
Abstract
High levels of inflammatory cytokines in the genital tract suggest mucosal vulnerability and increased risk of HIV and sexually transmitted infection (STI) acquisition. Intravaginal douching is associated with bacterial vaginosis (BV) in women in the United States, and both douching and BV are linked to HIV and STI acquisition. This study evaluates inflammatory cytokines in the genital tract to increase understanding of the effects of both BV and intravaginal douching to the vaginal mucosa. A cross-sectional study of participants in the Miami WIHS investigated 72 reproductive age women (45 HIV+ and 27 high-risk HIV−) who completed intravaginal douching questionnaires and underwent collection of vaginal swabs and cervicovaginal lavages (CVLs). BV was assessed using the Nugent score. Inflammatory cytokines in the CVLs (interleukin [IL]-6, IL-8, IL-1α, IL-1β, soluble intracellular adhesion molecule-1 [sICAM-1], interferon [IFN]α2, chemokine C ligand 5 (CCL5), vascular endothelial growth factor (VEGF), monocyte chemotactic protein-1 (MCP1), tumor necrosis factor alpha (TNFα), and secretory leukocyte protease inhibitor [SLPI]) were measured. Fourteen (19%) women reported intravaginal douching; 24 (33%) had BV. BV, intravaginal douching, and HIV were associated with higher levels of inflammatory cytokines. After controlling for demographic and risk factors and HIV status, women who had BV and douched had higher levels of inflammatory cytokines than those without BV and who did not douche, or who only had BV or only douched. These findings suggest that BV and douching are associated with greater mucosal inflammation and may facilitate HIV acquisition and transmission. Although longitudinal studies are needed to determine temporal associations and causality, interventions to decrease rates of intravaginal douching and BV could significantly decrease women's risks of acquiring STIs and HIV and limit the spread of HIV.
Introduction
C
Bacterial vaginosis (BV), the most common FRT infection, is characterized by a decrease in the number of vaginal lactobacilli and an increase in the number of anaerobic gram-negative bacilli. 11,12 BV is associated with increased risk of obstetric and gynecological complications, STI and HIV acquisition, and HIV transmission to sexual partners and newborns. 13,14 BV occurs in about 30% of reproductive age women, and up to 84% of BV is asymptomatic. 15 Women with BV have higher levels of vaginal inflammatory cytokines and lower levels of SLPI than those without BV, and treatment for BV has been shown to decrease FRT inflammatory cytokines. 6,16 –20
Intravaginal cleansing is the practice of introducing substances inside the vagina for the purpose of hygiene, and the use of commercially available vaginal douches is common among women in the United States. 21 –23 Intravaginal cleansing is associated with a significant decrease in lactobacilli in the FRT, indicating the potential risk for the development of BV. 24 –27 In addition to promoting BV, intravaginal cleansing is associated with other obstetric and gynecological complications (pelvic inflammatory disease [PID] and ectopic pregnancy) 21,28 and although definitive evidence is not conclusive, intravaginal cleansing may increase the risk of HIV acquisition. 29 –32
The mechanism by which BV and intravaginal cleansing facilitate HIV acquisition is not well understood and is likely mediated by changes in the inflammatory milieu of the FRT with recruitment of HIV target cells. 33,34 The effect of introducing feminine hygiene products on the FRT inflammation has previously been evaluated in vitro, and it has been suggested that vaginal douches promote a proinflammatory environment in the presence of BV. 35 The in vitro study showed a cause–effect relationship between commercially available vaginal douches and increased levels of inflammatory cytokines. 35 A study determined that lime juice tampons but not douches caused a significant change in the levels of inflammatory cervicovaginal cytokines; however, this study was done in women at low risk of HIV and did not evaluate BV. 34 No research has evaluated FRT inflammation in vivo in women who engage in vaginal cleansing using commercially available douches, nor if the combination of cleansing and BV increases FRT inflammatory markers and places women at a higher risk than vaginal cleansing or BV alone.
