
Abstract
Correlates of bacterial vaginosis (BV) are poorly understood, especially in HIV infection. In a cohort study, HIV-seropositive and comparison seronegative women were assessed every 6 months during 1994–2015. BV was considered present when three of four Amsel criteria were met. Behavioral characteristics were assessed using structured interviews. Multivariable logistic regression used generalized estimating equation models to determine factors associated with BV. Cumulative incidence of BV over time was assessed using the log-rank test. Among 3,730 women (964 HIV seronegative and 2,766 HIV seropositive) contributing 70,970 visits, BV was diagnosed at 2,586 (14.0%) visits by HIV-seronegative women and 6,224 (11.9%) visits by HIV-seropositive women (p < .0001). The cumulative incidence of BV was 530/964 (55.0%) in HIV-seronegative women and 1,287/2,766 (46.5%) in seropositive women (p < .0001). In adjusted analyses, factors associated with BV were younger age, ethnicity, lower income, less education, recruitment site, recruitment in the 2001–2002 cohort, heavier drinking, current smoking, depression, and sex with a male partner; both hormonal contraception and menopause were negatively associated with BV. Of 533 women with prevalent BV, 228 (42.8%) recurred within a year, while persistent BV was found in 12.8% of participants; neither proportion differed by HIV serostatus. Time trends in the proportion of women with BV at any single visit were not identified. BV is common among women with and at risk for HIV, but HIV infection does not predispose to BV, which is associated instead with behavioral and cultural factors.
Introduction
B
In the Women's Interagency HIV Study (WIHS), we have found differences in BV prevalence by method of diagnosis: using clinically based Amsel criteria, BV was found in 18% of HIV-seropositive women, versus 14% of seronegative women (p = .009). When the presence of BV was determined by Gram stain using Nugent criteria, which reflect microflora changes, but do not require presence of discharge, BV was more frequent and, in contrast, was found more often in HIV-seronegative than HIV-seropositive women (42% vs. 48%, p = .03). 6 This difference suggests that subclinical disturbances in vaginal flora do not result from immunodeficiency, but from other factors. Rates of BV decreased over time in both groups, reaching a plateau of 30%–40% after some 4 years, and the decline among HIV-seropositive women was associated with increasing use of combination antiretroviral therapy. 7
A number of gaps remain in the understanding of the temporal dynamics of BV. The initial decline in BV prevalence within WIHS suggests that casefinding and therapy for BV may be effective in reducing BV rates, although competing factors, including advancing age, counseling, improvement in immune status after introduction of highly effective antiretroviral therapy (HAART), and changes in sexual behavior arising from disease awareness after enrollment, may have played a role. The relatively high frequency of BV across time suggests that BV remains a persisting problem. Correlates of clearance and persistence are little understood. We set out to explore BV frequency, clearance, and persistence risk across time in both HIV-seropositive and HIV-seronegative women.
Materials and Methods
The WIHS is a U.S. multicenter cohort study of health outcomes among HIV-seropositive women. WIHS also enrolled HIV-seronegative comparison women. Enrollment began on October 3, 1994, at 6 study consortia and, over time, has enrolled 4,068 women, including those enrolled during expansions from 2001 to 2002 and 2011 to 2012. The study was designed to ensure that the cohort reflected the evolving HIV epidemic in U.S. women. 8,9 At each site, human subject committees reviewed and approved the study, and all participants gave written informed consent. Follow-up continues, but this analysis includes information on BV through March 31, 2015.
At semiannual visits, women completed health questionnaires with trained interviewers, had physical examinations, including pelvic and speculum examinations, and had laboratory specimens collected. Visits were scheduled when participants were not menstruating, and women were instructed to avoid inserting any substance into the genital tract for 48 h before each visit.
