
Abstract
Achievement and maintenance of virologic suppression after cancer diagnosis have been associated with improved outcomes in HIV-infected patients, but few studies have analyzed the virologic and immunologic outcomes after a cancer diagnosis. All HIV-infected patients with a diagnosis of cancer between 2000 and 2011 in an urban clinic population in Baltimore, MD, were included for review. HIV-related outcomes (HIV-1 RNA viral load and CD4 cell count) were abstracted and compared for patients with non-AIDS-defining cancers (NADCs) and AIDS-defining cancers (ADCs). Four hundred twelve patients with baseline CD4 or HIV-1 RNA viral load data were analyzed. There were 122 (30%) diagnoses of ADCs and 290 (70%) NADCs. Patients with NADCs had a higher median age (54 years vs. 43 years, p < .0001) and a higher frequency of hepatitis C coinfection (52% vs. 36%, p = .002). The median baseline CD4 was lower for patients with ADCs (137 cells/mm3 vs. 314 cells/mm3) and patients with NADCs were more likely to be suppressed at cancer diagnosis (59% vs. 25%) (both p < .0001). The median CD4 for patients with NADCs was significantly higher than patients with ADCs at 6 and 12 months after diagnosis and higher at 18 and 24 months, but not significantly. Patients with an NADC had 2.19 times (95% CI 1.04–4.62) the adjusted odds of being suppressed at 12 months and 2.17 times the odds (95% CI 0.92–5.16) at 24 months compared to patients with an ADC diagnosis. For patients diagnosed with ADCs and NADCs in this urban clinic setting, both virologic suppression and immunologic recovery improved over time. Patients with NADCs had the highest odds of virologic suppression in the 2 years following cancer diagnosis.
Introduction
H
More recently, it has been recognized that HIV-infected patients are also at higher risk for so-called non-AIDS-defining cancers (NADCs). 6,7,12 –15 Such NADCs include cancers of the lung, liver, oral cavity, and anus, as well as Hodgkin lymphoma among others. These NADCs have been recognized as an important cause of non-AIDS-related morbidity and mortality in HIV-infected patients. 16 –19
Mortality due to cancer has been notably higher among HIV-infected patients with cancer compared to HIV-uninfected patients with cancer. 19 –23 However, there is little data regarding HIV-specific outcomes (i.e., CD4 count recovery and virologic suppression) after a cancer diagnosis as the focus on HIV treatment and control shifts toward cancer treatment and cure. Because HIV-infected patients have historically been excluded from cancer treatment protocols, optimal strategies for ART management during cancer treatment are unknown. In addition, concurrent use of ART with chemotherapy is fraught with challenges due to overlapping toxicities, drug–drug interactions, and the struggle to maintain daily oral ART during chemotherapy-induced nausea and vomiting. 24 Nevertheless, achievement and maintenance of virologic suppression after cancer diagnosis have been associated with improved outcomes, 25 particularly for HIV-associated lymphomas. 26,27 Therefore, further research is needed to determine the typical virologic and immunologic outcomes in HIV-infected patients after a cancer diagnosis and whether these outcomes differ by the type of cancer.
The objective of this study was to compare the virologic and immunologic outcomes between HIV-infected patients with NADCs and those with ADCs.
Materials and Methods
Study population
The University of Maryland Medical Center, Institute of Human Virology, Maryland General Hospital, and Baltimore Veteran's Affairs Medical Center provide comprehensive care to ∼4,000 HIV-infected patients per year. The University is also a tertiary-care referral center for patients diagnosed with cancer from around the state of Maryland and surrounding areas.
A retrospective cohort study was conducted to estimate the association between cancer type and viral suppression at annual time points following cancer diagnosis. Patients were eligible for inclusion in the study if they were HIV infected and had a cancer diagnosis between January 1, 2000 and December 31, 2011. HIV-infected patients with a cancer diagnosis (n = 565) were identified by searches of electronic clinic records for all cancer-related diagnostic billing codes (ICD-9). Cancer diagnoses were recorded after confirmation from histopathologic reports. When patients had more than one cancer diagnosed, only the first cancer was analyzed further. The cancer type was categorized as ADC or NADC. ADCs included Kaposi sarcoma, invasive cervical cancer, non-Hodgkin lymphomas (diffuse large B cell lymphoma, plasmablastic lymphoma, Burkitt lymphoma, primary central nervous system lymphoma, and primary effusion lymphoma). NADCs were all other cancers.
