
Abstract
A decrease in the rate of acquired antiretroviral (ARV) drug resistance (ADR) over time has been documented in high-income settings, but data on the determinants of this phenomenon are lacking. We tested the hypothesis that in heavily ARV-experienced patients in the Mexican ARV therapy (ART) roll-out program, the drop in ADR would be associated with changes in ARV drug usage. Genotypic resistance tests obtained from 974 HIV-infected patients with virological failure and at least 2 previously failed ARV regimens from throughout the country were analyzed for the presence of nucleos(t)ide reverse transcriptase inhibitors, non-nucleoside reverse transcriptase inhibitors, and protease inhibitor (PI) resistance-associated mutations (RAMs). Patients were divided into two groups according to their first ART start date: 488 patients initiated ART before mid-2003 (group 1) and 486 after mid-2003 (group 2). The rate of RAMs, median resistance score of several sentinel ARVs, and composition of ART drugs in patient's entire treatment history were compared between both groups. Patients in group 2 were less likely to have >3 thymidine analogue-associated mutations (TAMs) and >3 PI-mRAMs [adjusted odds ratio (aOR) = 0.37; 95% confidence interval (95% CI) = 0.25–0.54; p < .001 and aOR = 0.53; 95% CI = 0.36–0.77; p = .001, respectively] and had a significantly lower resistance score for zidovudine, tenofovir, ritonavir-boosted (r)-lopinavir, r-atazanavir, and r-darunavir than group 1 patients. A significantly lower proportion of patients in group 2 used monotherapy, bitherapy, thymidine analogue-containing regimens, nonboosted PI-containing regimens, and low resistance barrier PI-containing regimens. In Mexican ARV-experienced patients, the occurrence of TAM and PI-mRAM has significantly declined over time. This can be explained by treatment optimization in the national ART roll-out program in recent years.
Introduction
S
In Mexico, universal ART coverage started in 1997 for employees in the formal sector and was subsequently expanded in 2003 to informal sector workers and the unemployed. 7 In 2008, the Ministry of Health (MoH) created a national board of clinicians with several years of ART experience to assist Mexican physicians in the prescription of deep salvage regimens likely to be successful in heavily treatment-experienced patients and in the optimization of the use of new expanded activity drugs in routine clinical care. 8 Data from these patients on ART prescription history and drug resistance after virological failure to multiple regimens provided a unique opportunity to address whether an association between these two sets of information actually exists.
The aims of this study were as follows: first, to determine the temporal trends in reduced HIV susceptibility to various ARVs and in the rate of RAMs in resistance tests obtained in routine clinical care in a country-wide representative sample of heavily ARV-exposed patients, and second, to assess whether these changes could be explained by a different frequency of use of suboptimal ARV regimens at any time in the patients' entire treatment history.
Materials and Methods
Study sample population and data collection
This is a cross-sectional comparison study. All HIV-infected patients requiring deep salvage regimens in the ART roll-out program operated by the Mexican MoH are reviewed by a National Peer Advisory Committee for physicians caring for heavily ART-experienced patients in HIV clinics (CORESAR for its acronym in Spanish). 8 During this process, the physician completes a structured application form that collects data concerning patient plasma HIV-1 viral load measurements and drug-resistance tests, CD4+ T cell counts, coinfections, clinical events, concurrent medications, a complete history of ART, and the reasons for drug changes (e.g., virological failure, adverse events, nonadherence, regimen simplification, or pharmacological interactions) since diagnosis with HIV.
The ART administration, logistics, and surveillance system (SALVAR for its acronym in Spanish) is a web-based secure information system that includes data on all individuals living with HIV who are enrolled in and receiving care through the MoH program; this system is used by all 173 prevention and treatment public health facilities (outpatient clinics and hospitals) located in the 32 states of Mexico. Clinicians are required to populate the data in this electronic system. Patients' consent to registering his or her personal data is obtained by the physician at the first visit, as mandated by law. The information used for this study's purposes was obtained from a structured application form completed by the practitioner when asking for peer advice from the CORESAR and was validated and/or complemented by reviewing the ART prescription data from SALVAR.