This innovative study assesses the relative contribution of the use of vaginal douches and BV to changes in lower FRT mucosal inflammatory markers, to increase understanding of the damaging effects of vaginal cleansing on the vaginal mucosa. It was hypothesized that women engaging in vaginal douching who have BV will have higher levels of FRT inflammatory cytokines than those who do not engage in vaginal douching and do not have BV. Results have relevance to both women with HIV and those at risk of HIV infection.
Materials and Methods
Ethics statement
Before study-related procedures, recruitment, or data analysis, approval was obtained from the Institutional Review Board at the University of Miami Miller School of Medicine. Preceding enrollment and provision of informed consent, participants were provided detailed information on study aims and assured of the confidentiality of study records. Signed informed consent was obtained by the study coordinator from all participants before any study-related assessment.
Study procedures
The study utilized a cross-sectional design enrolling women with HIV or at risk for HIV infection, and it was conducted at the AIDS Clinical Research Unit (ACRU) and the Behavioral Research Unit at the University of Miami, FL. The study was undertaken in cooperation with the Miami Women and HIV Interagency Study (WIHS) and the Miami Center for AIDS Research (CFAR). As per WIHS design, HIV-infected and HIV-uninfected women were recruited on a 2:1 ratio, and within the WIHS, a subset of women were corecruited for the present study. HIV-uninfected women enrolled in the WIHS report at least one of the following risk factors in the prior year: injection drug use; diagnosis of an STI; unprotected intercourse with three or more men or protected with more than five men; or exchange of sex for drugs, money, or shelter. Eligibility criteria for participation were women 18 to 45 years of age and being sexually active in the 3 months previous to study enrollment. Pregnant women or women using contraceptive medications or intrauterine devices were excluded. The study coordinator conducted web-based assessment of demographic and sexual risk factors, medical history, and vaginal cleansing practices. On completion of the web-based assessment, genital samples were collected.
HIV testing
The OraQuick ADVANCE® Rapid HIV-1/2 Antibody Test was used to determine HIV status for women without documentation of HIV status. Positive results were followed by a confirmatory HIV western blot. Participants known to be infected with HIV before the study presented documentation of positive HIV status, such as HIV western blot results, medical records, or two laboratory results with detectable HIV viral loads greater than 1000 copies/ml, and had a rapid test performed as confirmation.
Genital sample collection
Vaginal samples were collected by first inserting a vaginal speculum and then collecting with a vaginal cotton swab the secretions in the vaginal wall. The vaginal swab was placed on a glass slide and Gram stained for Nugent scoring. Following collection, the cervical os was examined and mucous was cleaned off. Cervicovaginal lavage (CVL) was then collected after installing 10 ml of sterile saline into the vaginal and cervical areas avoiding the os, and letting it rest for 60 s. CVL samples were transported on ice to the laboratory for analysis within 2 h of collection. CVLs were spun down for 10 min at 1000 g at 4°C and supernatants aliquoted and stored at −80°C for cytokine analysis.
Demographics and sexual risk factors
The demographic questionnaire assessed participant's age, race and ethnicity, marital status, educational level, employment, yearly income, alcohol use in the prior month, number of partners, history of exchanging sex for money, use of male condoms, and whether they had sexual activity the week before enrollment.
Medical history
The medical history questionnaires assessed whether a medical provider had previously diagnosed participants with STI (gonorrhea, syphilis, chlamydia, herpes, and trichomoniasis), PID, BV, and candida vaginitis, and self-reported date of their last menstrual period.
Vaginal cleansing and use of vaginal douches
The intravaginal cleansing questionnaire assessed whether participants had used a commercially available intravaginal douche in the past month using dichotomous response options (“yes,” “no”). Vaginal douching was limited to the use of commercial available douches and did not include the use of other products for vaginal cleansing. In addition to commercial douches, other products used for intravaginal cleansing (water alone, soap with water, vinegar, and homemade douches) were also assessed. Responses were not mutually exclusive.
Bacterial vaginosis
BV was diagnosed by Gram staining techniques of slides with vaginal secretions at the University of Miami microbiology laboratories within 24 h of collection. Staff were trained on proper procedures before analyzing the slides by the chief microbiologist and the same trained technicians were used to read the slides. Unclear cases were reviewed and confirmed by a second technician and the laboratory chief once a consensus was reached. The slides were judged based on Nugent criteria. A Nugent score of 4 or greater was diagnosed as abnormal vaginal flora, while a Nugent score of 7 or above was classified as BV.