Data abstraction methods have been previously described. 25 HIV-specific data collected included HIV RNA viral load levels and CD4 cell counts. Due to differences in HIV-1 RNA assays used over time, HIV suppression was defined as an HIV-1 RNA of ≤400 copies/ml. The HIV RNA level and CD4 cell count at the time of cancer diagnosis were those values closest to the date of diagnosis within 6 months before and 3 months after the diagnosis. Patients who were missing both a CD4 cell count and viral load at the time of cancer diagnosis were excluded (n = 153). A sensitivity analysis was performed to assess whether patients who were excluded differed significantly from patients included in the study by baseline covariates.
Antiretroviral regimen usage was recorded by start and stop date along with the stated reason for change (if applicable). Patients were determined to be taking ART at baseline if they were taking ART at least 30 days before cancer diagnosis. ART regimens were considered “NNRTI based” or “PI based” if they included two or more NRTIs with either an non-nucleoside reverse transcriptase inhibitor (NNRTI) or protease inhibitor (PI), respectively. ART consisting of only nucleoside analogues, dual protease inhibitor-NNRTI combinations, and integrase inhibitor-based regimens was categorized as “other.” Institutional Review Boards at each site approved the protocol.
Statistical analysis
Data were first investigated using univariate analysis to describe the frequency and distribution of the outcome (viral suppression), primary exposure variable (cancer type), and covariates. The crude association between cancer type and viral suppression was initially investigated in bivariate analysis using a Pearson's chi-square test. The association between baseline characteristics of HIV patients by AIDS and non-AIDS defining cancers was initially investigated in bivariate analysis. Associations among categorical variables were compared using either a chi-square or Fisher's exact test and continuous variables were compared using a Wilcoxon rank sum test for equality of medians. Logistic regression was used for the inferential analysis to estimate the association between cancer type and viral suppression at 12 and 24 months. Baseline covariates investigated as potential confounders included age at cancer diagnosis, sex, race, primary risk factor for HIV infection, hepatitis B infection, hepatitis C infection, CD4 cell count at cancer diagnosis, and ART regimen at cancer diagnosis. Potential confounders were maintained in the adjusted model if they changed the beta estimate of the crude association for cancer type and viral suppression by more than 10% or if they significantly improved model fit. Mean CD4 cell count following cancer diagnosis was modeled using multivariable liner mixed models for repeated measures with an unstructured covariance matrix. The baseline covariates were retained in the final model if they confounded the relationship between cancer type and mean CD4 cell count in stratified analysis or if they significantly improved model fit, which was determined by a significant reduction in the Akaike information criterion. A sensitivity analysis was conducted to assess whether the exposure outcome relationship was similar comparing those included to those excluded from the analysis. All analyses were conducted using SAS version 9.4 (Cary, NC).
Results
Demographic characteristics of the 412 study subjects are shown in Table 1. The median age at the time of cancer diagnosis was 52 years. The majority of patients were male (80%) and African American (87%). The most common risk factor for HIV acquisition was injection drug use (IDU, 43%), and hepatitis C infection was common (48%). The median time from HIV diagnosis to cancer diagnosis was 9 years.
Three patients were missing a CD4 cell count at cancer diagnosis and 38 were missing a viral load at diagnosis.
p-Value from Wilcoxon rank sum test.
p-Value from Chi-Square test of proportions.
p-Value from Fisher's exact test.
Includes six patients on an integrase inhibitor.
ADC, AIDS-defining cancer; ART, antiretroviral therapy; IQR, interquartile range; NADC, non-AIDS-defining cancer; NNRTI, non-nucleoside reverse transcriptase inhibitor; VL, viral load.