A database containing this information as well as the results of genotypic resistance tests (genRTs) from routine testing was created. The eligibility criteria required the following: patients (1) were considered cases of ARV virological failure (ongoing viral replication as defined by an HIV plasma viral load greater than 500 copies/ml in at least two prior consecutive measurements) after receiving at least two prior failed ART regimens, (2) were 18 years or older, and (3) had at least one genRT conducted before the cross-sectional analysis. The enrollment period of the study sample was from November 5, 2008, to May 14, 2015.
Analysis of drug resistance
genRTs are obtained as part of routine clinical care when a patient receiving ART experiences virological failure; the corresponding tests from all eligible patients were analyzed. Major resistance mutations were defined according to the IAS-USA 2015 list. 9 The level of clinically relevant loss of antiviral activity for each drug was determined using the Stanford HIVdb algorithm. 10 The total mutation penalty score was retrieved for each of the three sentinel nucleos(t)ide reverse transcriptase inhibitors (nRTIs) (lamivudine—3TC, zidovudine—AZT, and tenofovir disoproxil fumarate—TDF); three non-nucleoside reverse transcriptase inhibitors (NNRTIs) (efavirenz—EFV, nevirapine—NVP, and etravirine—ETV), and four sentinel protease inhibitors (PIs) (ritonavir-boosted atazanavir—ATV/r, ritonavir-boosted lopinavir—LPV/r, ritonavir-boosted tipranavir—TPV/r, and ritonavir-boosted darunavir—DRV/r). HIV harbored by the patients was classified as susceptible (penalty score 0–14), low/intermediate resistance (penalty score 15–59), or high-level resistance (penalty score ≥60) for each studied drug. In patients with more than one genRT, all RAMs identified in all tests were pooled and analyzed. The ViroSeq HIV-1 Genotyping System (Abbott) method was used in the majority of the genRTs and no differential trend over time in the rate of use of this technique occurred during the study period.
Assessment of ART regimens
All drug combinations in each patient's entire ART history were analyzed for the presence of suboptimal regimens. Suboptimal regimens were defined as mono or dual therapies (i.e., regimens comprising only one or two nRTIs, respectively), any drug combination including a non-(ritonavir) boosted PI (except for nelfinavir), or any drug combination including a PI with a low barrier for developing resistance (indinavir, saquinavir, or nelfinavir). A double PI-containing regimen was defined as the concomitant use of two PIs, regardless of the use of ritonavir as a drug booster.
Data analysis
Patients were divided into two groups according to their first ART start date: group 1 included patients who initiated ART before mid-2003 and group 2 comprised those who initiated ART after mid-2003. This time point was chosen as it is the median of date of ART initiation in the whole study sample population and the enrollment period was the same for both groups.
The rate of RAMs, resistance score of several sentinel ARVs, and frequency of suboptimal ART regimens and of regimens containing a thymidine analogue nucleoside (zidovudine or stavudine) were compared between the two groups. Data are reported as absolute values and percentages as well as medians and interquartile ranges. The differences between the groups in the percentage of patients with mutation-resistant HIV and in the percentage of patients with a genRT showing a susceptible, low/intermediate resistance or high-level resistance virus were tested with chi-square tests. We used multivariate logistic regression modeling to estimate the associations of the prevalence of drug RAMs with ART start date as a binomial variable, generating confounder-adjusted odds ratios (aORs) and 95% confidence intervals (95% CIs). This study was approved by the Research Ethics Committee of the Instituto Nacional de Ciencias Médicas y Nutrición “Salvador Zubirán.”
Results
Data regarding the genRT results and the complete history of ART were obtained from 974 eligible HIV-infected patients. NNRTI-RAMs were analyzed in genRT from 322 individuals in the study sample; this subsample was selected based on the ARV combination used during the genRT to include only patients in whom this test was performed under the selective pressure of a member of this drug class (efavirenz or nevirapine).
A significantly lower proportion of the 486 patients who initiated ART after mid-2003 had genRTs showing thymidine analogue-associated mutations (TAMs) (M41L, D67N, K70R, L210W, T215Y, T215F, and K219Q/E) and mutation L74V compared with the 488 patients initiating ART before mid-2003 (Fig. 1). In contrast, the proportion of patients with genRT results showing M184V and NNRTI-RAM mutations (K103N, Y181C and G190A) remained similar, and the rate of patients with a K65R mutation significantly increased (13.7% vs. 4.3%; p < .001) between both group of patients (Fig. 1). Moreover, a significantly lower proportion of patients who initiated ART after mid-2003 had genRT results showing the most commonly found major resistance mutations in the protease gene (PI-mRAMs) (L33F, M46I/L, I47V, Q58E, V82A, I84V, and L90M) and three or more darunavir-RAMs (Fig. 2).