Lower FRT inflammatory cytokines
Multiplex measurement in CVL samples for cytokines, sICAM-1, and CCL5
A panel containing 13 inflammatory (IL-6, IL-8, IL-1α, interleukin 1 receptor antagonist [IL-1Rα], IL-1β, interferon [IFN]α2, IL-10, IL-17α, VEGF, IL-4, interferon gamma-induced protein 10 [IP-10], monocyte chemoattractant protein-1 [MCP1], and tumor necrosis alpha [TNFα]) cytokines was measured in CVL samples using a customized MILLIPLEX™ Cytokine Human Ultrasensitive magnetic bead panel (EMD Millipore, Billerica, MA). A separate panel was used for both sICAM-1 and CCL5 measurement as suggested by the manufacturer. Undiluted samples were incubated overnight with cytokine-specific beads at 4°C with shaking. After washing, biotinylated detection antibodies and streptavidin-phycoerythrin were subsequently added. The beads were washed and acquired on a MAGPIX instrument (Luminex Corporation, Austin, TX). Median fluorescent intensity data were collected and analyzed with MILLIPLEX Analyst Software (EMD Millipore) and results were expressed as pg/ml. The lowest detection limit of standard curve for all analytes, except CCL5, was 3.2 pg/ml; for CCL5, the limit of standard curve was 2.44 pg/ml. Results for IL-10, IL-4, IL-17α, IP10, and IL-1Rα were not used for the analysis, given that most (∼80%) participants' values were below the detection cutoffs.
Measurement of SLPI levels in CVL
SLPI levels were measured in diluted samples by ELISA (Bio-Techne, Minneapolis, MN) with a sensitivity of detection of 25 pg/ml. Samples were tested using dilution ranges from 1:50, 1:100, to 1:300 to measure the actual SLPI levels in samples. Results were expressed as ng/ml.
Statistical analyses
Descriptive statistics were used to analyze demographic and medical history variables. Univariable Poisson models predicting cytokines were used to test for differences between BV, vaginal douching, HIV status, condom use, and race, and associations between cytokines and days since last menstruation, age, and frequency of sexual encounters. Vaginal douching was defined as having used commercial vaginal douches in the past month. Although other vaginal cleansing practices were assessed, due to collinearity, only vaginal douching with commercially available douches was included in the analysis as this practice is the most closely associated with the development of BV in the United States and products included in vaginal douches have previously shown a potential detrimental effect on the vaginal mucosa in the presence of BV. 35 We chose not to combine different cleansing practices because all participants engaged in at least one type of cleansing practice, and thus would have resulted in zero-cells and hindered statistical analysis. For values below or above the detection limits, the natural log of the value calculated from the division of the cutoff value by the square root of 2 was used. All models were built using PROC GLIMMIX with a log link and back-transformed medians and standard errors. Then, using the same analytic procedure, multivariable Poisson models were built with BV, vaginal douching, HIV status, condom use, race, days since last menstruation, age, and frequency of sex in the past month as predictors. Last, an interaction of BV and vaginal douching was tested for all cytokines, if both predictors were significant at p < .10 in multivariable models, also using a Poisson regression model with interaction. To follow-up significant interaction effects, medians were plotted and all possible six pairwise comparisons were tested for significance. Statistical Analysis System (SAS) v9.4 for Windows was used for all analyses.
Results
Demographics, medical history, douching history, and Nugent score (Table 1)
Participants were 72 women with a mean age of 34.17 (SD = 7.30). Three-fourths (76%) of the women were black and participants were primarily (64%) non-Hispanic. Nearly half (48%) of the women were in an unstable partnership. Most women had completed high school or less (72%), were unemployed (77%), and had a yearly household income of less than 1,200 (73%). On average, participants had 11 partners in the past 5 years (SD = 21.29), and almost two-fifths (38.0%) of the women reported having exchanged sex for compensation in the past. Only half (50.0%) reported consistent condom use in the past month, and an average of 5 (SD = 7.17) sexual encounters were reported in the past month. The median number of days from menstruation was 14 days (SD = 6.9).
