
Abstract
Changes in retrovirus acquisition/transmission behaviors have been reported in Brazil, with a concerning increase in HIV-1-infected individuals aged 15–39 years. In São Paulo, HIV-1/HTLV-1 and HIV-1/HTLV-2 coinfections have been associated with intravenous drug use and failure to detect HTLV-1/2 (human T cell lymphotropic virus types 1 and 2) with immunosuppression and the use of highly active antiretroviral therapy (HAART). Negative results for HTLV serologic [western blotting (WB)] and molecular [real-time PCR pol (qPCR)] confirmatory assays have been reported, whereas the best sensitivity has been found for INNO-LIA (LIA). In this study, we expand our previous data by analyzing a group of young patients (n = 1,383; median age 35.6 years) who recently acquired HIV by sexual contact, the majority of whom were HAART naïve, and comparing the performances of four HTLV confirmatory assays: LIA, WB, qPCR, and PCR-RFLP (tax). We confirmed HTLV infection in 58 (4.2%) blood samples: 29 HTLV-1, 24 HTLV-2, 1 HTLV-1+HTLV-2, and 4 HTLV. LIA, WB, qPCR, and PCR-RFLP sensitivities were 94.8%, 82.8%, 79.2%, and 74.5%, respectively. Associations of HTLV infection with female gender (OR = 2.28, 1.31–4.00) and age >40 years (p < .0001) were detected. The results confirm the low sensitivities of molecular assays and the best performance of LIA in detecting HTLV-1/2 in such patients. We hypothesize that the negative PCR results are due to the presence of defective provirus and/or low proviral load circulating in such patients, with inconclusive WB coinciding with the seroconversion period. Corroborating the associations obtained, repeated exposure is required for HTLV sexual transmission/acquisition, which is more efficient from male to female.
H
In Brazil, an estimated 2.5 million people are infected with HTLVs. Currently, the major routes of transmission are (i) sexual transmission due to unprotected intercourse, multiple partners, intercourse with an intravenous drug user (IDU), partners from HTLV-endemic areas, and a history of sexually transmitted disease and (ii) vertical transmission from mother to child through breast-feeding. 2 In contrast, the parenteral route of HTLV transmission through blood transfusion or sharing of contaminated needles has decreased in Brazil since HTLV serology became mandatory in blood banks (1993) and the implementation of several government-supported harm reduction projects that provide IDUs with sterile needles and syringes. Of note, these initiatives have considerably reduced the number of HIV-1 and HIV-HTLV coinfections occurring by this transmission route in Brazil. 1 –3
Although HIV-1, HTLV-1, and HTLV-2 share transmission routes and HIV/HTLV coinfection can occur, the outcomes differ. For instance, HIV-1/HTLV-1 has been associated with fast progression to AIDS, but HIV-1/HTLV-2 with slow progression. 4,5 Thus, correct diagnosis of HTLV-1 and HTLV-2 is important for appropriate patient follow-up.
Since the 1990s, the Instituto Adolfo Lutz, a Public Health Laboratory in São Paulo, Brazil, has performed studies on HIV/HTLV coinfection, detecting problems in diagnosis, mostly regarding HTLV-2 in HIV/AIDS patients. 6 –8 Indeed, the laboratory confirmed the presence of HTLV-1 and HTLV-2 in HIV/AIDS patients from São Paulo, with a high degree of inconclusive results for HTLV infection in these individuals. 9 Problems with the kits employed for screening and confirmatory assays were detected, 6 –10 and the application of molecular assays for diagnosis was suggested. 8,11 However, highly active antiretroviral therapy (HAART) in HIV/AIDS patients could affect detection of both HIV and HTLV, reducing the sensitivity of molecular assays for diagnosis. 3,12
In 2015, we reported a prevalence of 3.1% (1.7% for HTLV-1, 1.3% for HTLV-2, and 0.1% for HTLV) in 1,608 individuals (1,237 males, 371 females; median age 44.3 years) attending a pioneer AIDS Reference Center in São Paulo, with associations with female gender, IDU, and age >40 years (median age 49.5 years) (Group A). 3 In this cohort, low sensitivity of the real-time PCR pol (qPCR) confirmatory assay was detected (60%) in relation with the use of HAART. 3
Due to the current changes in the epidemiologic characteristics of HIV-1 and HTLV-infected individuals in São Paulo, we decided to expand our data on HIV/HTLV coinfection. In this study, we report HTLV-1/2 detection in a group of younger individuals recently acquiring HIV-1, mostly through sexual contact, and not undergoing HAART.