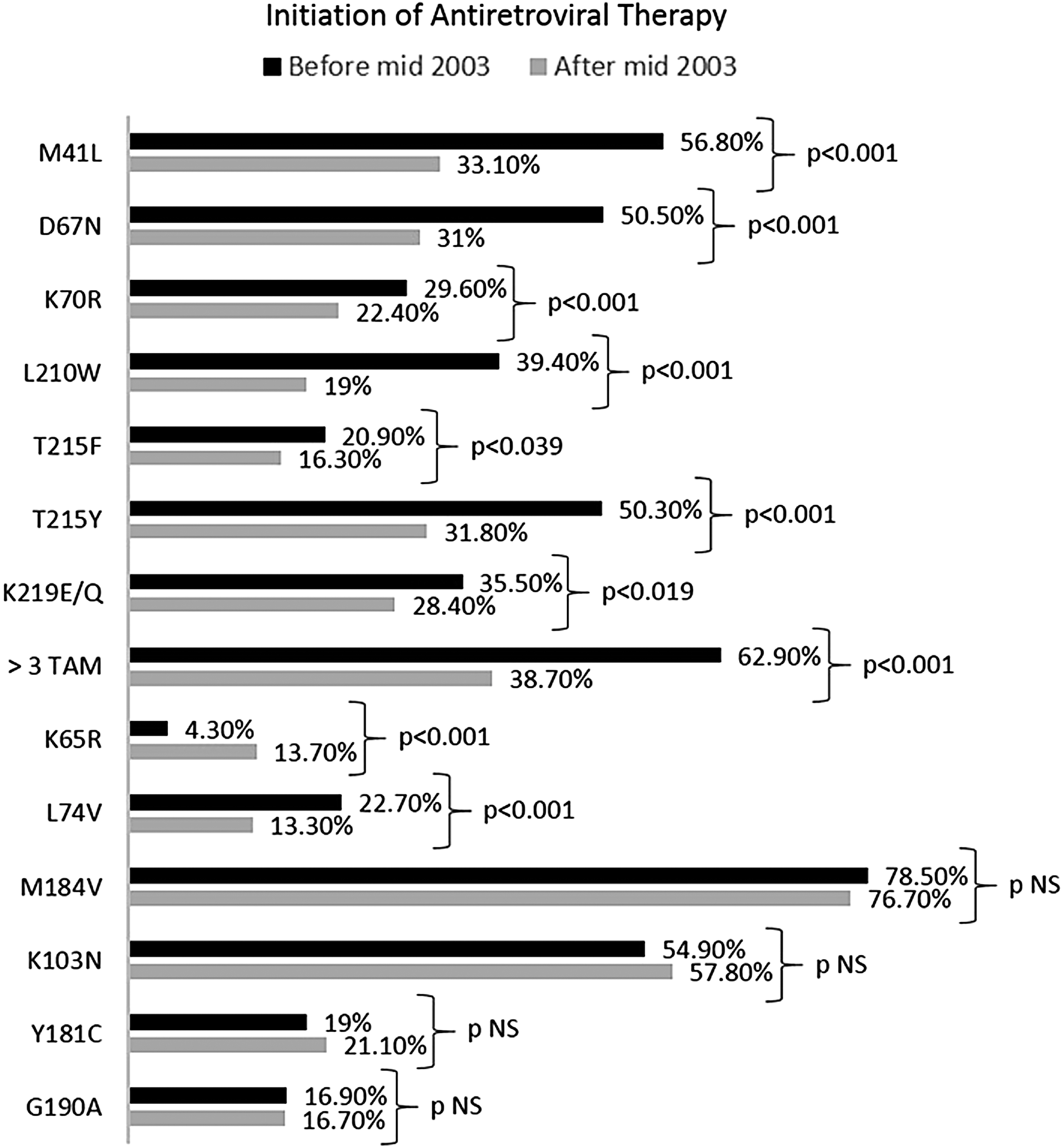
Frequency of patients with a HIV-genotypic resistance test showing specific mutations in the reverse transcriptase gene. Comparison between the 488 patients starting antiretroviral therapy before mid-2003 and the 486 patients starting antiretroviral therapy after mid-2003. NS, not significant. TAM, thymidine analogue-associated mutations
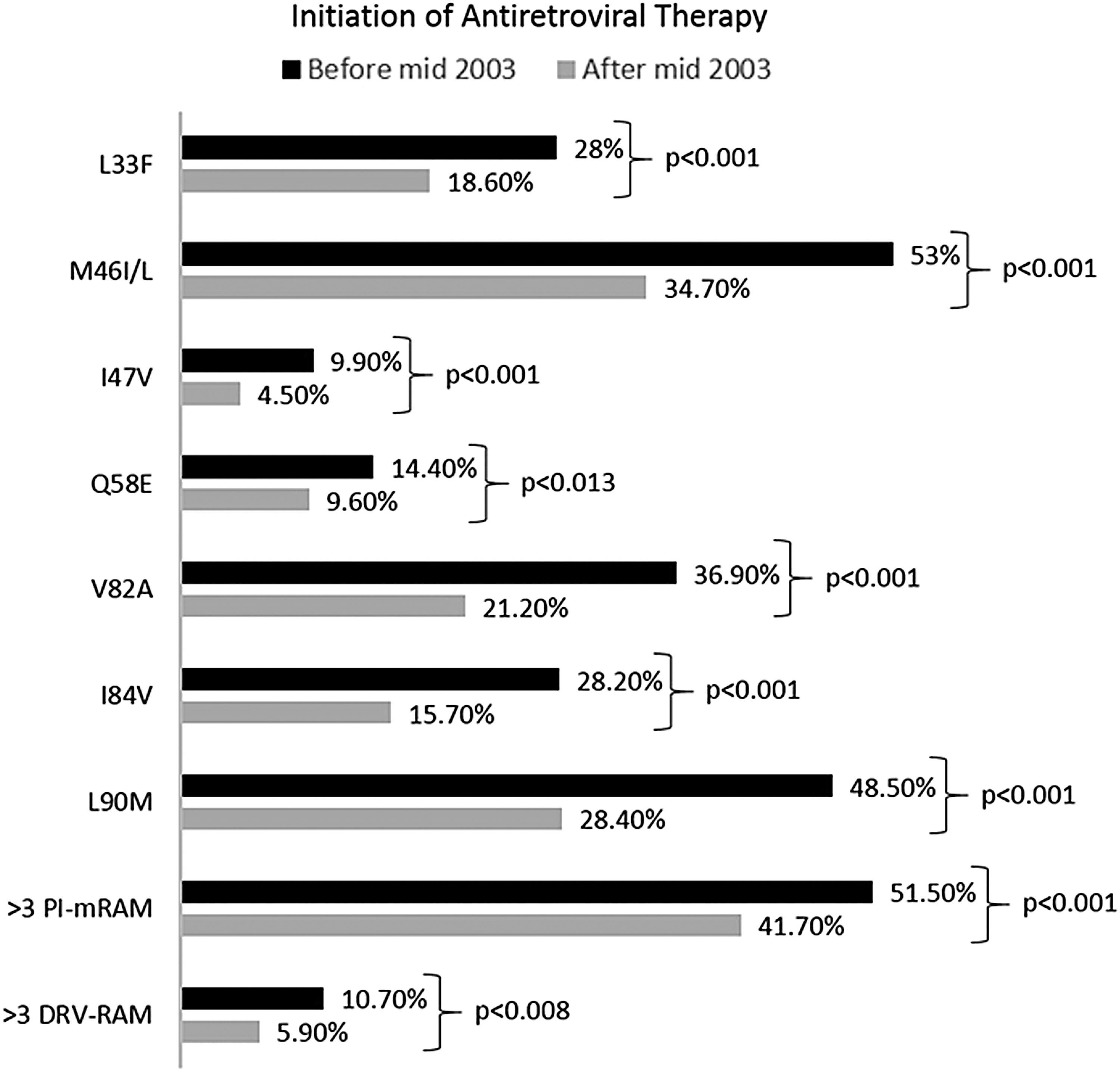
Frequency of patients with an HIV-genotypic resistance test showing specific major mutations in the protease gene. Comparison between the 488 patients starting antiretroviral therapy before mid-2003 and the 486 patients starting antiretroviral therapy after mid-2003. DRV-RAMs, darunavir resistance-associated mutations; PI-mRAM, protease inhibitor major resistance-associated mutations.