Bold numbers indicate significant p value <0.05.
BV, bacterial vaginosis; PID, pelvic inflammatory disease.
Many of the participants reported a prior STI. Nearly one-fifth (19.4%) of participants reported having a history of gonorrhea, and 18% of syphilis, 31% of chlamydia, 8% of PID, 10% of herpes, 26% of trichomoniasis, 19% of BV, and 47% of candida vaginitis. Further details of demographic characteristics and medical history are reported in Table 1.
About two-thirds of women were infected with HIV (45% or 63%). All women reported at least one type of intravaginal cleansing practice. Twenty-seven (37%) women reported the use of water, 22 (31%) used soap with water, 10 (14%) used vinegar, and 8 (11%) used homemade douches made with soap or vinegar. Douching with a commercially available douche in the prior month was reported by 14 women (19%).
More than two-thirds of the sample (48 women) had Nugent scores consistent with abnormal vaginal flora (Nugent score = 4–6), and one-third (24) had a BV Nugent score (Nugent score ≥7). None had a normal Nugent score of 0–3, which is not unexpected in a population at high risk for HIV.
The demographic and risk factors, medical history, douching history, and BV are shown in Table 1.
Associations of lower FRT soluble inflammatory markers (IL-6, IL-8, IL1α, IL1β, SLPI, sICAM-1, IFNα2, CCL5, VEGF, MCP1, and TNFα) by demographic and risk factors, date from menstrual period, use of vaginal douches, BV, and HIV status
In bivariate analyses and multivariable analysis (using age, race, condom use, frequency of sexual encounters, days since last menstruation, vaginal douching, HIV status, and BV as predictors), most inflammatory cytokines were higher in younger women, women of white race, those who reported consistent condom use, had higher number of sexual encounters, shorter time from menstruation, used vaginal douches, had HIV infection, or had BV. Table 2 presents the unadjusted and adjusted models.
Adjusted means (for categorical variables) or exponentiated coefficients/estimates (for continuous variables) are presented.
Bold numbers indicate significant p value <0.05.
Multivariable Poisson regression models included age (continuous), race, condom use, frequency of sexual encounters (continuous), days since last menstruation (continuous), vaginal douching, HIV status, and BV as predictors.
Unit: picograms per milliliter (pg/ml).
CCL5, chemokine C ligand 5; IL, interleukin; IFN, interferon; MCP1, monocyte chemotactic protein-1; sICAM-1, soluble intracellular adhesion molecule-1; SLPI, secretory leukocyte protease inhibitor; TNFα, tumor necrosis factor alpha; VEGF, vascular endothelial growth factor.
Inflammatory cytokines in women with BV and engaging in vaginal douches
Following multivariable models, interactions of BV and vaginal douching were tested for all cytokines (IL-6, IL-8, IL-1α, IL-1β, SLPI, sICAM, IFNα2, CCL5, VEGF, MCP1, and TNFα), controlling for HIV status. Significant interaction effects between commercial douching and BV were found for IL-8, IL1α, IL1β, SLPI, IFNα2, sICAM, CCL5, VEGF, MCP1, and TNFα. Interactions were plotted and are presented in Figure 1, along with their respective follow-up pairwise comparisons. That is, although levels of inflammatory cytokines were different depending on whether the woman had BV, this varied as a function of whether the woman used vaginal douches, such that levels of mediators of inflammation were highest in women who had BV and douched when compared to women who did not have BV and did not douche, douched and did not have BV, and had BV and did not douche. All interactions were tested, including HIV status, condom use, race, days since last menstruation, age, and frequency of sexual encounters as controls. Analysis to assess the relationship of inflammatory cytokines in women with BV engaging in intravaginal cleansing other than commercial douches was conducted and no significant associations were found.
