
Abstract
Sexual exposure has been the predominant route of HIV-1 spread in Hebei Province, China. However, little information is available on HIV-1-transmitted drug resistance (TDR) among HIV-1-infected youths aged 16 to 25 years who are infected with HIV-1 and sexually active. In this study, the overall prevalence of TDR was 6.6% (10/152), a moderate level (5.0%–15.0%) according to World Health Organization Threshold Survey guidelines. However, the prevalence of TDR to protease inhibitors and nonnucleoside reverse transcriptase inhibitors was 4.6% (7/152) and 2.0% (3/152), respectively, which correspond to a low level (<5.0%). All TDR mutations (M46L/I, Y181C, K101E, and G190E) were found only in youths infected with HIV-1 through sexual activity. The prevalence of TDR among heterosexuals (10.0%, 3/30) was higher than that among men who have sex with men (5.8%, 7/120). TDR mutations resided in CRF01_AE (M46I/L and G190E) and subtype B (Y181C and K101E). Our findings will provide useful information on which drug regimens to use in treating the newly infected people with HIV-1.
T
Hebei Province neighbors Henan Province at its southern border and encompasses Tianjin and Beijing. The first case of HIV-1 infection in Hebei was identified in 1989 among workers returning from Africa. 5 In the 1990s, Hebei was defined as an area where most HIV-1 infections were caused by commercial blood products contaminated by HIV. 6 However, the exposure owing to high-risk sexual behavior has become the predominant driver of a trend that has been increasing since 2005 of newly diagnosed HIV-1 infections in the province. 7
Free ART was launched in 2003 for Hebei Province. The national guidelines for ART have changed over the years from treating patients with CD4 < 200, to CD4 < 350 in 2011, to now treating all HIV-diagnosed individuals in China with ART.
To date, ART has been implemented for a total of 10 years and has improved patient quality of life. 8 However, a high prevalence of HIV-1 drug resistance (DR) has been observed among patients receiving ART in Hebei. 9 Low prevalence of TDR has also been identified among recently HIV-infected men who have sex with men (MSM) at MSM sentinel surveillance points. 7 With the scale-up of ART, TDR surveillance will provide useful information on which drug regimens to use in treating people newly infected with the virus. Moreover, sequences and phylogenetic analyses can provide much evidence about how HIV is spreading in the population. The objective of our study was to investigate the prevalence of TDR among newly diagnosed, treatment-naive young people, aged 16 to 25 years, who were infected with HIV-1 in 2013.
According to the World Health Organization (WHO) TDR surveillance threshold, 10 we enrolled in the study a total 152 of 214 treatment-naive youth who were newly diagnosed with HIV-1 in 2013 and who were from all 11 prefectures of Hebei Province (Table 1). All participants signed written informed consent forms. Ethical approval was obtained from the local Ethics Committee at Hebei Provincial Center for Disease Control and Prevention.
Single include unmarried, widowed, and divorced.
F, Fisher-exact test; IDU, intravenous drug use; MSM, men who have sex with men; TDR, transmitted drug resistance; URF, unique recombinant form.
Participants’ demographic data were obtained by face-to-face interviews using a standard questionnaire during collection of their blood samples. Within 6 h of collection, 500-μl plasma samples were separated from whole blood and were used to extract, amplify, and sequence HIV-1 RNA.
An HIV-1 partial pol gene (HXB2:2147–3462) was amplified, sequenced, edited, and assembled using an in-house method, as reported previously.