After adjusting for potential confounders (age, time receiving ART, number of prior ARV regimens, and nearest previous to genRT vRNA plasma level and T-CD4+ cell count), we found a 63% reduction in the prevalence of three or more TAMs (OR = 0.37; 95% CI = 0.25–0.54; p < .001) and a 47% reduction in the prevalence of three or more mPI-RAMs (OR = 0.53; 95% CI = 0.36–0.77; p = .001) in patients who initiated ART after mid-2003 compared with patients starting ART before this date.
The proportion of patients with genRTs showing viral susceptibility (Stanford HIVdb system total penalty score 0–14 points) to zidovudine, tenofovir, lamivudine, ritonavir-boosted atazanavir, ritonavir-boosted lopinavir, ritonavir-boosted tipranavir, and ritonavir-boosted darunavir significantly increased in patients who initiated ART after mid-2003 compared with patients starting ART before this date. No change in the proportion of patients with genRTs showing HIV susceptibility to nevirapine, efavirenz, or etravirine was observed (Fig. 3).
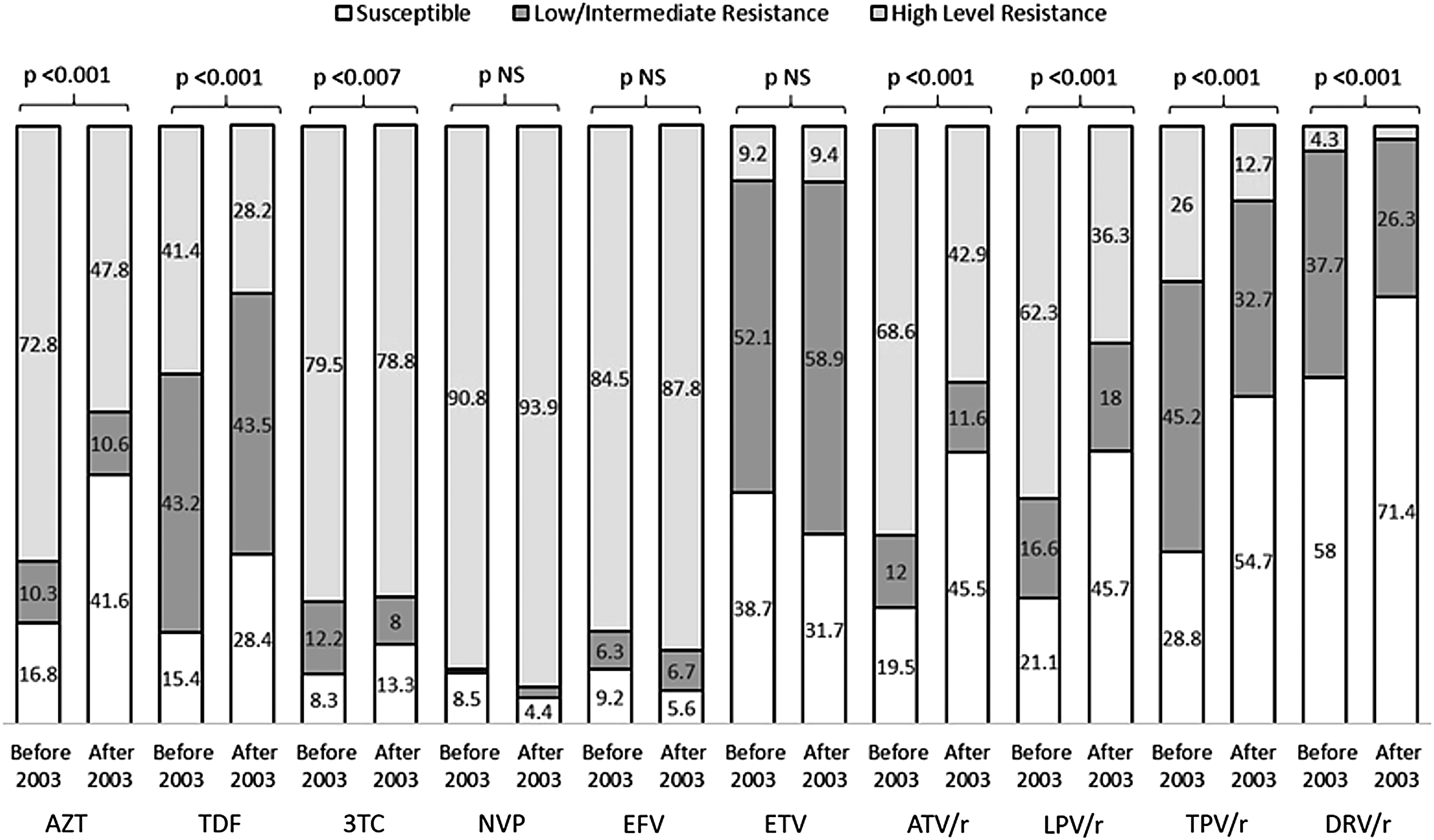
Distribution of patients according to the three viral drug-susceptibility categories in the HIV-genotypic resistance test for 10 sentinel antiretroviral agents. Categories are defined by the Stanford HIVdb system total penalty score: 0–14 (susceptible), 15–59 (low-level/intermediate resistance), and 60 or greater (high-level resistance). Comparison between the 488 patients starting antiretroviral therapy before mid-2003 and the 486 starting antiretroviral therapy after mid-2003. 3TC, lamivudine; ATV/r, ritonavir-boosted atazanavir; AZT, zidovudine; DRV/r, ritonavir-boosted darunavir; EFV, efavirenz; ETV, etravirine; LPV/r, ritonavir-boosted lopinavir; NVP, nevirapine; TDF, tenofovir disoproxil fumarate; TPV/r, ritonavir-boosted tipranavir.