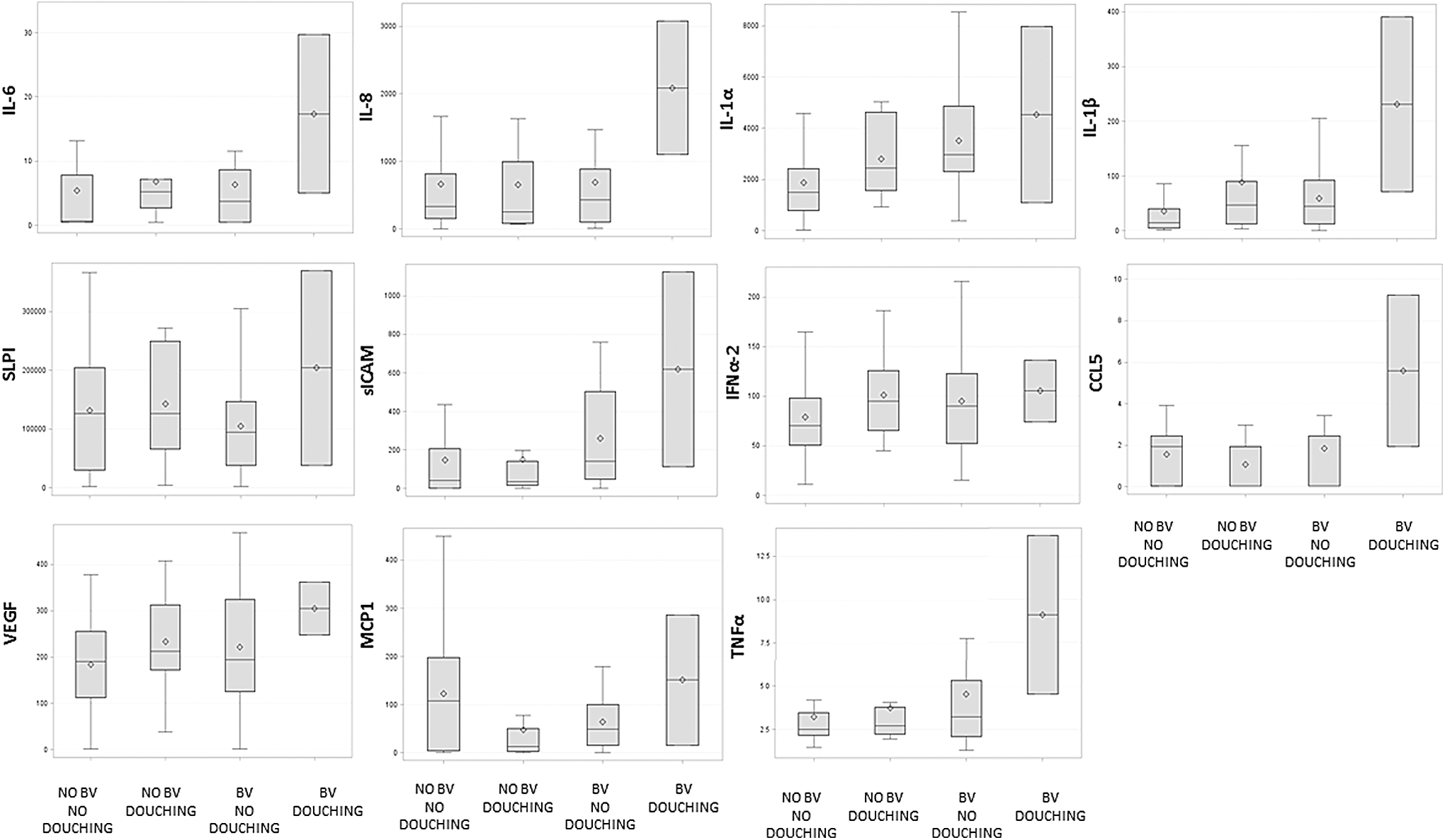
Inflammatory cytokines (pg/ml) in women engaging in vaginal douching with and without BV. Box plots report minimum, first interquartile range, median, third interquartile range, and maximum values; the mean is identified by open squares. IL-6: Levels of IL-6 were not significantly different between groups. IL-8: No BV and no douching was significantly different from no BV and douching and BV and douching; no BV and douching was significantly different from BV and no douching and BV and douching; BV and no douching was significantly different than BV and douching (all p < .01). IL-1α, IL-1β, SLPI, MCP1: All groups were significantly different from each other (all p < .05). sICAM-1: No BV and no douching was significantly different from no BV and douching, BV and no douching, and BV and douching; no BV and douching was significantly different from BV and no douching, and BV and douching; BV and no douching was significantly different than BV and douching (all p < .01). IFNα2: No BV and no douching was significantly different from no BV and douching, and BV and no douching (p < .05); no BV and douching was significantly different than BV and no douching. CCL5: No BV and douching was significantly different than BV and no douching and BV and douching (p < .05). VEGF: No BV and no douching was significantly different from no BV and douching, BV and no douching, and BV and douching; no BV and douching was significantly different from BV and douching; BV and no douching was significantly different than BV and douching, and BV and douching (all p < .01). TNFα: No BV and no douching was significantly different than BV and no douching, and BV and douching (p < .01); no BV and douching was significantly different than BV and douching (p < .05). All models controlled for age (continuous), race, condom use, frequency of sexual encounters (continuous), days since last menstruation (continuous), vaginal douching, HIV status, and BV. BV, bacterial vaginosis; CCL5, chemokine C ligand 5; IFN, interferon; MCP1, monocyte chemotactic protein-1; sICAM-1, soluble intracellular adhesion molecule-1; SLPI, secretory leukocyte protease inhibitor; TNFα, tumor necrosis factor alpha; VEGF, vascular endothelial growth factor.
Discussion
This study examined the levels of inflammatory cytokines in the FRT of women with HIV or at risk for HIV infection, and the relative contribution of the use of commercial vaginal douches and BV to distal FRT inflammation. Results indicated that most genital tract inflammatory cytokines were higher in younger women, women of white race, those who reported consistent condom use, had higher number of sexual encounters, shorter time from menstruation, used vaginal douches, had HIV infection, or had BV. In addition, distal FRT inflammation was increased in women who used vaginal douches and had BV when compared to those who did not use vaginal douches and/or did not have BV, regardless of demographic and risk factors and HIV status.