Blood samples sent to Instituto Adolfo Lutz for HTLV-1/2 diagnosis during the period of 2012 to 2015 were selected. We first considered the local attendance of patients (the most recent HIV/AIDS services setting in São Paulo) and then data obtained from medical records and from the Ministry of Health of Brazil through net information systems that control new HIV/AIDS cases and results for CD4+ cells and HIV-1 viral load. The study was approved by the Ethics Committee of Instituto Adolfo Lutz under protocol number 106D/2012.
Blood samples from 1,383 individuals (930 males, 453 females; median age 35.6 years) (Group B) were analyzed for the presence of HTLV-1 and HTLV-2. Briefly, blood was separated into plasma and peripheral blood leukocytes (PBLs). The plasma was screened for the presence of HTLV-1/2-specific antibodies using two enzyme immunoassays, Murex HTLV-I+II (Diasorin S.p.A, Dartford, United Kingdom) and Gold ELISA HTLV-I+II (REM, São Paulo, SP, Brazil). Reactive samples were confirmed by western blotting and line immunoassays [HTLV Blot 2.4 (WB); MP Biomedicals, Solon, OH, and INNO-LIA HTLV-I/II (LIA); Fujirebio, Europe N.V., Belgium]. All serological assays were performed and the result criteria interpreted according to the manufacturers' instructions. PBLs from all patients exhibiting positive reactivity in the screening assays were analyzed for the presence of HTLV-1/2 proviral DNA using in-house qPCR, as described. 11 Restriction fragment length polymorphism (RFLP) analysis of the amplification products of tax nested PCR using TaqI endonuclease, the cleavage site for which is present in HTLV-2 and absent in HTLV-1, was also applied. 13
Based on serological screening, 76 serum samples were reactive; all of them as well as the corresponding PBLs were tested by confirmatory assays. Considering true HTLV infection according to the result of any of the confirmatory assays, with more than 70% of samples confirmed as infection in three assays, but only 6.5% in one assay (data not shown), HTLV infection was confirmed in 58 (4.2%) blood samples: 29 HTLV-1, 24 HTLV-2, 1 HTLV-1+HTLV-2, and 4 HTLV. Results for nine samples were indeterminate. The sensitivities of LIA, WB, qPCR, and PCR-RFLP were 94.8%, 82.8%, 79.2%, and 74.5%, respectively. These results confirm that none of the confirmatory assays shows 100% sensitivity for detecting HTLV-1 and HTLV-2 in HIV-1-infected patients. Failure of molecular assays limits their use as a unique confirmatory assay in such individuals. Interestingly, the negative PCR results in Group B could not be attributed to HAART as the majority of patients were treatment naïve (data not shown). Thus, we hypothesize a very low HTLV viral load with transmission by sexual contact and/or the presence of defective HTLV-1 and HTLV-2 provirus circulating in these patients. Corroborating these hypotheses, repeated exposure is required for HTLV sexual transmission, and low proviral load (PVL) is reported in individuals acquiring HTLV through sexual routes. 2 In addition, mutations in LTR and tax segments of HTLV-1 have been implicated in low PVL and inconclusive WB results. 14
Compared with WB, the best sensitivity was observed for LIA in Group B (94.8% vs. 82.8%), corroborating the data obtained for Group A 3 and highlighting LIA as the choice for detecting HTLV-1 and HTLV-2. The indeterminate WB results could be related to the period of seroconversion as the WB profile indicated reactivity mostly with envelope proteins (Table 1), which are known to be the first antibodies to appear during seroconversion, 9 and in patients who are HTLV positive according to molecular assays. 14
Results obtained by WB (HTLV Blot 2.4; MP Biomedicals, Solon, OH) and immuno line assay (INNO-LIA HTLV-I/II; Fujirebio, Europe N.V., Belgium) according to manufacturers' criteria.
Results by in-house molecular assays: real-time PCR pol (qPCR) and restriction fragment length polymorphism analysis of amplification products of the tax nested PCR (PCR-RFLP) as previously described. 11
Ct, cycle threshold value; HTLV, human T cell lymphotropic virus; ND, not done; Neg., negative; WB, western blotting.
As in our previous data, associations of HTLV infection with female gender (OR = 2.28, 1.31–4.00) and age >40 years (median age 43.5 years) were detected in Group B, although the age of the patients differed significantly from that of the Group A patients (Fig. 1). No difference in HTLV prevalence between Groups A and B was detected (3.1% vs. 4.2%, p = 0.113).
