistance mutation (TDRM) (V75M) in a single strain. The genetic data obtained can serve as a baseline for Suriname to monitor emerging mutations. This study reveals that the HIV-1 epidemic in Suriname is still characterized by a low TDRM rate (1%) and a low level of subtype diversity. However, both genes display a high genetic polymorphism. This high polymorphism may ultimately lead to drug resistance. Continuous monitoring of the baseline resistance is therefore a prerequisite to safeguard effective long-term treatment for people living with HIV-1 in Suriname.
Introduction
S
Treatment of HIV-1-infected patients in Suriname started on a very small scale in 1996, when it was confined to a specific subset of well-motivated individuals and was provided by a few specialists in internal medicine through gifts of antiretroviral (ARV) drugs from the Netherlands and the United States. With the establishment of a Revolving Fund in 2000, access to ARV treatment was broadened. National provision of ARV therapy free of charge started in 2005. The initiation and monitoring of treatment also shifted from secondary healthcare to primary healthcare in 2005. The number of HIV-1-infected patients receiving ARV therapy has thus dramatically increased since 2005, from 345 in 2005 to 1,428 in 2013. 2 The common first-line ARV regimens use a combination of two nucleoside and one nonnucleoside reverse transcriptase inhibitors (NRTIs and NNRTIs), all targeting the reverse transcriptase enzyme of HIV-1. In 2009, the national standard first-line treatment in Suriname consisted of the combination of Zidovudine (AZT), Lamivudine (3TC), and Nevirapine (NVP). Patients who fail this first line of treatment are switched to a protease inhibitor (PI)-based regimen with a backbone of NRTIs. Nevertheless, the number of different RTI and PI drugs currently available in Suriname remains limited.
The prevalence of transmitted drug resistance (TDR) is highly variable worldwide, with rates ranging from 0% to 25%. 3 The highest rates are reported in countries with a long-standing use of ARV drugs. The WHO distinguishes three groups of TDR prevalence: low (<5%), moderate (5%–15%), and high (>15%). 4 A systematic review of the literature showed that the rates of TDR in low- and middle-income countries increased between 2003 and 2010, reaching a peak of 6.6% in 2009. 5 Given that HIV-1 variants have not yet been described in Suriname and ARV treatment is started without prior genotypic testing due to resource limitations, knowledge of the polymorphism of HIV-1 protease (PR) and reverse transcriptase (RT), as well as mutations, whether or not associated with resistance, was critical. We therefore conducted a molecular study in a cohort of treatment-naive adult patients to investigate the level of natural polymorphism present in PR and RT genes, determine the subtype distribution, and identify potential drug resistance-associated mutations.
Materials and Methods
Between August and October 2009, a prospective cross-sectional study was conducted using plasma samples collected from 101 HIV-1-positive adults naive to ARV drugs. Participants included in this study were selected from the ambulatory care services of the four hospitals in the capital Paramaribo (Academisch Ziekenhuis Paramaribo, Diakonessen Ziekenhuis, Rooms Katholiek Ziekenhuis, and ‘s Lands Hospitaal) and the 10 largest healthcare centers of the Regional Health Services, which cater to the capital and surrounding areas. The study population consisted of ARV-naive adult HIV-1-positive persons living in Paramaribo and the surrounding areas with a CD4 count ≤385 (≤350 including a 10% range). This cutoff point was selected to include patients who were expected to start ARV treatment within 1 year. A minimum sample size of 70 was calculated with EPI Info (95% confidence level). For this calculation, the expected frequency of primary TDR in Suriname was set at 5%. This expected frequency was based on international figures, the relatively young epidemic, and the relatively short history of widespread use of ARV in Suriname. The genotyping was performed as an additional diagnostic test for the study participants. The study was approved by the Ministry of Health's National Ethics Committee.