In the United States, the use of commercially available vaginal douches for vaginal cleansing has previously been identified as one of the main risk factors for developing BV, and BV has been associated with HIV acquisition. 14,36,37 In addition to HIV, BV has also been associated with STI acquisition, HIV transmission to sexual partners and newborns, preterm delivery, and spontaneous abortions. 38 Therefore, both vaginal cleansing and BV are important contributors to poor women's health outcomes and risk of STI and HIV acquisition. 21,28,39
The mechanism by which vaginal cleansing and BV increase the risk of HIV acquisition is not well understood, as it is not clear if the risk of using vaginal douches is independent or mediated by BV. It has been postulated that vaginal douches promote a change in the vaginal flora facilitating BV and an increase in the FRT inflammatory milieu with the associated release of inflammatory cytokines. Such an inflammatory milieu favors recruitment and activation of HIV host cells, the expression of HIV receptors, and tissue damage, all increasing mucosal vulnerability to HIV during vaginal intercourse. 35
The increase of inflammatory cytokines in the FRT in women with BV and in HIV-infected women has previously been described. 6,9,19 However, this is the first study to include the effect of vaginal cleansing with commercial douches as a potential contributor to FRT inflammation. Higher levels of cytokines identified in women who both engage in vaginal douching and have BV suggest that the combination of both factors impacts markers of inflammation in a greater magnitude than BV alone, causing the highest damage to the FRT mucosa and the highest potential for HIV acquisition.
In interpreting study findings, some limitations must be discussed: (1) the study's small sample size limits the generalizability of the results; (2) BV was assessed by using Nugent criteria and more sophisticated culture or microbiome analysis could have differentiated more microbial factors associated with inflammation in women who douche; (3) the results only apply to vaginal douching using commercial products and cannot be generalized to other vaginal cleansing practices or combination of similar practices; (4) our study did not have the power to detect differences related to levels of endogenous or exogenous sex steroid hormones and we did not determine the phase of the menstrual cycle. We, however, included the number of days from the last menstruation as a control variable; and (5) because of the cross-sectional and noninterventional nature of our study, we are limited on inferring causality based on associations. Longitudinal studies with a larger sample size and frequent assessments are needed to account for hormonal variations associated with menstrual cycles, and to establish a baseline level of cytokines and changes in cytokines over time. In addition, women who are not at risk for HIV should be included in future studies as controls.
