
Abstract
The HIV care continuum is a tool that describes the quality of HIV care for people living with HIV and assesses the extent to which the goal of viral suppression has been achieved. In 2014, we conducted a retrospective cross-sectional study to assess the characteristics associated with three steps of the HIV continuum of care in Italy [i.e., most recent diagnoses, people diagnosed and in care who are on therapy, and people with viral load (VL) suppressed among those on therapy]. Among the 10,262 individuals diagnosed and linked to care, 9,810 (95.6%) were on therapy and among these 8,383 (85.7%) had VL suppressed. The comparison between people diagnosed in 2013 to those diagnosed before 2013 shows that they were more likely to be male [adjusted odds ratios (AOR) = 1.46; 95% confidence interval (95% CI): 1.18–1.79], <25 years of age (AOR = 7.59; 95% CI: 4.17–13.79), and born in Italy (AOR = 1.33; 95% CI: 1.09–1.62). Factors significantly associated with not being in therapy were as follows: age <35 years (AOR = 4.03; 95% CI: 2.50–6.51), age 35–55 years (AOR = 1.85; 95% CI: 1.19–2.87), being migrants (AOR = 1.25; 95% CI: 1.13–1.39), being men who have sex with men (MSM) (AOR = 1.54; 95% CI: 1.22–1.95), have been diagnosed in 2010–2012 (AOR = 4.51; 95% CI: 3.03–6.73), or before 2010 (AOR = 3.18; 95% CI: 2.41–4.21), and not had previous clinical AIDS (AOR = 8.24; 95% CI: 3.33–20.23), whereas factors significantly associated with not having VL suppressed were as follows: age <35 years (AOR = 1.56; 95% CI: 1.13–2.13) and age 35–55 years (AOR = 1.23; 95% CI: 1.10–1.38), being migrants (AOR = 1.38; 95% CI: 1.11–1.70), have been diagnosed in 2010–2012 (AOR = 1.34; 95% CI: 1.14–1.57), in 2013 (AOR = 4.35; 95% CI: 2.47–7.68), and not having had previous clinical AIDS (AOR = 0.74; 95% CI: 0.63–0.86). Despite this we observed significant disparities for young people, MSM, and migrants, overall in Italy the vast majority of people diagnosed with HIV and in care in 2013 received therapy and the percentage of people who are VL suppressed is near the Joint United Nations Programme on HIV/AIDS goal.
Introduction
T
UNAIDS (The Joint United Nations Programme on HIV/AIDS) has accepted the importance of this instrument and has set an important goal to be achieved by 2020: “90-90-90,” that is, 90% of diagnosed infections with HIV, 90% of people diagnosed on Antiretroviral Therapy (ART) and 90% of people in therapy achieve viral load (VL) suppression. 1 At European level, the European Centre for Disease Prevention and Control has clarified the definitions of the outcome of HIV Continuum of Care and collected the data from countries to build a European HIV Continuum of Care, 2 which is represented by four elements namely people living with HIV, those who know their HIV status, those who receive antiretroviral therapy, and those who are virally suppressed. Each of the outcomes of the Continuum of Care may be affected by numerous individual and systemic factors: patient sociodemographic characteristics (gender, age, nationality, and transmission mode), clinic conditions of patient (CD4 count and AIDS events), and HIV national guidelines or characteristics of an infectious diseases clinic (IDC). 3 Italy, has already reported its domestic HIV continuum of care 4 –6 but these studies did not evaluate the characteristics associated with the steps of the HIV continuum of care.
In 2014, we conducted a retrospective cross-sectional study to assess the characteristics of people diagnosed in 2013 and before 2013 and to evaluate factors associated to not being on ART and to not having a VL suppressed among people on ART.
Materials and Methods
In Italy, only specific disease clinics (mainly public infectious disease clinic, IDC) are authorized to offer free of charge monitoring, and treatment to all HIV-positive individuals. 7 People with HIV just diagnosed are invited to go to the IDC even if they did the tests in other screening facilities.
This study is part of the project “Characteristics of persons with HIV/AIDS in Italy-CARPHA” 4 : in the first phase of the project in 2013, we identified all IDCs in Italy and we estimated the percentage of people on ART and with VL suppressed using only simple aggregated data from each IDC. In this second phase, among the 173 IDCs previously identified we selected 12 IDCs.