Blood samples (2 × 5 ml) were drawn by venous puncture in EDTA tubes. Plasma was separated and stored at −80°C until RNA extraction for viral load (VL) measurement and genotyping. RNA was isolated from 1 ml of plasma with the Nuclisens® EasyMag® (BioMérieux, Marcy l'Etoile, France), as recommended by the manufacturer. The VL was determined using the bioMérieux NucliSENS EasyQ HIV-1 v1.2 kit. For genotyping, RNA was reverse transcribed to cDNA and amplified for partial RT and protease genes using the ANRS (Agence Nationale de Recherche sur le Sida) consensus sets of primers (
The PR and RT nucleotide sequences obtained were aligned using MEGA5 software with known group M reference sequences pooled from the HIV-1 database (
Results
One hundred one HIV-1-infected adult naive patients were recruited in Paramaribo. There were 55 women and 46 men. The mean age was 38 years (range, 18–62) for women and 39 (range, 23–58) for men. The VL ranged from 25 to 106 copies/ml. One patient was excluded for genotyping due to a VL below 100 copies/ml. Successful amplification was observed for 99 PR and 95 RT genes. Amplification of both genes could be obtained for 94 samples. Phylogenetic analyses together with the CPR tool showed that all RT sequences (n = 95) clustered with subtype B. All, but five PR sequences were subtype B (95%). The five non-B PR sequences were assigned to the D subtype.
PR and RT sequences were analyzed for polymorphisms, which were defined as any amino acid change compared to the B subtype consensus sequence HXB2 (Tables 1 and 2). Several major and minor mutations were detected. For PR, 82 of the 99 sequences (82.8%) analyzed harbored two or more mutations. Among them, 18% (n = 17/82) of the sequences harbored five to eight mutations. Alignment of the sequences showed that overall, at least one polymorphism had occurred at 38 of 99 (38.4%) amino acid positions (Table 1). In particular, V3 displayed a fixed mutation with 100% of sequences mutated, followed by the highly polymorphic L63, S37, V77, I15, R41, T12, and I72. Some of these polymorphic amino acid substitutions corresponded to positions of secondary resistance (in descending order: V77I, I15V, L63P, M36I, D60E, I62V, and H69K/Q/Y/R for those over 15% frequencies). Similarly, RT sequences exhibited polymorphic substitutions at 82 of 250 (32.8%) amino acid positions (Table 2). Substitutions found in more than 40% of the study subjects occurred at Q207, R211, E122, L214, S162, T200, V35, and I178. None of these positions corresponded to positions of drug resistance.
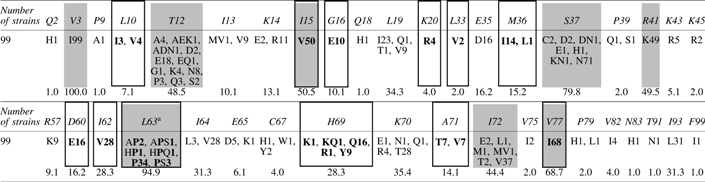
The gray boxes show polymorphic positions (>40%) and the boxed columns point to the positions of drug resistance mutations according to the French ANRS algorithm, v25 September 2015. Numbers after the mutated amino acid designation represent the number of strains with the respective substitution.
Additional substitutions at the L63 position: A1, C8, E1, H17, HQ1, IT1, K1, N3, Q4, R2, S11, and T2.

The gray boxes show polymorphic positions (>40%) and the boxed columns point to the positions of drug-resistance mutations according to the French ANRS algorithm, v25 September 2015. Numbers after the mutated amino acid designation represent the number of strains with the respective mutation.
Sequence analysis for the presence of DRMs in PR according to the French ANRS algorithm, version 25, revealed no major mutation conferring drug resistance. However, we detected one isolate carrying mutations L10V, G16E, M36I, D60E, and I62V, which confer a resistance to Atazanavir (ATV) and a possible resistance to Saquinavir (SQV) (Table 3). A second isolate was detected harboring substitutions L10LV, I15V, K20R, I62V, L63P, H69Q, A71V, and V77I, which together confer resistance to SQV and Lopinavir (LPV), and a possible resistance to ATV. A third isolate, carrying mutations L10I, I15V, M36I, I62V, and H69Q, implicated in resistance to SQV and a possible resistance to Tipranavir (TPV), also harbored the V179D mutation on RT (Table 3). Other combinations of minor amino acid mutations were detected, associated with possible resistance to SQV for 16 isolates, ATV for five isolates, TPV for two, and LPV for one isolate (Table 3). Finally, isolates carrying mutations associated with possible resistance to multiple drugs were identified, with SQV and ATV for two isolates, SQV and TPV for two, as well as LPV and ATV for one isolate (Table 3).