BV was diagnosed when samples met at least three of four Amsel criteria (clue cells, pH >4.5, characteristic discharge, and amine odor with KOH). Several BV outcomes were assessed, including prevalence at recruitment, incidence, persistence (presence at three or more visits), and BV at each visit during the study time period. Demographic and medical characteristics were obtained at baseline visit, including HIV status, age, race/ethnicity, income, education, employment status, and depression (CES-D score of 16 or higher on the Center for Epidemiologic Studies Depression Scale). Baseline behavioral factors were also recorded, including intake of alcohol, smoking, injection drug use, number of sexual partners in the prior 6 months, use of hormonal contraception, menopause, and hysterectomy. BV was described by year and by categorized time periods based on pre-HAART era (1994–1995), introduction of HAART (1996–2000), and post-HAART era (2001–2015). For HIV-seropositive women, CD4+ T lymphocyte count (CD4 count), HIV RNA level, and HAART use were assessed. Unadjusted (chi-square statistics and independent sample t-tests) and adjusted analyses were conducted to assess the association between demographic and medical characteristics, and having BV at a given visit. Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated and multivariable logistic regression was used to determine factors independently associated with BV. To control for repeated measurements within women, generalized estimating equation (GEE) multivariable logistic regression models were fitted to obtain adjusted OR's and 95% CI. All variables that were associated with BV in the unadjusted analyses and factors associated with BV in the literature were included in preliminary multivariable models. The most parsimonious model was selected, including only variables that were significant in the final model. Cumulative incidence of BV over time was assessed by HIV status using incidence rate ratios (IRRs). Graphical displays of BV over time are also described. All analyses were performed in the SAS software, version 9.4 (SAS Institute, Inc., Cary, NC), and STATA software, version 13.1 (StataCorp, College Station, TX).
Results
After exclusions, we identified 3,730 women who had been assessed in WIHS for BV, 964 HIV seronegative and 2,766 HIV seronegative. These women contributed 70,970 visits (median of 19.0 visits/subject) at which BV was assessed by Amsel criteria and followed for a total of 38,520 person-years with a median follow-up of 11.2 person-years. Five percent of the sample had only one visit at which BV was identified. BV was found at 2,586 (14.0%) individual visits by HIV-seronegative women and at 6,224 (11.9%) visits by HIV-seropositive women (p < .0001).
Table 1 shows the distribution of demographic, behavioral, and medical variables among women who did and did not have BV by visit. Table 1 also presents unadjusted and GEE-adjusted ORs for the association of these variables with diagnosis of BV at any visit; we focused on adjusted results.
Unadjusted OR and 95% CIs and GEE-adjusted multivariable logistic regression.
p-Values obtained using the chi-square test unless otherwise specified.
Results reflect the most parsimonious GEE model. Blank cells reflect variables that were significant in unadjusted analyses, but were not included in adjusted GEE analysis, because when included, they were not significant.
Highly active antiretroviral therapy.
BV, bacterial vaginosis; CIs, confidence intervals; GEE, generalized estimating equation; HAART, highly effective antiretroviral therapy; ORs, odds ratios.
In these adjusted analyses, including both HIV-seropositive and HIV-seronegative women, BV was not associated with HIV status. When compared to visits that occurred before the introduction of HAART into the cohort, visits during introduction of HAART (1996–2000) were associated with the identification of BV, while visits during the remaining study period were not. Other factors that remained associated with BV were younger age, ethnicity, especially non-Hispanic black, income below $18,000/year, less than a high school education, recruitment site, recruitment in the 2001–2002 cohort, more drinks per week, current smoking, depression, and sex with a male partner in the prior 6 months; both hormonal contraception and menopause were negatively associated with BV (Table 1). Site and ethnicity were linked (p < .0001), reflecting regional differences in U.S. demographic site.
In a separate model (Table 2), multivariable GEE analysis for only HIV-positive women showed similar findings, except there was no significant association with the time period of introduction of HAART, and higher CD4 count was associated with lower risk BV.
Unadjusted OR and 95% CIs and GEE-adjusted multivariable logistic regression.
p-Value obtained by using the chi-square test unless otherwise specified.
Results reflect the most parsimonious GEE model. Blank cells reflect variables that were significant in unadjusted analyses, but were not included in adjusted GEE analysis, because when included, they were not significant.