The selection was carried out by dividing Italy into four macro-geographical areas (North, Center, South, and Islands). Next, for each macro-area, it was evaluated the functional urban area (FUA). FUA uses population density to identify urban cores and travel-to-work flows to identify the hinterlands whose labor market is highly integrated with the cores; it links the population density to the level of urbanization (rural and urban). 8 Then, three subareas for each macro-geographical-area (i.e., for Northern Italy: Milan, Modena, and Trento; for Central Italy: Rome, Perugia, and Massa-Carrara; for Southern Italy: Naples, Pescara, and Bisceglie; for Islands: Palermo, Trapani, and Sassari) were selected based on three different levels of FUA. Finally, within each subarea, if more than one IDC was present, we selected that one with more similar sociodemographic and behavioral characteristics (gender, age, nationality, and mode of transmission) resulted from the census conducted in 2012. These 12 IDCs are likely to be representative of all Italian IDCs, although opportunistically selected and not sampled. The selected IDCs were asked to collect through a standardized individual collection form data for each HIV-infected adult (i.e., ≥15 years) who had been linked to care in these IDCs between January 1, 2013 and December 31, 2013. We defined persons “linked to care” individuals who had at least one medical visit at any time after HIV diagnosis.
For each person in care during 2013, IDCs were asked to report individual data about the following: – Sociodemographic and behavioral characteristics: gender, age, country of birth, and transmission mode [heterosexual (HET), men who have sex with men (MSM), injecting drug user (IDU), other modes (i.e., mother-to-child transmission or blood transfusion)]; – HIV historical information: first test HIV positive, use of ART; – Clinical, immunological, and virological characteristics: lymphocytes CD4 measurements, VL measurements, AIDS-defining diseases, coinfection with hepatitis B virus (HBV), hepatitis C virus (HCV).
Outcomes
Three different outcomes were evaluated. As first outcome, we considered the HIV diagnosis in 2013 with the aim to identify the characteristics of those most recently diagnosed compared to those diagnosed before 2013.
The second outcome was the use of ART (defined as proportion ever diagnosed who ever initiated ART regardless of the number of days use) among those diagnosed and linked to care.
The third outcome, only among those on ART treatment, was having VL suppressed [defined as proportion ever on ART who were virally suppressed (≤50 copies/mL) at last visit]. The last two outcomes are two steps of the HIV Continuum of Care.
We estimated the percentage of these three outcomes also stratifying by the following variables: gender; age as of January 1, 2013; country of birth; transmission mode categorized as MSM, IDU, HET, or other modes [blood transfusion or perinatal exposure or unknown risk group (i.e., risk factor not reported nor identified)]; previous clinical AIDS; coinfection with HCV; coinfection with HBV.
To evaluate the independent association of the previously described variables with each of the three outcomes considered multiple mixed logistic regression models were used where the IDC was the cluster-sampling variable. Age was initially categorized in 10-years classes (i.e., 15–24, 25–34, etc.) and then grouped if some adjacent categories had similar effects. Adjusted odds ratios (AOR) were shown in the results section with 95% confidence intervals (95% CIs). Variables CD4 count and VL were not included in these analyses because considered outcomes of ART therapy. The analysis was performed using STATA software version 13. 9
Results
People included in the study were 10,262. The main characteristics of the people included in every IDC are shown in Table 1. Overall, the majority were male (71.0%), born in Italy (85.3%), aged ≥45 years (62.9%). The median age was 48 years (interquartile range (IQR) 41–53) and it significantly differed (p < .01) by gender [48 (IQR 41–53) and 46 (IQR 40–51) years] for men and women, respectively. The median age was different for people who were born in Italy and for foreign-born people; it was 49 years (IQR 43–53) and 41 years (IQR 35–47) for people who were born in Italy and for foreign-born respectively. Almost half of people foreign-born were from Africa (42.4%) and 32.5% from Latin America (data not shown).
ART, antiretroviral therapy; HBV, hepatitis B virus; HCV, hepatitis C virus; HET, heterosexual; IDU, injection drug use; IQR, interquartile range; MSM, men who have sex with men; VL, viral load.
There were 446 (4.3% of those in care; 95% CI: 3.7–5.2) people diagnosed in 2013 (Table 2); compared to those diagnosed before 2013, they were more likely to be male (AOR = 1.46; 95% CI: 1.18–1.79), <25 years of age (AOR = 7.59; 95% CI: 4.17–13.79), and born in Italy (AOR = 1.33; 95% CI: 1.09–1.62). Considering clinical characteristics, people diagnosed in 2013 were more likely not had previous clinical AIDS (AOR = 1.70; 95% CI: 1.19–2.41) and not had coinfection with HCV (AOR = 4.46; 95% CI: 2.11–9.39). We found a significant intraclass correlation of 0.03 (see footnote of Table 2) suggesting a slight residual effect of the IDC on this outcome.
