
Abstract

O
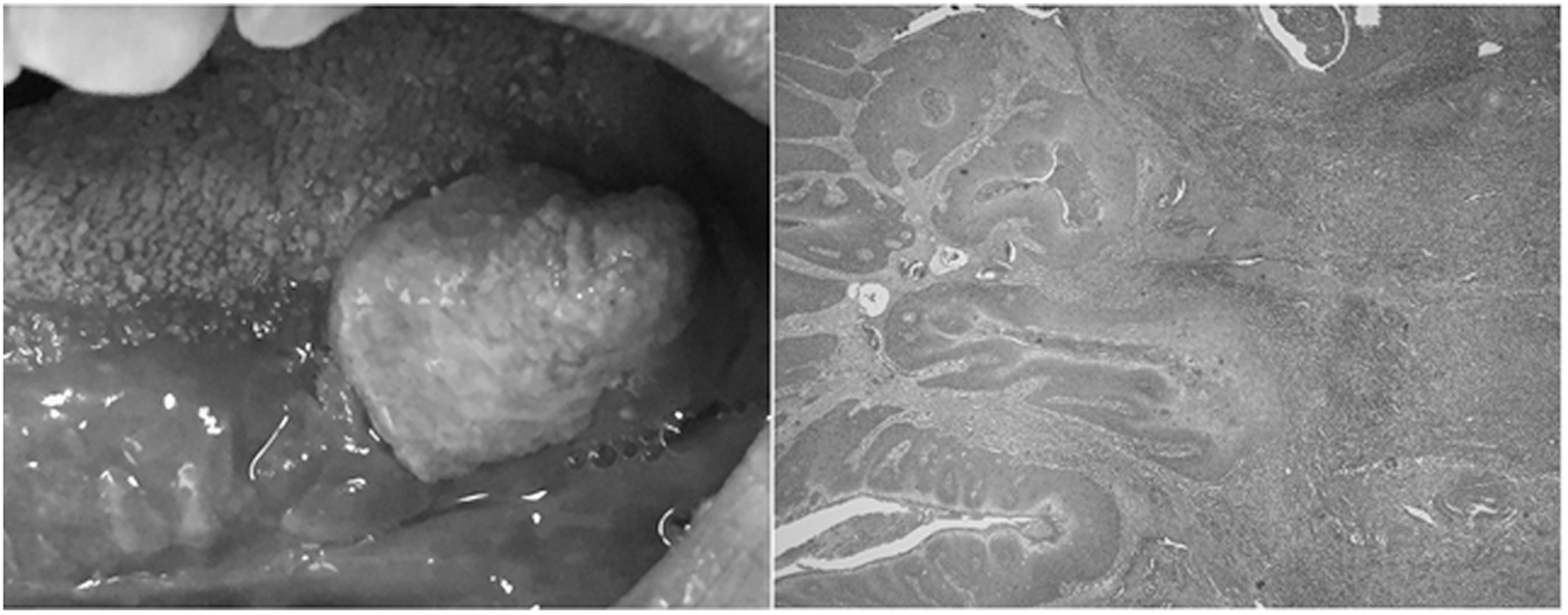
Subsequent head and neck magnetic resonance imaging showed a 20 × 12 × 15 mm mass infiltrating the genioglossus muscle without apparent lymphonodal involvement. A diagnosis of squamous cell carcinoma was formulated on biopsies of the lesion. Immunohistochemical expression of p16 antigen resulted positive for both cytoplasmatic and nuclear in neoplastic cells of the bioptic specimens, suggesting the presence of HPV infection. The patient underwent surgical excision of the neoplasia and the histological examination confirmed the presence of a low-intermediate grade, partially keratinizing, squamous cell carcinoma (Fig. 1B).
This case shows the clinical relevance of HPV-HIV coinfection, particularly in patients with other risk factors for oral squamous cell carcinoma, such as tobacco and alcohol consumption. The patient was on effective antiretroviral therapy with optimal control of HIV replication but with a low CD4/CD8 cell ratio; this scenario is known to be associated with an increased risk of serious non-AIDS events. 3
It is conceivable that although other risk factors may have contributed to initiation and progression of the neoplasm, HPV infection, given the immunohistochemical data, may be considered the prominent trigger.
Current data show the efficiency of HPV vaccination in preventing dysplasia and intraepithelial neoplasia even after HPV infection. 4 It is important to emphasize the relevance of correct sexual behaviors and communication about the risk of HPV infection along with HPV vaccination, especially for all HIV-infected patients, as a valuable tool to reduce HPV-related complications.
Footnotes
Author Disclosure Statement
No competing financial interests exist.