Highly active antiretroviral therapy.
p-Value obtained by using the t-test for means.
p-Value obtained by using the median two-sample test for medians.
Further analysis demonstrated a significant time effect on the interaction of HIV status and BV. Including an interaction term for timing of visit around introduction of HAART into the cohort and HIV status demonstrated that in HIV-seronegative women, BV diagnosis was more likely during the 1996–2000 time period [adjusted OR (AOR) = 1.52, 95% CI 1.21–1.91, p = .0003], but not during the 2001–2015 time period (OR = 1.08, 95% CI 0.82–1.41, p = .60), when compared to the period before HAART introduction. In HIV-seropositive women, compared to the 1994/1995 period, the prevalence of BV at each visit did not significantly differ during the 1996–2000 (OR = 1.07, 95% CI 0.95–1.21, p = .28) and 2001–2015 (OR = 0.88, 95% CI 0.76–1.02, p = .09) time periods.
As shown in Figure 1, the cumulative incidence of new BV diagnoses was higher in HIV-seronegative women (530/964, 55.0% vs. 1,287/2,766, 46.5%, p < .0001).
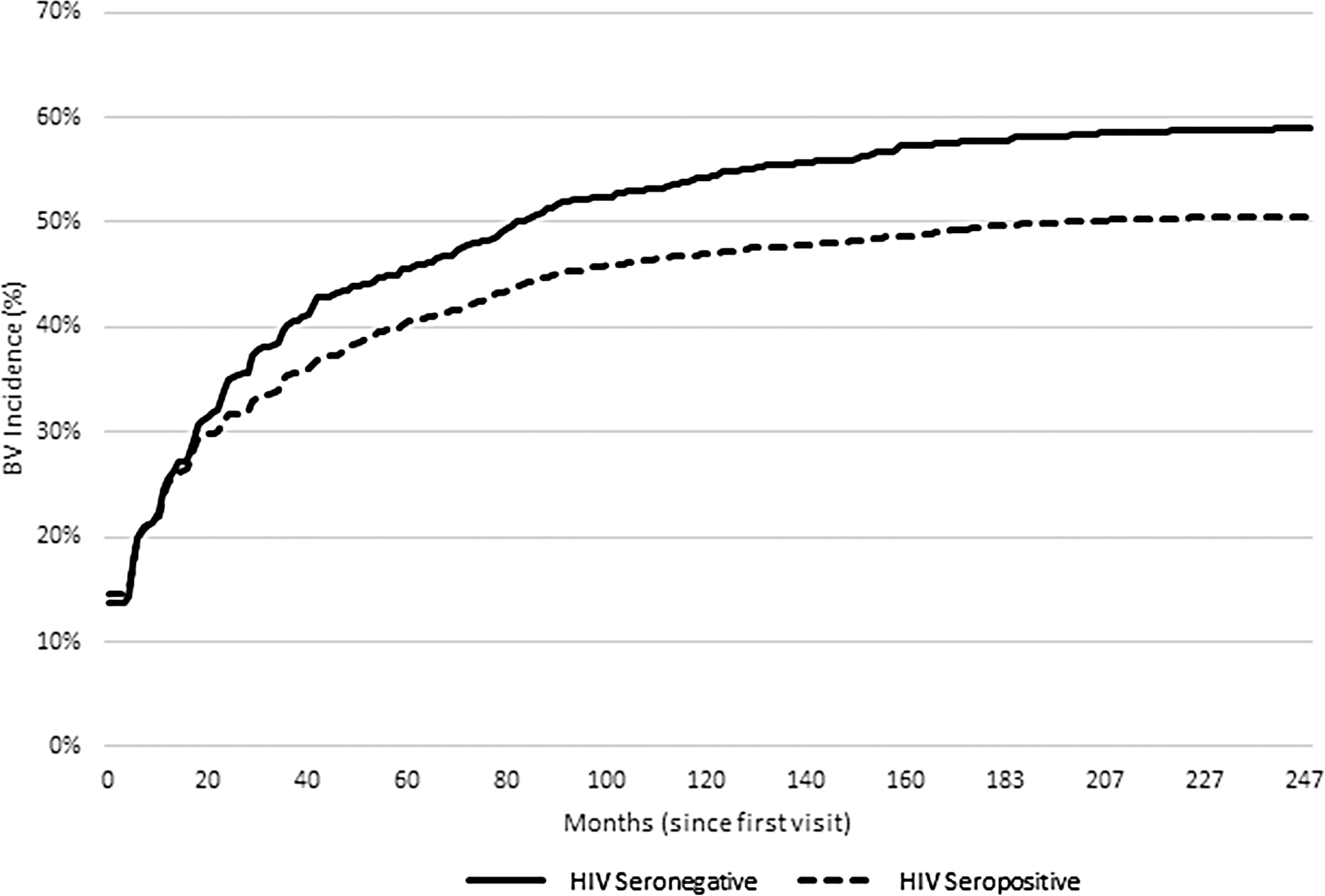
Cumulative incidence of bacterial vaginosis among HIV-seropositive and HIV-seronegative women.