A lower proportion of patients who started ART after mid-2003 used suboptimal ARV regimens (monotherapy, bitherapy with nRTIs, or nonboosted PI-containing regimens), zidovudine (or stavudine)-containing regimens, double PI-containing regimens, and a low barrier to resistance PI-containing regimens compared with patients who initiated earlier than 2003 (Table 1).
Comparison between the 488 patients starting antiretroviral therapy before mid-2003 and the 486 patients starting antiretroviral therapy after mid-2003.
Low barrier to resistance PI: indinavir, saquinavir, or nelfinavir.
AZT, zidovudine; d4T, stavudine; NNRTI, non-nucleoside reverse transcriptase inhibitor; nRTI, nucleoside analogue reverse transcriptase inhibitor; PI, protease inhibitor; TDF, tenofovir disoproxil fumarate.
Discussion
This study assessed the prevalence of heavily ARV-experienced patients harboring HIV with reduced susceptibility to diverse ARVs; a comparison between patients initiating ART before mid-2003 and those commencing therapy after mid-2003 was conducted. We chose this year as the cutoff point for the comparison because it was the year when the ART universal-access program of the Mexican MoH was implemented. Our results show that the proportion of patients with a genRT showing reduced viral susceptibility to zidovudine, tenofovir, and all first- and second- generation-studied PIs was significantly reduced over time. In contrast, the level of antiviral activity of NNRTIs and of cytidine analogue reverse transcription inhibitors (lamivudine and emtricitabine) remained stable, and a significant increase in the frequency of K65R mutations in the reverse transcriptase gene was observed. These temporal changes remained even after adjusting for potential confounders; that is, they were independent of the duration of previous ART exposure, level of viremia, and T-CD4 blood cell count at genotyping.