The majority of the study sample had been diagnosed with an NADC (70%). The most frequent cancer among patients diagnosed with an ADC was non-Hodgkin lymphoma (N = 76), followed by Kaposi sarcoma (N = 37), unspecified lymphatic (N = 5), and invasive cervical cancer (N = 4). Among patients diagnosed with an NADC, lung cancer was the most frequent (N = 59), followed by prostate (N = 46), head and neck (N = 35), liver (N = 23), and Hodgkin lymphoma (N = 17). Patients with an ADC diagnosis were significantly younger, had a significantly lower median CD4 cell count at baseline, were less likely to be on ART, and were less likely to be virally suppressed at diagnosis compared to patients with an NADC diagnosis. The median time from HIV diagnosis to cancer diagnosis for patients with NADCs (11 years) was more than double that for patients with ADCs (5 years, p < .0001). A total of 189 (46%) patients did not reach the study endpoint of 2 years. The majority of the attrition was due to death (43%), and there was not a significant difference in the proportion of death comparing patients with an NADC to those with an ADC (40% vs. 44%, p = .45). Thirteen patients were lost to follow-up, eight in the ADC group (6%) and five in the NADC group (2%) (p = .03).
Patients who were excluded did not differ significantly from patients included in the final study by most baseline covariates (data not shown). The sensitivity analysis showed no differences in hepatitis B, time from HIV diagnosis, ART at the time of diagnosis, or race, but there were statistically significant differences in sex (20% of included subjects were females compared to 28% of excluded subjects), mode of transmission (43% of those included were IDU vs. 29% of those excluded), and hepatitis C (48% included in study vs. 32% excluded). The results of the sensitivity analysis, which included the patients excluded due to missing CD4 and viral load measures at baseline, to estimate the crude association between cancer type and viral suppression, yielded results consistent with the final findings of increased odds of viral suppression at 12 and 24 months among patients with an NADC compared to patients with an ADC (data not shown).