Prevalent BV was found at intake in 400 (14.5%) HIV-seropositive women and 133 (13.8%) HIV-seronegative women (p = .61). Prevalent BV had a strong impact on subsequent BV diagnosis. Of 533 women with prevalent BV, 228 (42.8%) had BV within a year; this proportion did not differ by HIV serostatus. The incidence of BV was 22.2 cases/100 person-years among HIV-seropositive women and 24.7 cases/100 person-years among HIV-seronegative women (IRR = 0.90, 95% CI 0.86–0.94). Excluding prevalent cases at baseline, the overall incidence was slightly lower, but still showed that HIV-seropositive women had a lower rate of BV than HIV-seronegative women (20.8 vs. 23.4 cases/100 person-years, IRR = 0.86, 95% CI 0.85–0.93). Incidence was higher among those with prevalent BV (4,2l7 cases/100 person-years) compared to those who did not have BV at baseline (18.0 cases/100 person-years, IRR = 2.37, 95% CI 2.26–2.48).
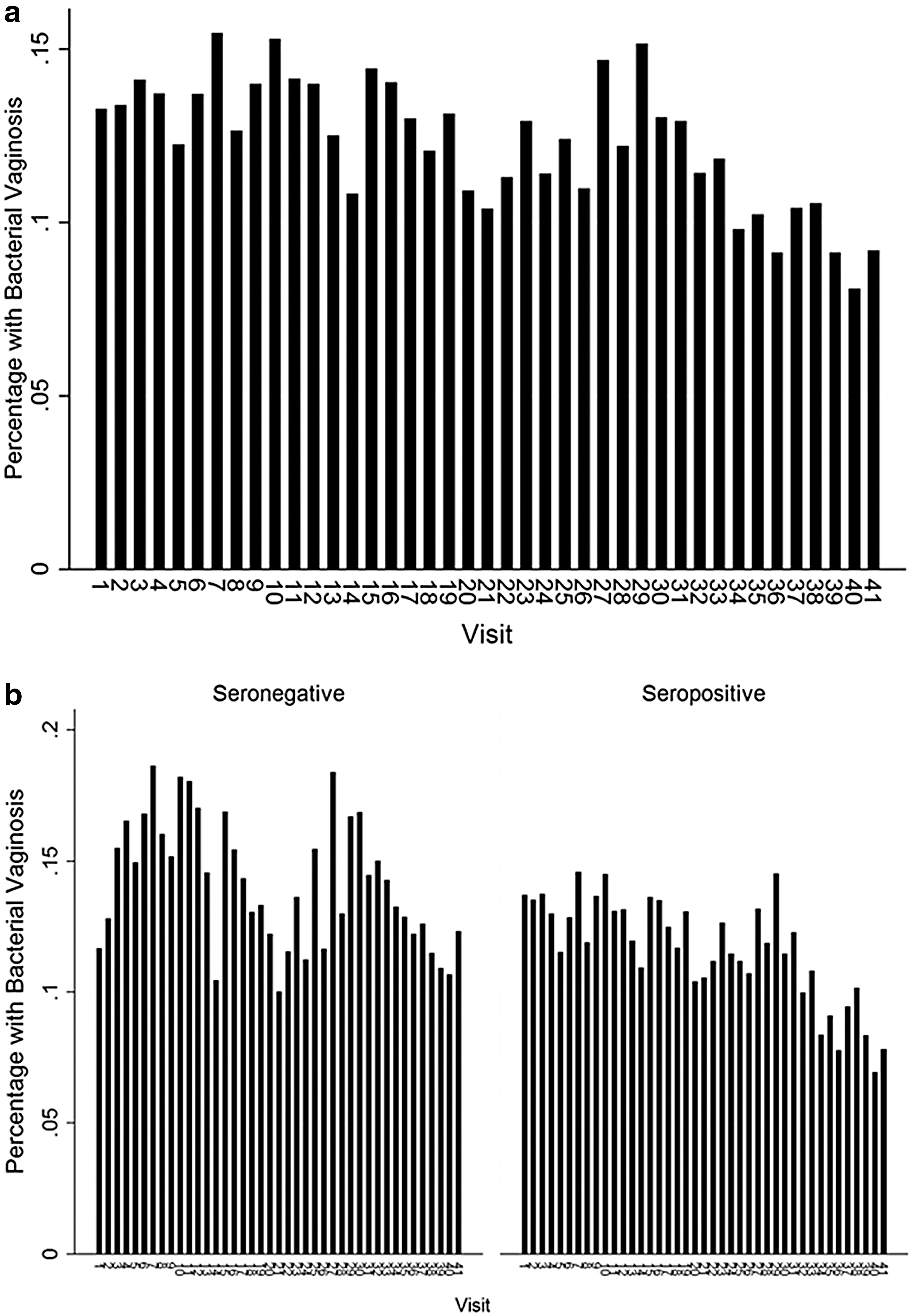
As shown in Figure 2a, the proportion of women with BV at any single visit ranged from 8.1% to 15.5%. This proportion fell significantly across time, but in multivariable analysis, the effect was small (OR for each later year 0.98, 95% CI 0.97–0.99). Figure 2b shows similar proportions by HIV serostatus. In seronegative women, the proportion of BV at a visit ranged from 10.0% to 18.6% (p = .003) and was 7.0% to 14.6% in seropositive women (p < .0001).
Persistent BV, defined as BV at three or more consecutive visits, was found in 12.8% of participants and did not vary by HIV serostatus (p = .78). Only 64 women (1.7%, 18 HIV seronegative and 1.9%, 46 HIV seropositive) had BV at every visit assessed (p = .67).
Discussion
BV was a common and recurring problem among the largely indigent and minority population enrolled in WIHS. Although an earlier study found a decline over time in BV rates diagnosed by Nugent criteria, in this expanded and extended cohort study of HIV seropositive and comparison seronegative women,