11
The HIV-1 subtype was determined using the neighbor-joining (NJ) phylogenetic tree analysis. Reference sequences (A-D, F-H, J, K, CRF01_AE, CRF08_BC, and CRF07_BC) were obtained from an HIV database (
Viral pol gene sequences were submitted to the Stanford University HIV Drug Resistance Database (
Demographic characteristics of 152 young people infected with HIV-1 are summarized in Table 1. Among these, 91.4% (139/152) were male and 79.6% (121/152) were unmarried. Han nationality accounted for 97.4% (148/152) of the population. Mean age was 21.9 (16–25) years and mean first CD4 cell counts were 270.8 (16–1149) cells/μl. A total of 98.7% (150/152) participants had a history of sexual exposure to HIV, including MSM (78.9%, 120/152) and heterosexuals (19.7%, 30/152). Another 1.3% (2/152) had a history of intravenous drug use (IDU).
In this study, phylogenetic analysis of 152 pol gene sequences (Fig. 1) indicated that the predominant subtype was CRF01_AE, accounting for 53.3% (81/152), followed by CRF07_BC (26.3%, 40/152), subtype B (17.1%, 26/152), unique recombinant forms (URFs; 2.0%, 3/152), and CRF08_BC (1.3%, 2/152). Mosaic structure analysis identified that the recombinant pattern of all three URFs was CRF01_AE/BC.
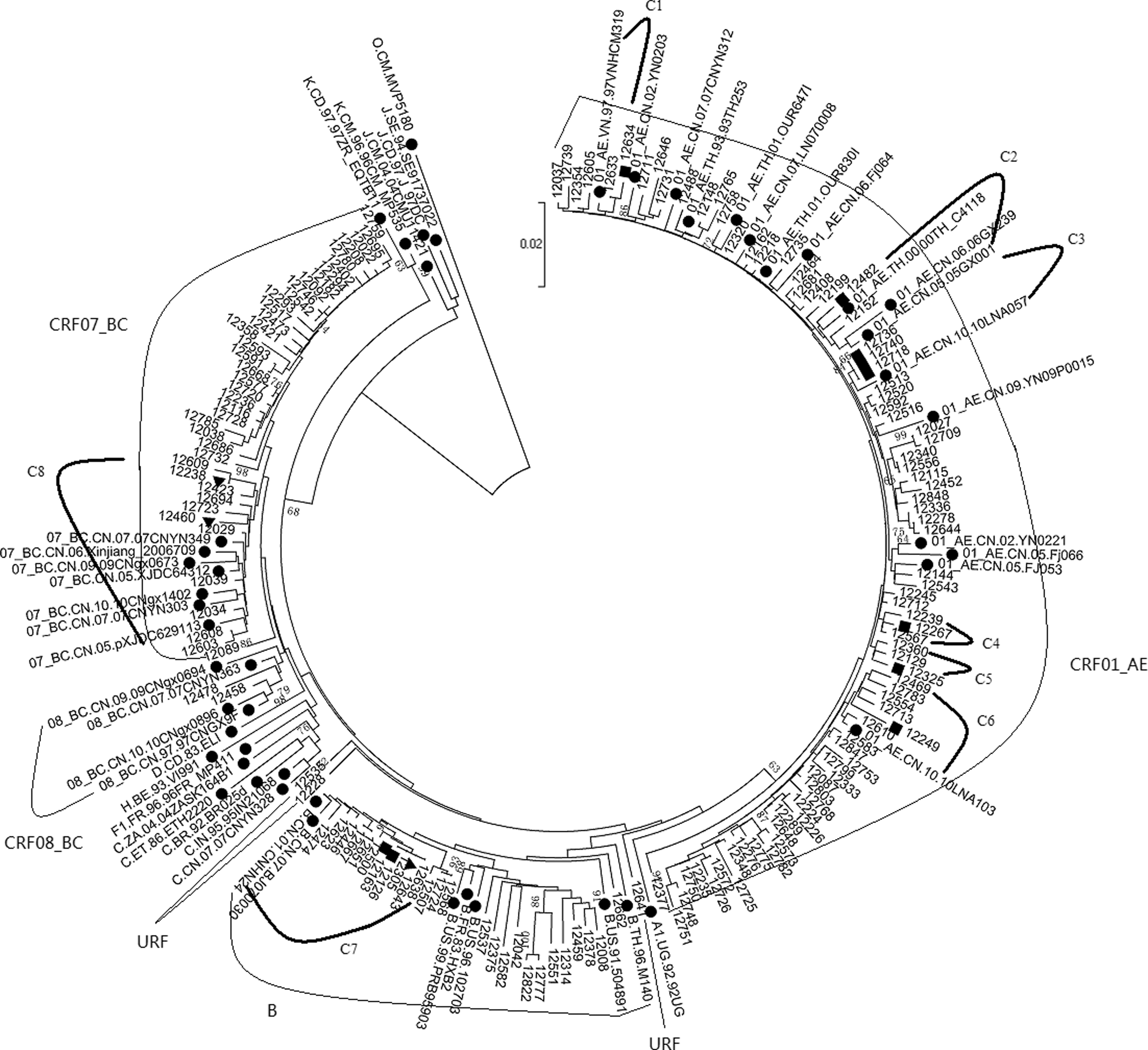
The phylogenetic tree analysis based on HIV-1 partial pol gene sequences from 152 newly diagnosed HIV-1 infected youths without the treatment in Hebei. The neighbor-joining phylogenetic tree was constructed with our sequences and the reference gene sequences of subtype A-D, F-H, J, K, O, CRF01_AE, CRF07_BC, and CRF08_BC obtained from the HIV database (
Table 2 reveals that 13 participants harbored DR to protease inhibitors (PIs; 7 cases) and nonnucleoside reverse transcriptase inhibitors (NNRTIs; 6 cases). Only one mutation was found in each of these 13 participants. M46L/I, Y181C, K101E, and G190E were included on the 2009 WHO TDR mutation list. The overall prevalence of TDR among participants was 6.6% (10/152), a moderate level (5.0%–15.0%) according to WHO Threshold Survey guidelines. 