Public health efforts should be undertaken to inform women of the potential damaging effects of douching on the vaginal mucosal surface and the risks associated with vaginal douches as well as other intravaginal cleansing practices, including the risk of HIV acquisition. Both BV and vaginal douching are difficult to influence; BV is often asymptomatic and screening for asymptomatic BV has not shown to be beneficial in the general population, and douching is a common behavior among women. 15,36 This study provides further evidence to support continued research evaluating interventions to decrease the use of vaginal douches and BV in both HIV-infected and HIV-uninfected women, as such interventions could be of relevance in women's health programs, especially in those that focus on STI and HIV prevention.
Footnotes
Acknowledgments
This study was funded by the National Institutes of Health, the Miami Center for AIDS Research (CFAR) at the University of Miami Miller School of Medicine [P30AI073961], Miami Women's Interagency HIV Infection Study (WIHS) [U01AI103397], and the Eunice Kennedy Shriver National Institute of Child Health and Human Development [K23HD074489]. The WIHS is funded primarily by the National Institute of Allergy and Infectious Diseases (NIAID), with additional cofunding from the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD), the National Cancer Institute (NCI), the National Institute on Drug Abuse (NIDA), and the National Institute on Mental Health (NIMH). Targeted supplemental funding for specific projects is also provided by the National Institute of Dental and Craniofacial Research (NIDCR), the National Institute on Alcohol Abuse and Alcoholism (NIAAA), the National Institute on Deafness and other Communication Disorders (NIDCD), and the NIH Office of Research on Women's Health. WIHS data collection is also supported by UL1-TR000004 (UCSF CTSA) and UL1-TR000454 (Atlanta CTSA).
Disclaimer
Data in this article were collected by the Women's Interagency HIV Study (WIHS). The contents of this publication are solely the responsibility of the authors and do not represent the official views of the National Institutes of Health (NIH). WIHS (Principal Investigators): UAB-MS WIHS (Michael Saag, Mirjam-Colette Kempf, and Deborah Konkle-Parker), U01-AI-103401; Atlanta WIHS (Ighovwerha Ofotokun and Gina Wingood), U01-AI-103408; Bronx WIHS (Kathryn Anastos), U01-AI-035004; Brooklyn WIHS (Howard Minkoff and Deborah Gustafson), U01-AI-031834; Chicago WIHS (Mardge Cohen and Audrey French), U01-AI-034993; Metropolitan Washington WIHS (Mary Young), U01-AI-034994; Miami WIHS (Margaret Fischl and Lisa Metsch), U01-AI-103397; UNC WIHS (Adaora Adimora), U01-AI-103390; Connie Wofsy Women's HIV Study, Northern California (Ruth Greenblatt, Bradley Aouizerat, and Phyllis Tien), U01-AI-034989; WIHS Data Management and Analysis Center (Stephen Gange and Elizabeth Golub), U01-AI-042590; Southern California WIHS (Alexandra Levine and Marek Nowicki), U01-HD-032632 (WIHS I–WIHS IV).
Authors' Contributions
All authors have seen and approved the content of this article, have contributed significantly to the work, and declare no conflict of interest. No writing assistance was sought in preparing this manuscript. M.L.A., S.P., S.P., D.L.J., and M.A.F. contributed to the conception and design of the work. M.L.A. and V.J.R. contributed to the acquisition of the data. S.P., M.R., and O.M. contributed performing laboratory analysis. M.L.A., V.J.R., and K.A. contributed to the analysis and interpretation of the data. R.N.F. contributed with advice on interpretation of the cytokine analyses. M.L.A., R.N.F., S.P., D.L.J., S.P., and M.A.F. drafted the manuscript and revised it critically for important intellectual content. All authors have contributed to the final version of this manuscript.
Author Disclosure Statement
No competing financial interests exist.