Recurrent BV was common among women with prevalent BV, and 12.8% of women studied had BV persisting for at least a year. Although fewer than 2% of women studied had BV at every visit, and 5% had only one visit at which they were assessed for BV, most women had BV identified at least once, with cumulative incidence over 50%.
However, the cause of BV remains obscure and is likely multifactorial. Etiologic factors include imbalances in the composition of the vaginal microbiota, possibly modulated by sexual and hygienic practices. In our study, multivariable analysis showed that HIV infection was not correlated with BV, a finding discordant with results previously reported from WIHS at baseline and during initial follow-up, as well as from the HIV Epidemiology Research Study. This may reflect selection among control HIV-seronegative women, who were required to have behaviors placing them at risk for HIV infection, which in turn might have predisposed to BV. BV in the current study was linked to age, ethnicity, recruitment site and year, smoking status, and sex with a male partner. This suggests that disturbances in the vaginal microenvironment arising from hygienic and sexual practices play a greater role in the development and persistence/recurrence of BV than cellular immune factors. Differences in cultural practices may explain why BV rates vary by ethnicity and site. Consistent with this, Bradshaw et al. found that recurrent BV occurs in more than 50% of cases within a year and is linked with the same sexual partner and inconsistent condom use, and reduced with oral contraceptive use. 10 Further research may require more detailed studies of sexual and genital hygiene behaviors linked to multiple BV assessment strategies, while genome-wide association studies may identify genetic components of risk.