13 This is higher than the prevalence of HIV TDR in 20 countries (3.7%) 14 and in 19 provinces or cities (4.9%) of China. 15 Furthermore, the prevalence of TDR after 10 years of ART scale-up in Hebei (6.6%) is clearly higher than the 3.2% after 8 years in Guangxi Province 16 and the 4.3% after 7 years in Dehong Prefecture of Yunnan Province 17 ; however, this rate is lower than the 14.3% after 8 years of ART scale-up in Henan Province. 18
Underlined bold mutations are not included in the 2009 World Health Organization TDR mutation list.
NNRTIs, nonnucleoside reverse transcriptase inhibitors; PIs, protease inhibitors.
As shown in Figure 1, those sequences containing TDR mutations (black squares) and TDR-associated mutations (black triangles) formed eight different clusters within CRF01_AE, subtype B, and CRF07_BC. Within CRF01_AE, six clusters containing TDR were found, including cluster 2 in the heterosexual group, cluster 3 in the MSM group, and another four clusters in the MSM and heterosexual groups. In particular, cluster 2 was associated with Guangxi (GX), and clusters 3 and 6 were closely associated with Liaoning (LN). Within subtype B, one DR transmission cluster (cluster 7) containing eight MSM sequences and three heterosexual sequences were identified, being related to Henan (HN) and Beijing (BJ). Within CRF07_BC, cluster 8 included sequences from the MSM (eight cases), IDU (one case), and heterosexual (two cases) groups. Those sequences harboring TDR-associated mutations were related to provinces with high HIV prevalence in China, such as Xinjiang, Yunnan, and Guangxi. The above facts show that DR is spreading rather rapidly among the population through sexual contact.
The main mutation associated with TDR to PIs was M46L/I, which had a prevalence of 4.6% (7/152). Three TDR mutations were identified in the NNRTI coding region, including Y181C (0.7%, 1/152), K101E (0.7%, 1/152), and G190E (0.7%, 1/152). The prevalence of TDR to NNRTIs was 2.0% (3/152). The prevalence of TDR to PIs and NNRTIs was at low levels (<5.0%). No TDR to NRTIs was found in this study.