Clinical center as a random effect estimate: 0.32 (95% CI: 0.18–0.57), intraclass correlation estimate: 0.03 (95% CI: 0.01–0.09).
95% CI, 95% confidence interval; AOR, adjusted odds ratios; NI, not included in the multiple logistic model.
Figure 1 shows an estimate of HIV Continuum of Care for Italy in 2013 based on the data from the 12 IDCs participating in this study. Among the 10,262 individuals diagnosed and linked to care, 9,810 (95.6%; 95% CI: 94.5–96.4) were on ART and among these 8,383 (85.7% of those on ART; 95% CI: 83.4–87.3) had VL suppressed (29 did not have VL information).
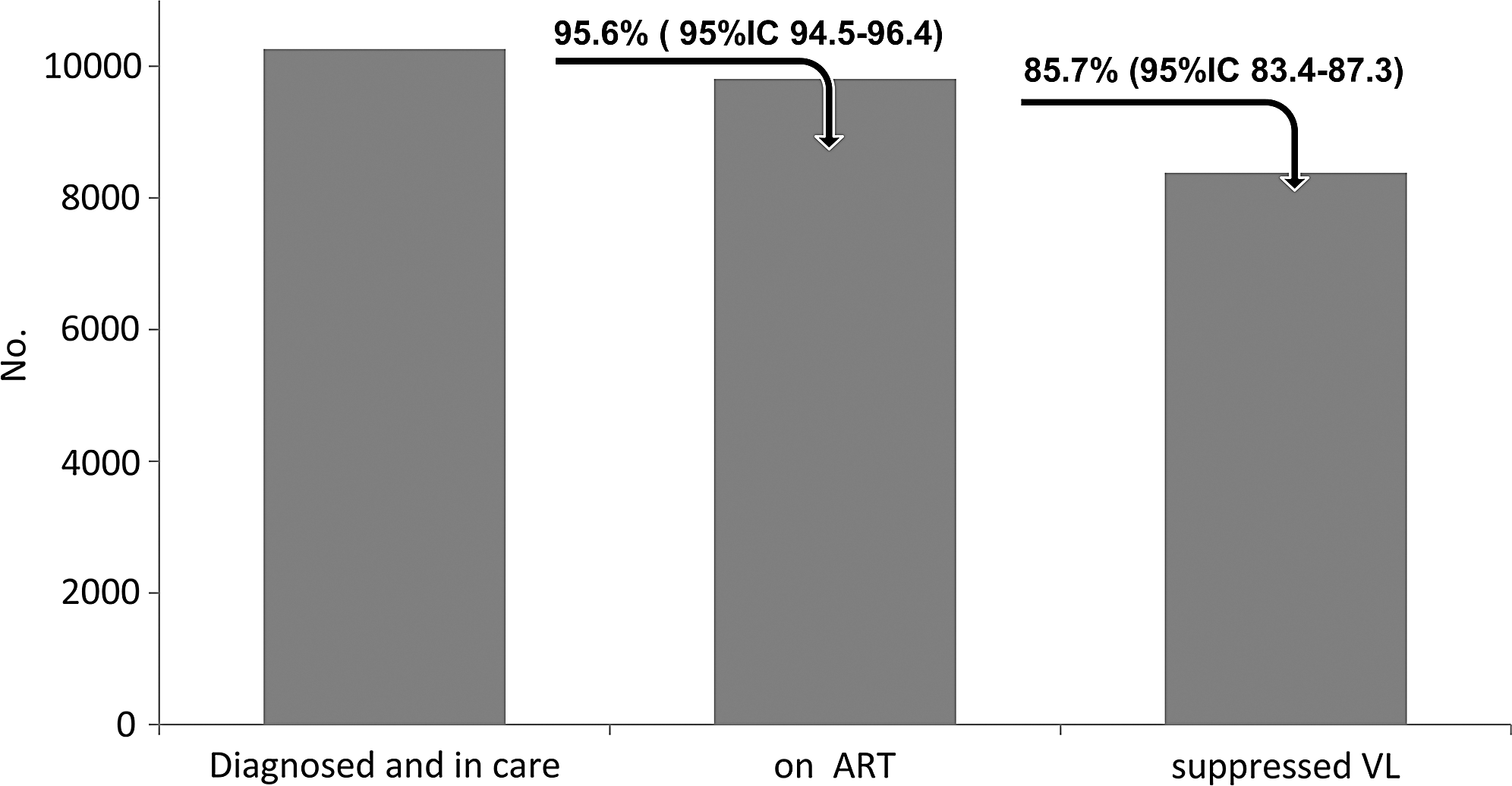
HIV continuum of care among 12 public infectious diseases clinics (10,262 people), Italy 2013. ART, antiretroviral therapy; VL, viral load.