VL, viral load (log10 copies/mm3).
According to the French ANRS algorithm, version 25, September 2015. Major resistance mutations are in bold.
Resistance to ARV drugs is indicated in bold, possible resistance is in plain text.
ARV, antiretroviral; NRTI, nucleoside reverse transcriptase inhibitor; NNRTI, non-NRTI; PI, protease inhibitor; RT, reverse transcriptase.
With regard to the presence of DRMs in RT, one isolate out of 95 (1.05%) exhibited a major DRM (V75M), conferring resistance to the NRTI Stavudine (d4T) (Table 3). This isolate did not bear resistance mutations to NNRTIs and PIs. In addition, two isolates presented the V179D mutation that confers a possible resistance to Rilpivirine (RPV), while three others presented the V106I mutation that does not confer any resistance alone, nor a possible resistance, to NRTIs or NNRTIs.
According to the WHO list for surveillance of DRMs, the overall prevalence of TDR in Suriname was 1% with only one isolate bearing a DRM to the NRTI Stavudine.
Discussion
This study allowed us to document the circulating HIV-1 subtypes in Suriname and present the first published data on TDR in HIV-1-infected individuals in Suriname. The most prevalent HIV-1 clade observed in Suriname is subtype B (95%), the remainder being B/D intersubtype recombinants (5%). Predominance of subtype B is also observed in neighboring countries (Venezuela, French Guiana, and Northern Brazilian states) and in the Caribbean, even though its prevalence varies over a wide range across the different countries. 7 –12 These results are also comparable to the Netherlands. 13,14
A high level of polymorphism on both PR and RT genes was found in our population. Similar results were obtained in the region, where a high genetic diversity was observed in PR and RT genes in Venezuela, French Guiana, and Brazil. 9,10,15 Despite the high level of polymorphism on both PR and RT genes in our cohort, the genotypic drug resistance analysis uncovered only one drug resistance mutation for RT (V75M). The 1% level of transmitted HIV-1 drug resistance in Suriname is regarded as low according to the WHO classification. This is in line with recent results from French Guiana with a reported 4.6% prevalence of TDR, but in contrast with other countries in the region, given that the median overall TDR prevalence in Latin America and the Caribbean between 2000 and 2013 was 7.6%. 3,9
The absence of major drug resistance mutations is consistent with an ARV-naive population in a country where structural use of anti-HIV-1 drugs has been introduced relatively recently. These results can therefore serve as a baseline for Suriname. Since the detected V75M mutation confers resistance to Stavudine, which is only used in Suriname as an alternative drug in the first-line treatment for patients with anemia, these results become even more favorable. The practice of starting ARV treatment without prior genotypic testing is therefore not challenged in the current situation with limited resources and very low drug resistance. Nevertheless, the high degree of PR polymorphism at key amino acid positions known to be associated with drug resistance in HIV-1 subtype B is a concern for long-course PI treatment of people living with HIV-1. These results imply that PR and RT DRMs deserve monitoring to optimize first-line ARV regimens in Suriname.
Sequence Data
The GenBank accession numbers for the sequences are KX390878 to KX390977.
Footnotes
Acknowledgments
The study was funded by the Pan American Health Organization and the National AIDS Programme of Suriname. We acknowledge Dr. Stephen Vreden for his expert input and steering as a clinical researcher and clinician. We are obliged to Dr. Sigrid Ottevanger who comanaged this research. Furthermore, we owe thanks to the medical students, Ragni Chauti and Vikash Punwasi, who were involved in the data collection and data entry. We also thank the participating clinics and the directors and personnel of the laboratories of the Academic Hospital Paramaribo (Dr. John Codrington), Diakonessen Hospital (Mrs. Uselencia Esajas), and Central Laboratory (Mr. Merril Wongsokarijo).
Author Disclosure Statement
No competing financial interests exist.