As indicated in Tables 1 and 2, TDR mutations were mainly found in Shijiazhuang (9.4%, 3/32), Tangshan (11.4%, 4/35), Xingtai (33.3%, 1/3), and Cangzhou (9.5%, 2/21) prefectures; no TDR was observed in other prefectures. TDR mutations were observed in CRF01_AE (M46I/L and G190E) and subtype B (Y181C and K101E) only. The prevalence of TDR in CRF01_AE and subtype B was 9.9% (8/81) and 7.7% (2/26), respectively. All TDR mutations were found only in young people infected with HIV-1 through sexual activity, and the prevalence of TDR among heterosexuals (10.0%, 3/30) was higher than that among MSM (5.8%, 7/120). Although no TDR mutations were found for some demographic characteristics, the distribution of TDR by sex, age, first CD4 count, transmission route, marital status, ethnicity, subtype, and prefecture showed no significant differences (Table 1).
According to the Stanford DR algorithm, M46I/L can confer low-level resistance to nelfinavir (NFV). NFV has never been used in Hebei. We can infer that M46I/L may be derived from HIV-1-resistant strains in other provinces or foreign countries rather than PI selection in Hebei. Y181C is responsible for significant resistance to efavirenz (EFV), etravirine (ETR), rilpivirine (RPV), and nevirapine (NVP). K101E causes intermediate resistance to NVP and low-level resistance to EFV, ETR, and RPV. G190E results in high-level resistance to NVP and EFV and intermediate resistance to RPV and ETR.
In addition, both V108I and F227FL, which were not included on the 2009 WHO TDR surveillance list, 12 are nonpolymorphic TDR-associated mutations. V108I is an accessory mutation identified in two MSM (from Tangshan and Cangzhou) harboring CRF07_BC and subtype B (Table 2), respectively, and can result in low-level resistance to NVP and EFV. F227FL, detected in one MSM (from Chengde) with CRF07_BC (Table 2), is closely associated with intermediate resistance to NVP and low-level resistance to EFV.
Of the above drugs, EFV, ETR, and NVP are first-line antiretroviral drugs that have been included in ART regimens since the launching of ART in 2003. This suggests that TDR mutations occur owing to selection for antiretroviral drugs.
Currently, sexual exposure has become the predominant route for the spread of HIV-1 in Hebei. Moreover, CRF01_AE, subtype B, and CRF07_BC are the main subtypes circulating in the province. This study is the first investigation of TDR among newly diagnosed, treatment-naive young people aged 16 to 25 years, infected with HIV-1 in Hebei, and reveals a moderate prevalence of TDR (6.6%) after 10 years of ART in the province. The circulation of TDR HIV-1 strains among youth who are sexually active will cause rapid development of HIV-1 genetic diversity and reduce the effort to improve therapy outcomes. Our findings suggest that it is important to continually monitor HIV-1 TDR among treatment-naive young people who have been newly diagnosed with HIV-1 and who are sexually active. Medical interventions as well as interventions for high-risk sexual behavior are needed to help manage the HIV-1 epidemic in Hebei, China.
Footnotes
Acknowledgments
The authors thank the staff of local Centers for Disease Control and Prevention in Hebei Province for their assistance, especially with the fieldwork. This study was implemented with the support of the Natural Science Fund of Hebei Province (H2016303006). All nucleotide sequences reported in this study have been submitted to GenBank with accession numbers KX198563, KX198583, KX198569, KX198571, KX198581, and KX791498-KX791637.
Authors’ Contributions
The study was conceived and designed by X.L. and X.K. X.L. and Y.L. carried out the study and analyzed the experimental data. X.L. drafted the article. Y.L. edited and assembled sequences. Y.L., J.L., Z.C., and S.C. contributed to the acquisition of epidemiological data. All authors read and approved the final article.
Author Disclosure Statement
No competing financial interests exist.