Immunologic outcomes
The median CD4 count at diagnosis for all patients was 268 (interquartile range 114–443). Figure 1 depicts the adjusted mean CD4 by ADC and NADC over time. The mean CD4 for NADCs was significantly higher than that for ADCs at baseline and at 6 months after cancer diagnosis (baseline, p < .0001, 6 months, p < .01). By 12 months after diagnosis, there was no evidence of a difference in mean CD4 for NADC and ADC patients after adjusting for sex, baseline CD4, ART, and both hepatitis B virus and hepatitis C virus coinfection (12 months, p = .11, 18 months, p = .51, and 24 months, p = .77).
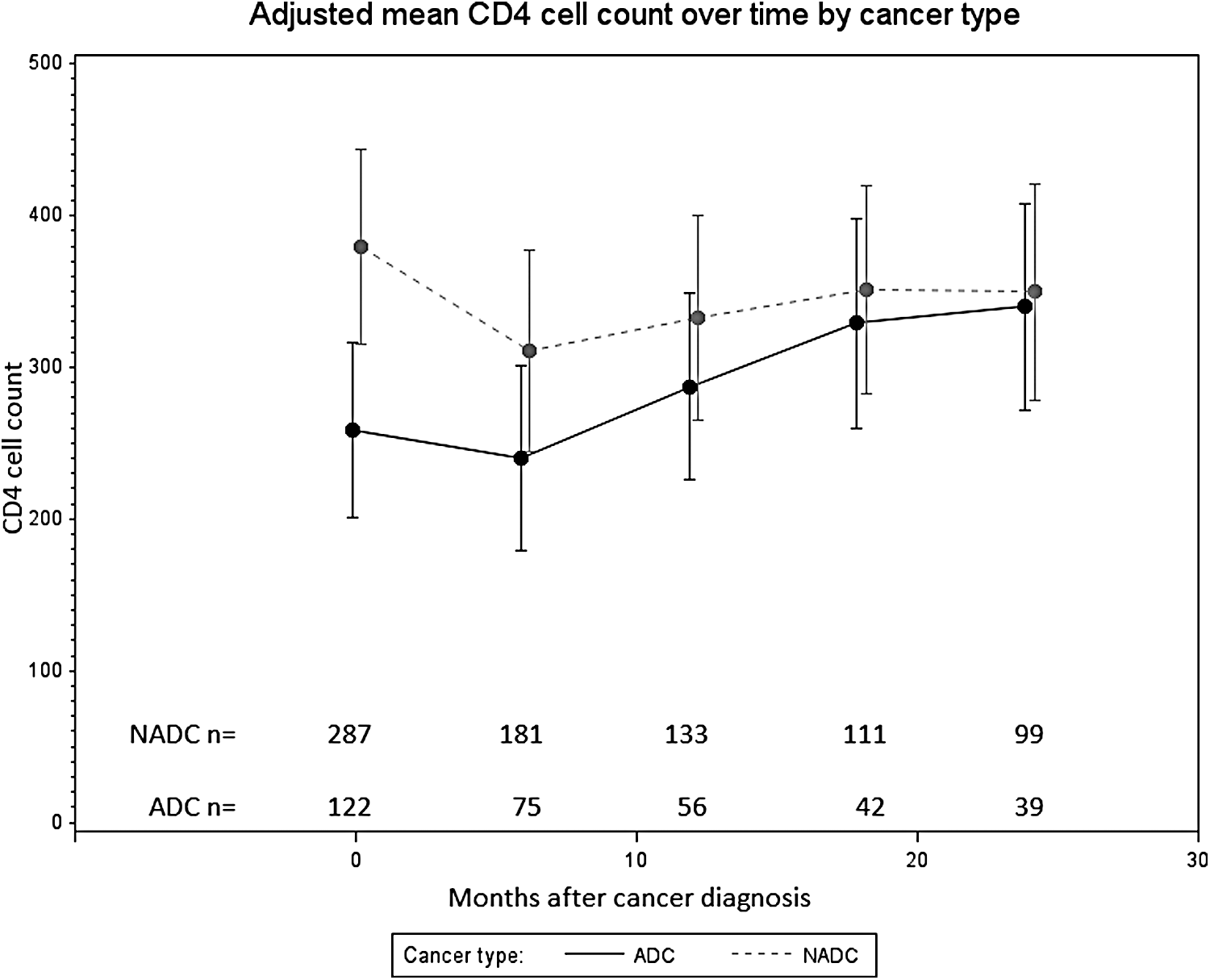
Mean CD4 cell counts adjusted for sex, baseline CD4 cell count, ART at cancer diagnosis, HCV coinfection, and HBV coinfection. ART, antiretroviral therapy; HCV, hepatitis C virus; HBV, hepatitis B virus.
Virologic outcomes
Approximately half (49%) of patients had a suppressed viral load at the time of cancer diagnosis, but a greater proportion of patients with NADCs were suppressed than those with ADCs (59% vs. 25%) (Fig. 2). Virologic suppression improved over time in ADC patients and averaged 60% from 12 to 24 months. In patients with NADCs, virologic suppression ranged from 70% to 80% between 6 and 24 months. Virologic suppression remained significantly different by the type of cancer; patients with ADCs were less likely than those with NADCs to be suppressed at each time interval from baseline to 24 months.
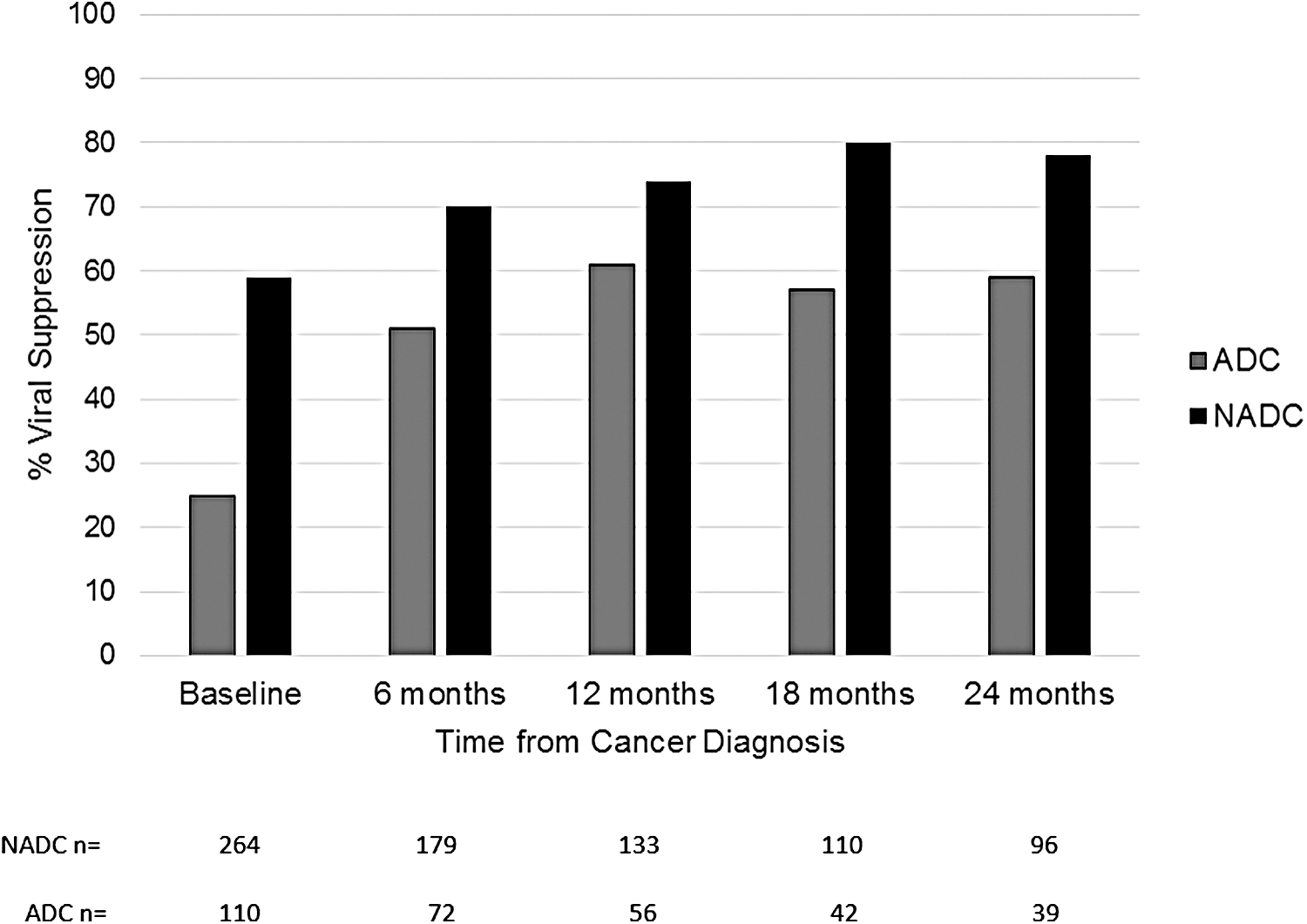
Proportion of cases with virologic suppression ≤400 copies/ml over time.
In the unadjusted analysis, patients with an NADC diagnosis had 1.81 times the odds (95% CI 0.94–3.51) of being suppressed at 12 months compared to patients with an ADC diagnosis (Table 2). After controlling for sex and primary HIV risk factor, patients with an NADC had 2.19 times the odds (95% CI 1.00–4.92) of being suppressed at 12 months compared to patients' with an ADC diagnosis.