Regarding ART treatment, there were 452 persons (4.4%; 95% CI: 3.6–5.5) not being in ART (Table 3); at the univariate analysis they were significantly more likely to be aged <35 years (p < .01), foreign-born people (p < .01), being MSM (7.7%; p < .01), not had previous clinical AIDS (p < .01), and not having HCV coinfection (p < .01).
Clinical center as a random effect estimate: 0.41 (95% CI: 0.21–0.81), intraclass correlation estimate: 0.05 (95% CI: 0.01–0.16).
NE, not estimable.
At the multivariate analysis, factors significantly and independently associated with not being in ART were as follows: age <35 years (AOR = 4.03; 95% CI: 2.50–6.51), age 35–55 years (AOR = 1.85; 95% CI: 1.19–2.87), being foreign-born people (AOR = 1.25; 95% CI: 1.13–1.39), being MSM (AOR = 1.54; 95% CI: 1.22–1.95), have been diagnosed in 2010–2012 (AOR = 4.51; 95% CI: 3.03–6.73), or before 2010 (AOR = 3.18; 95% CI: 2.41–4.21), and not had previous clinical AIDS (AOR = 8.24; 95% CI: 3.33–20.23) (Table 3). We found a significant intraclass correlation of 0.05 (see footnote of Table 3) suggesting again a slight residual effect of the IDC on this outcome.
Regarding VL suppression among those on ART, overall there were 1,398 (14.3%; 95% CI: 12.7–16.1) persons not being VL suppressed (Table 4); at the univariate analysis, persons who were not VL suppressed were significantly more likely to be aged <35 years (p < .01), foreign-born people (p < .01), who acquired the HIV infection through injecting drugs (p < .01), who were diagnosed in 2013 (p < .01), and who had previous clinical AIDS (p < .01).
Clinical center as a random effect estimate: 0.97 (95% CI: 0.56–1.68), intraclass correlation estimate: 0.22 (95% CI: 0.09–0.46).
At the multivariate analysis, factors significantly associated with not having VL suppressed were as follows: age <35 years (AOR = 1.56; 95% CI: 1.13–2.13) and age 35–55 years (AOR = 1.23; 95% CI: 1.10–1.38), being foreign-born people (AOR = 1.38; 95% CI: 1.11–1.70), have been diagnosed in 2010–2012 (AOR = 1.34; 95% CI: 1.14–1.57), have been diagnosed in 2013 (AOR = 4.35; 95% CI: 2.47–7.68), and not had previous clinical AIDS (AOR = 0.74; 95% CI: 0.63–0.86) (Table 4). We found a significant intraclass correlation of 0.22 (see footnote of Table 4) suggesting a strong residual effect of the IDC on this outcome.
