
Abstract
We show that intensification of treatment with maraviroc in patients chronically infected with HIV-1 receiving successful long-term antiretroviral therapy was not associated with improvements in HIV-related morbidity, HIV reservoir, microbial translocation, immune activation, or immune exhaustion in either gut or peripheral blood. The measurement of reservoir in both gut and blood longitudinally contributes to a paucity of data in the area.
Background
D
Intensification of ART in individuals with suppressed plasma viremia has not consistently reduced viral reservoir or improved immune function. 4,5 The C-C chemokine receptor type 5 (CCR5) entry inhibitor, maraviroc, is an attractive option as CCR5 receptors are most numerous in the gut and the drug penetrates tissue well. 6 Studies suggest a possible role in increasing CD4 count 7,8 and reducing immune activation. 5,9 The gut has been less investigated, 4 with no consensus on microbial translocation 5,10,11 or immune activation. 10,11
We investigated the effect of maraviroc intensification on gut immune function and viral reservoir.
Methods
Study design and recruitment
A prospective study whereby 10 individuals with chronic HIV infection with sustained virological suppression on ARV for >12 months and a CD4+ T cell count less than 500 cells/mm3 were intensified with a 24-week course of standard dose maraviroc. Blood samples were collected at weeks 0, 4, 12, and 24. At baseline and week 24, individuals underwent flexible sigmoidoscopy, in which 8–10 rectal biopsies were taken and fixed overnight in 10% normal buffered formalin at 4°C.
Laboratory tests
Bacterial translocation
Plasma bacterial 16s DNA was quantified by real-time polymerase chain reaction (RT-PCR). 11 Plasma sCD14 was quantified using the Quantikine Human sCD14 Immunoassay (R&D Systems, Minneapolis, MN), according to manufacturer's instructions. All samples were run in duplicate.
HIV reservoir and residual viraemia
Low copy viral load was measured with an internally controlled ultrasensitive quantitative RT-PCR able to detect 3 copies/ml. Purified peripheral blood CD4 T cells were analyzed by quantitative PCR (qPCR) for HIV-1 DNA (total and integrated) and cell-associated HIV-1 RNA unspliced transcripts as reported elsewhere. 12
For preparation of the gut biopsies for HIV reservoir quantitation, a commercial kit was used (Cat. No. 56404; Qiagen, Hilden, Germany), and the manufacturer's protocol modified as follows to ensure maximum yield of DNA. Biopsy sections were removed from paraffin blocks using a scalpel and placed into 1.5 ml micro centrifuge tubes. Samples were washed repeatedly with xylene and ethanol until the precipitate had disappeared, then dried at room temperature. Biopsy sections were incubated at 37°C and DNA was extracted using a commercial kit (QIAAMP DNA FFPE Tissue Extraction Kit, ID 56404; Qiagen). The resulting DNA was eluted into 200 μl and analyzed by qPCR using the same assays for peripheral blood CD4 cells as already detailed.
Immune activation and lymphocyte subsets
Peripheral blood mononuclear cells isolation were stained with the anchor markers (CD3- VioBlue, CD4 (VIT4)-VioGreen, and CD8-APC) and a live/dead marker near IR APC-Cy7 plus either an activation panel [CD25 (3G10)-PE, CD38-PE-Vio770, CD69-FITC, and anti-HLA-DR-PerCP] or an exhaustion panel (TIGIT-PE, TIM-3-FITC, LAG-3-PerCPeF710, and PD1-PE-Cy7). Cells were run on a MACSQuant and analyzed with FlowJo software v10 (Miltenyi Biotec).
Immunohistochemistry
Rectal biopsy sections were stained for CD4 (goat polyclonal; Novus Biologicals) and CD8 antibodies (rabbit polyclonal; Abcam). Images were analyzed in ImageJ and the distribution of cells was determined as described by Milano et al. 13
Statistics
For each outcome measure, the results at baseline and week 24 were compared using the paired t-test. Wilcoxon rank test was used to assess the impact of tropism on each parameter.