aOR, adjusted odds ratio; CI, confidence interval; OR, odds ratio.
At 24 months, in the unadjusted analysis, patients with an NADC had 2.48 times the odds (95% CI 1.12–5.53) of being suppressed compared to patients with an ADC diagnosis. After controlling for race and primary HIV risk factor, the adjusted odds ratio was attenuated to 2.17 (95% CI 0.92–5.16) (Table 3).
Discussion
This study has several important findings. First, patients with NADCs were typically diagnosed with cancer while on ART, with high CD4 counts, and while virologically suppressed. Most patients then maintained virologic suppression in the 2 years following cancer diagnosis. Second, patients diagnosed with ADCs were largely not taking ART at baseline; the proportion of ADC patients with virologic suppression improved over time, yet a significant proportion (42%) remained unsuppressed even at 1 year after cancer diagnosis. Due to the potential impact of ongoing viremia on mortality after cancer diagnosis, this finding is concerning and may contribute to an increased likelihood of death in these dually affected patients.
This cohort represents the largest number of virologic outcomes after cancer diagnosis for patients with NADCs reported to date. At 12 and 24 months, viral suppression was nearly 80%, a figure that is comparable or better than rates of suppression in the general HIV population at a typical urban clinic today. 28 –30 One reason for this high suppression rate may be that, patients with NADCs are heavily engaged in their own medical care through frequent visits with their oncologic and HIV care team. In addition, high precancer viral suppression rates typical for patients diagnosed with NADCs 31 may be reflected in the high levels of engagement in care for this population. However, the fact that a significant proportion of patients (∼20%) were not suppressed indicates that additional strategies are needed to optimize HIV treatment after cancer diagnosis.