Discussion
In this study, we provided estimates for Italy for three important findings of the epidemiology of HIV infection, that is, the characteristics of the most recent diagnoses, percentage and characteristics of people diagnosed and in care who are on ART, and percentage and characteristics of those with VL suppressed among those on ART. These estimates were obtained from 12 IDCs and were selected in a way that they can be considered representative (in terms of similarity by age, gender, nationality, mode of transmission, geographical area, and population density) of overall HIV-positive people diagnosed and in care in Italy. The people diagnosed and in care obtained from 12 IDCs represent the 10.9% of all people diagnosed and in care in Italy in 2012. 4
Regarding the most recent diagnoses, the comparison between people diagnosed in 2013 and before 2013 highlights that the most recent diagnoses were more likely to be among young men born in Italy and not HCV coinfected. This is consistent with data from Italian HIV and AIDS surveillance system in 2013 that point out that a large proportion of new diagnosis were among young people (53.7% people under 40 years), among Italians (76.0%). 10
Initially, the HIV continuum of care was proposed as a three-step target with the 90-90-90 goal considered as the success of screening and treatment for a country. 1 However, these steps were further subdivided up to five steps. 1 Data from this study provide estimates for two of the outcomes (i.e., being on ART among those diagnosed and in care and having VL suppressed among those on ART). Thus, our estimates are not always directly comparable with other data because the definitions did not overlap. Nevertheless, the data could suggest that Italy in 2013 has approached the suggested target (i.e., 90-90-90) for what concerns being on ART, whereas for what concerns having VL suppressed, is still 4.3% lower than the 90% UNAIDS target. This lack could be caused by multiple factors, for example, comorbidity conditions, ART adherence, daily life activities, and distance to clinics and shows the need to improve the attention to the people in care. 11 Although we used a strict definition of “viral suppression” (i.e., ≤50 copies/mL), often lower than the cutoff used in some other countries, the percentage of people on ART and with VL suppressed observed in our study is sometimes higher than that reported in other Western European countries (i.e., United Kingdom: 90% and 90.0% in 2013 using VL ≤200; France: 81% and 86% in 2010 using VL ≤50 copies; The Netherlands: 87% and 90% in 2012 with VL ≤100 copies; and Belgium: 83% and 69% in 2013 with VL ≤50 copies). 12 –15
Neverthless, our study revealed that success at each outcome of the Continuum might differ between population groups; thus, different strategies might be needed in different groups to achieve optimal improvement at each step of the Continuum of Care. In this study, when adjusting for other characteristics, we found that people under 55 years of age have a significantly higher probability of not being on ART and not being virally suppressed compared to older people. Similar results have been reported elsewhere 16 ; one possible explanation is that in 2013 younger HIV-positive individuals, who were more recently diagnosed, had on average better clinical, immunological, and virological condition, and therefore they were still waiting to start ART (based on the 2013 Italian guidelines, which suggested to begin antiretroviral treatment when a person's CD4 cell count falls below 350 cells/mL). 17
MSM experienced higher probability of not being on ART. This is reported also by other European studies 18,19 who found that MSM had the poorest percentages on all the outcomes of the HIV Continuum of Care. Furthermore, data from the Italian HIV surveillance system show that in recent years a high proportion of new diagnoses occur among MSM. Therefore, due to recent diagnosis, this population could not be yet on HAART, although this effect for MSM was also estimated when adjusting for year of diagnosis. 10
Finally, it is necessary to underline that foreign people show a higher probability of not being on ART compared to Italians as already reported in other studies, 19 –21 highlighting difficulties of access to care for this particular population. Second, in our study, we have no information about HIV diagnosed people and not in care but we can refer to other Italian estimates. 22
In conclusion, our study shows that overall in Italy the vast majority of people diagnosed with HIV and in care in 2013 received ART and the percentage of people who are VL suppressed is near the UNAIDS goals. However, significant disparities were observed among young people, MSM, and migrants.
Footnotes
Acknowledgments
This study received financial support from the Ministry of Health, Ricerca Finalizzata 2009 to 2010 (grant no. RF-2009-1505025). Sources of support: Collaborations: The CARPHA Study Group: Claudio Paternoster (Ospedale S. Chiara, Trento); Giuliano Rizzardini, Chiara Atzori (Ospedale Luigi Sacco, Milano); Cristina Mussini, Vanni Borghi (Policlinico, Modena); Maurilio Chimenti (Ospedale Civico, Massa Carrara); Franco Baldelli, Daniela Francisci (Ospedale S. Maria della Misericordia, Perugia); Andrea Antinori, Alberto Giannetti (INMI L. Spallanzani, Roma); Guglielmo Borgia, Giovanni Di Filippo (AOU Federico II, Dipartimento Malattie Infettive, Napoli); Giustino Parruti, Paola Di Stefano (Ospedale S. Spirito, Pescara); Tommaso Fontana, Ruggero Losappio (Ospedale Vittorio Emanuele II, Bisceglie); Maria Stella Mura, Giordano Madeddu (AOU, Dipartimento di Malattie Infettive, Sassari); Enzo Maria Farinella, Cecilia Occhino (Ospedale Cervello, Palermo); Vincenzo Portelli (Ospedale S. Antonio Abate, Trapani).
Author Disclosure Statement
No conflicting financial interests exist. The authors declare that they have no affiliation with any organization whose financial interest may be affected by material in the article or that may potentially bias it.