Several retrospective studies conducted in high-income settings have analyzed the trends of resistance in ART-exposed individuals. 1 –6 In a multicohort of 20,323 ART-experienced genotyped patients across seven countries in western Europe, HIV drug resistance mutations to all historical drug classes were found to decline in calendar years, and the proportion of cases exhausting the available drug options dropped from 32% in 2000 to 1% in 2008. 5 Authors of some of these surveys have suggested that these trends involved changes in the ART sequencing strategies as well as in the genetic barrier of the entire regimen; however, this explanation remains purely speculative, as no data on ART prescriptions in the study participants have been documented in any of these studies. In addition, a significant methodological flaw of these studies is the lack of control for possible selection biases, such as differential enrollment of more patients with a lower prior ART exposure and hence a lower likelihood of experiencing viral evolution (i.e., virological failure after first- or second-line regimens) as the year of recruitment increased. In our survey, we had complete information on the history of ARTs of every individual, which allowed us to make accurate associations between the type of drug regimens and selection of diverse RAMs. Furthermore, we minimized the selection bias by enrolling only heavily ARV-experienced patients and included a likely representative study sample, as it comprised individuals under routine care in HIV clinics throughout the country.
We documented significant changes in the first and subsequent regimens received by patients who started ART in and after 2003; the main changes were characterized by a drop in the use of mono/bitherapy and of regimens containing thymidine analogues (zidovudine and stavudine) as well as an increase in the use of ritonavir-boosted regimens, PI regimens with a higher barrier to resistance, and tenofovir-containing regimens. We postulate that these changes in ARV usage over time led to the changes in the rate of loss of viral susceptibility to various ARV drugs. Thus, a lower use of thymidine analogues led to a lower rate of selection of TAMs and, in turn, to an increase in viral susceptibility to zidovudine and tenofovir. Similarly, a lower use of nonboosted and of low barrier to resistance PIs led to a lower rate of selection of PI-mRAM and, in turn, to an increase in viral susceptibility to commonly used boosted PIs, such as atazanavir, lopinavir, and darunavir. Conversely, an increased use of tenofovir led to a rise in the rate of mutation K65R; however, this rate remained relatively low, perhaps because of the high genetic barrier to resistance of tenofovir. It is worth noting that this change in the frequency of K65R substitution had no effect on increasing the resistance score of tenofovir; indeed, this score actually diminished secondary to a significant drop in the relatively high rate of TAMs over time. Interestingly, the rate of cytidine analogues (lamivudine and emtricitabine) and of NNRTIs (efavirenz and nevirapine) RAM remained similar over time; this phenomenon has been observed in other settings as well 2,3,5 and could be explained by the stable high frequency of usage, throughout the study time period, of these ARV agents with low genetic barriers to resistance.
In brief, the decline in the loss of activity of certain ARV agents that are commonly used, such as tenofovir, and of ritonavir-boosted atazanavir, lopinavir, and darunavir, is driven by a decrease in the selection of the predominant HIV variants harboring RAMs, such as TAMs and PI-mRAMs. Our study provides empirical data to propose that these viral drug susceptibility changes are secondary, at least in part, to an increasing incorporation of drugs with higher genetic barriers to resistance in the armamentarium of Mexico's ART roll-out program. All patients in our study had a history of virological failure to several prior regimens, mostly because of a low adherence. Patients starting ART in recent years used drugs that are less likely to select for resistant viral strains, which led to a lower rate of patients with predominant HIV variants harboring RAMs emerging during these prolonged periods of persistent viremia under the selective pressure of diverse ARV agents. As we were unable to measure the length of these periods, we could not assess whether a shorter time of virological failure (more prompt switch to effective salvage therapy) was another determinant of the lower rate of RAMs detected among patients commencing ART after 2003; this is a limitation of our study.
This is the first epidemiological survey to report the trends in drug resistance in the HIV infection of heavily ARV-experienced patients treated through a national universal-access ART program in a middle-income country. These study data support a likely causal relationship between an increase in the use of ARV drugs with an increased barrier to resistance and a decline in the rate of nRTI- and PI-RAMs among individuals with a history of multiple failed ART regimens.
Footnotes
Acknowledgment
Funding for this work was provided by the Centro Nacional para la Prevención y el Control del VIH/SIDA (CENSIDA) for conduct of the study and collection of the data.
Author Disclosure Statement
J.J.C. has served as consultant on advisory boards for Janssen Pharmaceutical and Merck and reports personal honoraria from Stendhal, Bristol-Myers Squibb, and GlaxoSmithKline. S.L., M.A.T.M., M.O.F., C.L., P.A.S., H.R., and J.P.R. have nothing to declare.