The adjusted association between cancer type and viral suppression at 12 months showed that the odds of being suppressed among NADC-diagnosed patients compared to ADC diagnosis was significantly higher. Others have reported variable rates of viral load (VL) suppression after a diagnosis of non-Hodgkin lymphoma (NHL), ranging from 55% at 1 year 32 to 69% at the end of chemotherapy. 33 Although the pathogenesis of HIV-related lymphoma is not fully known, circulating viremia has been associated with increased risk for lymphoma development 34,35 as well as increased mortality after NHL diagnosis. 26 The fact that less than 60% of patients with ADCs in this cohort were virologically suppressed at 12 and 24 months illustrates that new strategies may be needed to improve the virologic outcomes of these patients diagnosed with ADCs. As only 25% of patients with ADCs in this cohort were virologically suppressed at baseline, this group likely represents a subpopulation of patients who are not strongly engaged in care. Currently, there is no standard-of-care ART regimen for HIV-infected patients undergoing cancer treatment due to the historical exclusion of HIV-infected patients from oncology studies; further research is critical to determine the best ART regimens for such patients.
One limitation of this study was the reduction in sample size with increasing time since cancer diagnosis. It was not possible to compare individual cancer types due to the low number of CD4 and VL measures for each patient. Low rates of VL sampling in routine clinical practice for dually affected patients may suggest a lack of focus on HIV during cancer diagnosis and treatment or such patients have difficulty maintaining connection with their HIV provider during rigorous cancer treatment schedules. Given the possibility that HIV viremia after cancer treatment may be a risk factor for mortality, plus the multitude of drug–drug interactions between ART and cancer chemotherapeutic drugs, it is critical for oncologists to work closely with infectious disease colleagues to maximize treatment outcomes during acute cancer management.
This study had several additional limitations. Because the patients were drawn from an urban clinical cohort in Baltimore, the findings may not be generalizable to all HIV-infected patients in the United States. However, this population, which is largely an underserved minority population comprised predominantly of African Americans with a high proportion of IDU history and hepatitis C infection, is more reflective of the HIV epidemic in the United States, which is largely concentrated in urban areas. Second, due the retrospective design and clinical nature of the data, the study inferences are limited since VL measures were not taken at standard intervals and patients missing both a CD4 and viral load at baseline were excluded. These patients could be systematically different from those included (potential selection bias); however, patients excluded from the study had the same cancer type distribution as those included in the study, which would indicate that the missing baseline laboratory values for the outcome were not associated with the exposure of interest and if the association between cancer type and outcome is true, it would likely exist in those excluded as well. In addition, the results of our sensitivity analysis yielded quantitatively similar estimates of association. Finally, the number of patients alive and with available data at 24 months was small, limiting the conclusions that could be drawn about long-term follow-up. A noncancer comparison group was not available, and so temporal trends related to changes in ART patterns could not be assessed. Differences in ART utilization and efficacy may also have contributed to virologic and immunologic outcomes among the cohort.
In conclusion, patients diagnosed with NADCs in this urban clinic setting had high rates of virologic suppression at baseline that continued throughout the course of cancer treatment. Patients with NADCs had higher odds of virologic suppression in the 2 years following cancer diagnosis compared to patients with ADCs. Significant proportions of patients with both ADCs and NADCs remained unsuppressed after cancer diagnosis, indicating that new strategies are urgently needed for engaging and treating HIV-infected patients who are diagnosed with cancer.
Footnotes
Acknowledgments
At the time of the study, DJR was partially supported by a Paul Calabresi Clinical Oncology Training Program award (K12 CA126849); KAS was partially supported by the Building Interdisciplinary Research Careers in Women's Health (BIRCWH) program award (K12 HD43489-13). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the article. We would also like to thank Rotana Alsaggaf for reviewing the data.
Authors' Contributions
D.J.R. and R.R.R. conceived and designed the study; D.J.R. acquired the data; K.A.S. and A.V. analyzed the data; D.J.R., K.A.S., A.V., and R.R.R. interpreted the analysis; D.J.R. drafted the article; D.J.R., K.A.S., A.V., and R.R.R. contributed to revisions. All authors approved the final version of the article. D.J.R. had full access to all the data in the study and takes responsibility for the integrity of data and the accuracy of data analysis.
Author Disclosure Statement
No competing financial interests exist.