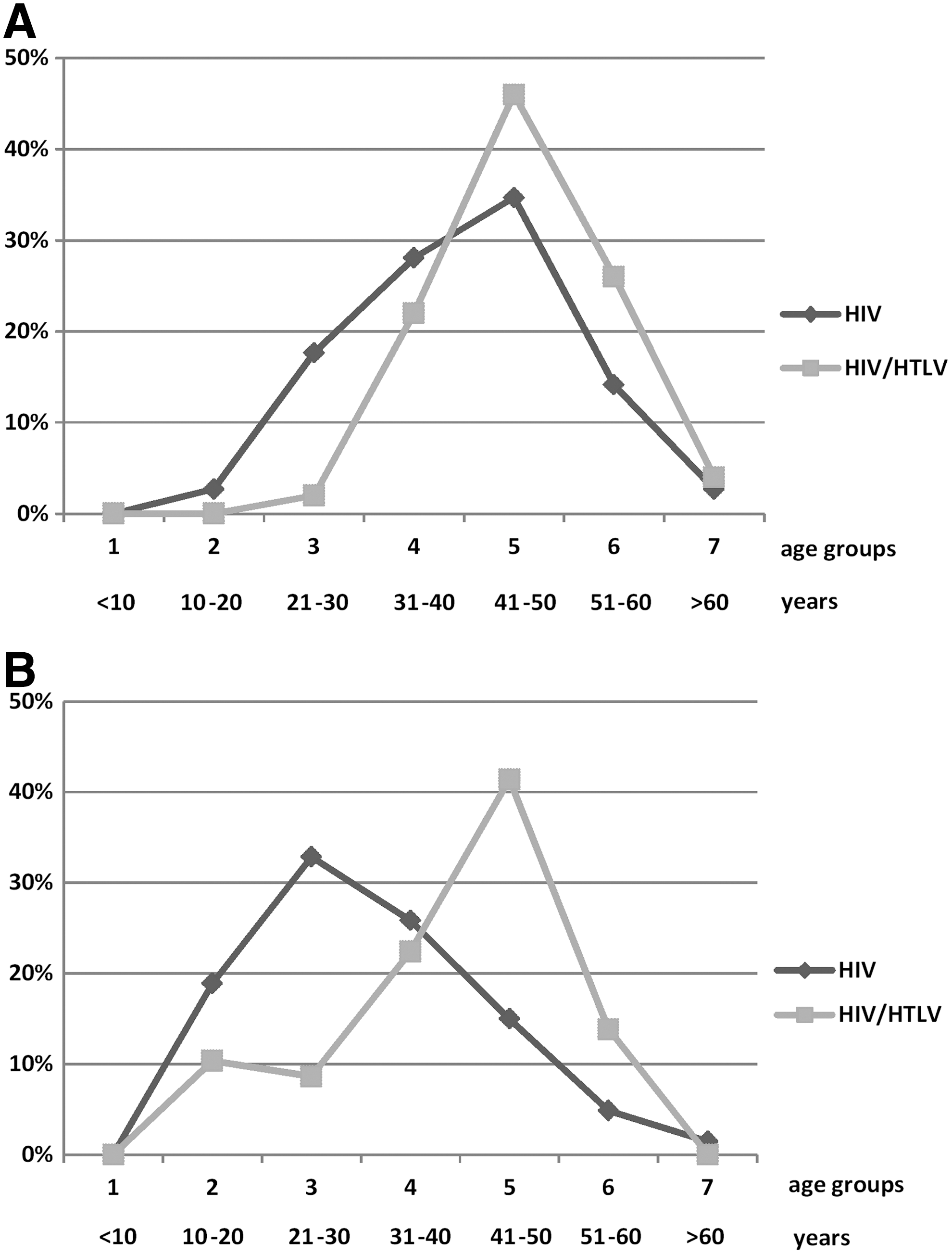
Percentages of HIV-1-infected and HIV-1/HTLV-1/2-coinfected patients attending a pioneer AIDS Reference Center (Group A)
In conclusion, this study emphasizes the importance of HTLV-1/2 surveillance in HIV-1-infected patients and suggests the use of LIA as a confirmatory assay. To understand the cause(s) of negative qPCR results, we are now sequencing the HTLV provirus to identify defective particles.
Footnotes
Acknowledgments
This study was supported by grants from the Ministério da Saúde/SVS/DDAHV BRAK57 # CA 125/13; DECIT/SCTIE/MS, CNPq, FAPESP, SES-SPPPSUS # 2012/51220-8; FAPESP # 2016/03654-0, CNPq PD # 302661/2015-8. K.R.C. is supported by a master fellowship from CAPES. The authors are indebted to Nadia Aparecida Costa for their technical assistance.
Author Disclosure Statement
No competing financial interests exist.