Use of Nugent's Gram stain criteria for the identification of BV has some advantages over clinician assessment using Amsel criteria, especially reproducibility. We chose to use Amsel criteria to focus on women with clinical rather than purely bacteriological findings. Compared to Nugent criteria, diagnosis of BV by three of four Amsel criteria is 99% specific, but only 37% sensitive for BV. 11 More recently, nucleic acid hybridization tests have become available to detect Gardnerella vaginalis. These are more sensitive than Amsel criteria, but can require delay for reporting. 12 Bacteriological changes of subclinical BV are likely to be substantially more common than we found and may persist longer than we report. In addition, bacteriological changes without clinically evident discharge may be more common in HIV-seropositive women: Jamieson and associates in another large U.S. cohort study of women with HIV found that HIV infection was associated with BV by Nugent criteria and risk for BV by Nugent criteria rose as CD4 counts declined. 13
Antibiotic therapies for BV appear to be effective, but reversion to normal vaginal flora is often not durable. We found that 43% of women with BV had another episode within a year. Women are dissatisfied with current therapies and use self-help and behavioral modification to minimize risk, although some approaches such as douching may increase risk, with minimal impact. 14 Clinicians caring for women with BV may consider home screening, 15 probiotics, 16 suppressive antibiotics, or the provision of antibiotics to use when symptoms recur, to minimize delay arising from need for a clinician visit. 17
Footnotes
Acknowledgments
Data in this article were collected by the Women's Interagency HIV Study (WIHS). The contents of this publication are solely the responsibility of the authors and do not represent the official views of the National Institutes of Health (NIH). WIHS (Principal Investigators): UAB-MS WIHS (Michael Saag, Mirjam-Colette Kempf, and Deborah Konkle-Parker), U01-AI-103401; Atlanta WIHS (Ighovwerha Ofotokun and Gina Wingood), U01-AI-103408; Bronx WIHS (Kathryn Anastos), U01-AI-035004; Brooklyn WIHS (Howard Minkoff and Deborah Gustafson), U01-AI-031834; Chicago WIHS (Mardge Cohen and Audrey French), U01-AI-034993; Metropolitan Washington WIHS (Mary Young and Seble Kassaye), U01-AI-034994; Miami WIHS (Margaret Fischl and Lisa Metsch), U01-AI-103397; UNC WIHS (Adaora Adimora), U01-AI-103390; Connie Wofsy Women's HIV Study, Northern California (Ruth Greenblatt, Bradley Aouizerat, and Phyllis Tien), U01-AI-034989; WIHS Data Management and Analysis Center (Stephen Gange and Elizabeth Golub), U01-AI-042590; Southern California WIHS (Joel Milam), U01-HD-032632 (WIHS I–WIHS IV). The WIHS is funded primarily by the National Institute of Allergy and Infectious Diseases (NIAID), with additional cofunding from the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD), the National Cancer Institute (NCI), the National Institute on Drug Abuse (NIDA), and the National Institute on Mental Health (NIMH). Targeted supplemental funding for specific projects is also provided by the National Institute of Dental and Craniofacial Research (NIDCR), the National Institute on Alcohol Abuse and Alcoholism (NIAAA), the National Institute on Deafness and other Communication Disorders (NIDCD), and the NIH Office of Research on Women's Health. WIHS data collection is also supported by UL1-TR000004 (UCSF CTSA) and UL1-TR000454 (Atlanta CTSA).
Author Disclosure Statement
No competing financial interests exist.