Results
Patient characteristics
The median age was 46 years. All patients were male with subtype B virus and were receiving two nucleoside reverse transcriptase inhibitors (NRTIs) combined with either a non-NRTI (n = 5) or protease inhibitor (n = 5). The mean CD4 T cell count was 321 cells/μl (SD 112), CD4:CD8 0.51 (SD 0.27), and nadir CD4 117 cells/ml (SD 135). All patients were maintained an HIV viral load <50 copies/ml throughout the study. Individual plots of viral reservoir, microbial translocation, and immune activation are shown in Table 1 and mean changes in parameters between week 0 and 24 are shown in Figure 1.
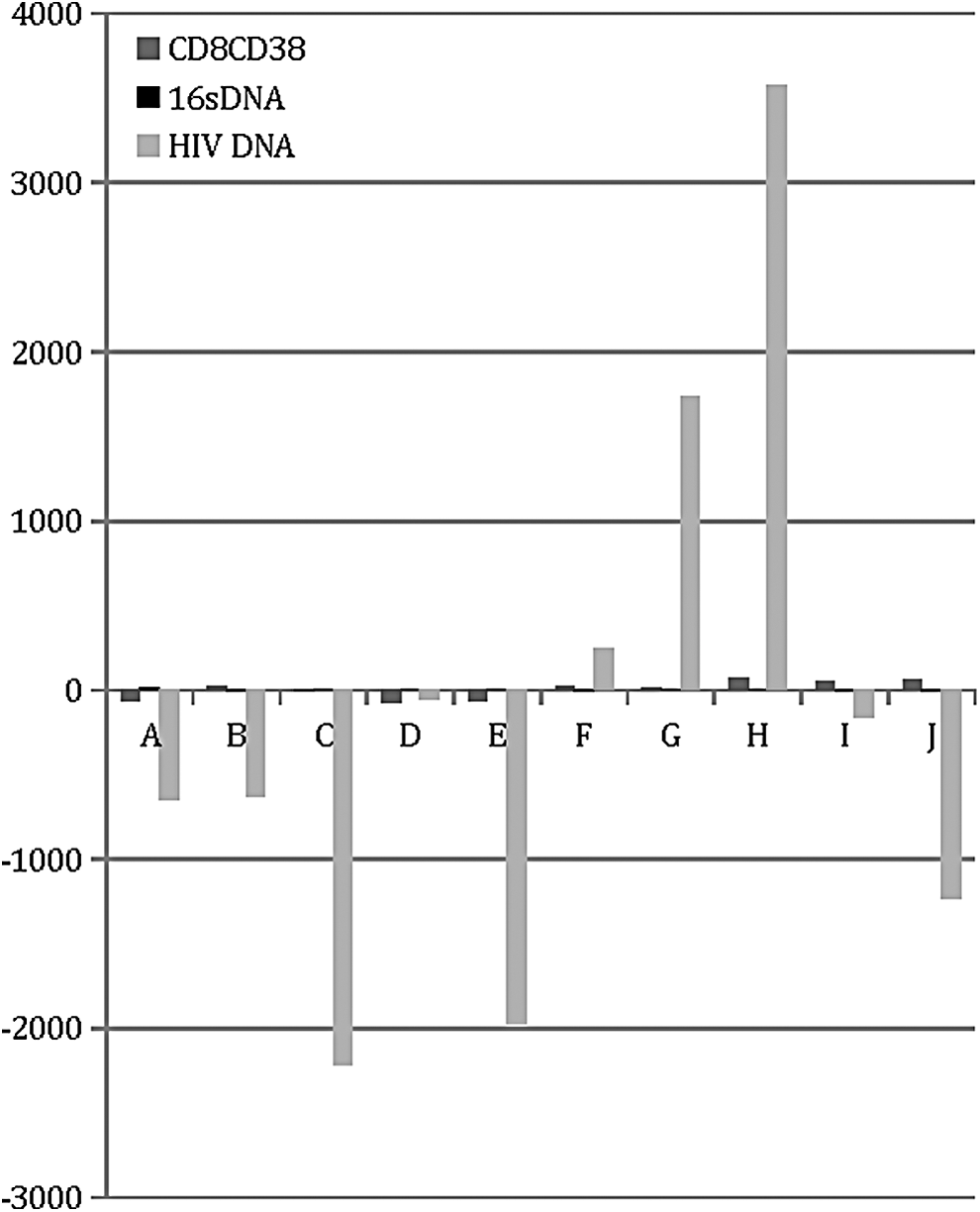
Individual change in key parameters between week 0 and 24.
Baseline to week 24
Clinical outcome/T cell subsets composition in blood and gut
Between baseline and week 24 (Table 2) in the blood, there was a nonsignificant increase of 48.22 CD4 T cells/ml (p = .275) and 39.23 CD8 T cells/ml (p = .672), whereas CD4:CD8 did not change. This was accompanied by a nonsignificant reduction in gut CD4 (−0.80; p = .087) and gut CD8 T cells (−5.59; p = .052). Changes in blood CD4 and CD8 lymphocytes did not correlate with changes in these cells in the gut.
SD, standard deviation.
Bacterial translocation
Between baseline and week 24, there was no significant change in 16s DNA copies (−0.60; p = .797) or sCD14a (+59.35; p = .637).
HIV reservoir
Neither HIV RNA, HIV DNA (blood or gut), or cellular HIV RNA changed significantly between baseline and week 24 or between baseline and week 12. At baseline, gut HIV DNA levels (mean 101,806 copies/million cells) were significantly higher than those in blood (3,669 copies/million CD4 T cells) (p = .017).
T cell activation and exhaustion
The level of activation of CD4+ T cells and CD8+ T cells showed nonsignificant increases from baseline to week 24 in six parameters (including CD8+CD38+HLADR; p = .677) with only percentage CD8+HLADR (+0.61; p = .048) increasing significantly. These findings were the same when analyzed from baseline to week 12 with only percentage CD8+ HLADR+ showing a significant change (+0.47; p = .001).
Eight out of 10 immune exhaustion markers increased from baseline to week 24 but only percentage CD8 tigit reached significance (+6.07; p = .006). This was supported by analysis of week 0 to 12 [percentage CD8 tigit (mean increase +5.82; p = .004)].
Tropism
Six out of 10 individuals had R5 virus. Tropism (R5 vs. X4 or X4/R5) did not correlate with changes in reservoir, immune activation, immune exhaustion, or microbial translocation (all p values > .05).
Discussion
In this pilot study, intensification of treatment with maraviroc in patients chronically infected with HIV-1 receiving successful long-term ART with a blunted CD4 immune response was not associated with any overall improvements in surrogate markers of HIV-related morbidity (CD4 T cell count or CD4:CD8 ratio), microbial translocation, immune activation, or immune exhaustion in either gut or peripheral blood. The isolated significant results in the absence of a broad class-wide effect on T cell exhaustion or activation are potentially interesting but should not be over interpreted. Furthermore, reservoir did not decline longitudinally in either gut or blood. The large gut HIV reservoir supports interventions targeting this compartment; however, the large intraindividual variation means that sample sizes may need to be large. The lack of impact of tropism on the effect of maraviroc on immunological function or reservoir size is novel but limited because of small sample size.
Overall, the study shows no role for maraviroc intensification to improve clinical or immunological outcomes or to provide complete viral inhibition. The null effect may also reflect that these individuals had more resistant immune dysfunction than intensification with ART could repair or the short duration of follow-up. The study is limited by the small sample size and lack of control group but the detailed analysis particularly of the gut further diminishes the investigation of maraviroc as an agent of intensification.
Footnotes
Acknowledgment
We acknowledge support from the biobank nurse funded by Guys and St. Thomas' NHS Trust and NIHR.
Author Disclosure Statement
No competing financial interests exist.