
Abstract
While children's exposure to environmental lead in the United States has decreased, areas of elevated levels remain. Because lead exposure is a risk factor for developmental delays, it should be considered when studying neurodevelopmental effects of in utero antiretroviral medication (ARV) exposure in the growing population of perinatally HIV-exposed, uninfected (PHEU) children. We compared blood lead levels (BPb) in PHEU children enrolled in the Surveillance Monitoring of ART Toxicities (SMARTT) Study to U.S. children, assessed associations with neurodevelopment, and explored whether associations between in utero ARV and neurodevelopment are modified by BPb. Prevalence of elevated BPb (≥5 μg/dl) at ages 1–2 years was calculated by year and race/ethnicity and compared to that for children in the National Health and Nutrition Examination Survey (NHANES 2002–2010). Associations between elevated BPb and neurodevelopment at 1 and 3 years were assessed. Associations between ARVs (tenofovir disoproxil fumarate [TDF]; atazanavir) and neurodevelopment were evaluated within BPb level (≥5 μg/dl vs. <5 μg/dl). Mean BPb in SMARTT decreased from 5.9 to 2.7 μg/dl between 1998 and 2014; prevalence of elevated BPb decreased from 50% to 4%. Both were consistently higher than in NHANES. Elevated BPb was associated with cognitive delay at age 3 (adjusted odds ratio: 1.64; 95% confidence interval: 0.95–2.90). At age 1, TDF was associated with delay only among those with elevated BPb. PHEU children more often had elevated BPb than the general U.S. pediatric population. Exposure to environmental lead is one of several factors that may place these children at higher risk for neurodevelopmental delay.
Introduction
L
Federal, state, and local governments in the United States have instituted measures to reduce lead exposure, 13 including the introduction of unleaded gasoline, abatement of lead-based paint from residences, and increased screening. These actions have led to a striking decline in blood lead level; however, elevated levels remain high in some areas, particularly urban neighborhoods with older housing. 14
Another long-standing source of lead exposure is drinking water. Cost-cutting changes in water sources, repairs to aging distribution pipes, and chemical treatment, all can result in increased lead concentration. In Greater Flint, Michigan, the resulting deleterious effects include a doubling of blood lead concentrations above 5 μg/dl in children between 2013 and 2015; the rise is especially high among children living in disadvantaged neighborhoods. 15 While the crisis in Flint is receiving the most attention, other communities across the United States are experiencing similar increases. 16
The SMARTT (Surveillance Monitoring for ART Toxicities Study in HIV-uninfected Children Born to HIV-infected Women) cohort of the Pediatric HIV/AIDS Cohort Study (PHACS) is an ongoing multisite U.S.-based study of children perinatally exposed to but uninfected with HIV, and is examining the effects of maternal HIV infection and in utero exposure to antiretroviral medications (ARVs) on biomedical, neurodevelopmental, and behavioral outcomes in these children. Since endpoints associated with lead exposure are also key outcomes for SMARTT, and because pockets of elevated lead remain in areas that include SMARTT site locations, it is important to determine the prevalence of elevated blood lead level among children in SMARTT. The possible role of lead as an effect modifier of the association between in utero exposure to ARVs and developmental function is also an important association to investigate. For instance, exposure to both elevated blood lead and to a particular ARV might have a greater than additive effect than exposure to either alone. 17
We determined the prevalence of elevated blood lead level (BPb) among children in SMARTT, compared this prevalence to that in a nationally representative sample, and estimated the association between BPb and neurodevelopmental function in early childhood. We also explored whether the association between in utero ARV and neurodevelopmental function varies by BPb.
Materials and Methods
Study population
SMARTT is a prospective cohort study designed to evaluate the safety of in utero exposure to HIV and ARVs. All children are HIV-exposed but uninfected. Enrollment began in 2007 at 22 PHACS clinical research sites in the United States, including Puerto Rico. Children were enrolled in two cohorts: the Static cohort enrolled children ≤12 years old and closed to enrollment in 2009; enrollment of newborns and their HIV-infected mothers in the Dynamic cohort is ongoing. The Institutional Review Board at each site and at the Harvard T. H. Chan School of Public Health approved the study. Parents provide written informed consent for their own and their child's participation.
At entry, information is collected on ARVs taken during pregnancy as well as demographic and maternal information. Annual study visits include updating demographic information, medical chart abstraction, and physical examinations. Assessments of neurocognitive function are conducted at specific ages. For these analyses, only children whose biological mothers were enrolled as caregivers (98.7%) were included, to reduce potential confounding by caregiver status.
Comparison with nationally representative population
Published summary data (race/ethnicity; proportion [95% confidence interval (CI)] with BPb ≥5 μg/dl; testing year) for children in the 2002–2010 National Health and Nutrition Examination Survey (NHANES) 14 aged 1–2 years were included to provide a nationally representative comparison. NHANES race/ethnicity-stratified prevalence estimates were restricted to 2007–2010; therefore, our race/ethnicity-specific comparisons between the SMARTT and NHANES cohorts were restricted to this period.
Blood lead levels
In SMARTT, BPb obtained between the ages of 1 and 3 years as part of standard of care or local guidelines are abstracted from the medical chart when available. Otherwise, measurements are obtained through real-time testing at local laboratories at age 3 years by testers blind to participants' neurodevelopmental function test results.
In these analyses, BPb was considered both as a continuous and a dichotomous (elevated vs. not elevated; ≥5 μg/dl vs. <5 μg/dl) measure.
Outcomes
Neurodevelopmental function at 1 year of age was evaluated with the Bayley Scales of Infant and Toddler Development-Third Edition (Bayley-III), 18 which is normed for infants and young children and provides standardized measures of development in five domains: cognition, language, motor skills, social–emotional function, and adaptive behavior. We examined continuous scores as well as impaired performance (>1 standard deviation below population norm).
At 3 years of age, developmental function was assessed with the Bayley Screening Test (Bayley Screen), 19 which includes a subset of items from the Bayley-III with the domains of cognition, receptive communication, expressive communication, and fine and gross motor development. Children are classified as “at risk,” “emerging,” (some risk) or “competent” in each domain. The Bayley Screen does not provide continuous scores. In this analysis, we compared “at risk” or “emerging” performance to “competent.” We also compared “at risk” performance to “emerging” or “competent” in secondary analyses.
The Bayley-III and Bayley Screen are available only in English, and were not administered to children in our two Puerto Rican sites. The assessments were administered to children who had sufficient English language exposure and whose mothers were sufficiently bilingual to answer standardized questions. These assessments were administered according to standardized procedures by experienced psychologists. Invalid results were reviewed by psychologists and all scores deemed invalid were excluded from analyses.
Covariates
Several factors were considered as potential confounders of the association between BPb and neurodevelopmental function: sex; race; ethnicity; maternal IQ (evaluated with the Wechsler Abbreviated Scale of Intelligence 20 ); maternal education, primary language, living arrangement, and living situation; household income; geographic region; prenatal tobacco exposure; postnatal tobacco exposure within the home; age at the developmental evaluation; and help from others caring for the child. A subset of these factors (education, region, age at evaluation, income, prenatal tobacco exposure) and maternal drug (marijuana, cocaine, heroin, opium, PCP [phencyclidine] or MDMA [3,4-methylenedioxy-methamphetamine]) and alcohol use during pregnancy were considered as potential confounders in the analysis examining BPb as a modifier of the association between ARV and neurodevelopmental function. Potential confounders were evaluated in directed acyclic graphs (DAGs) using DAGitty 21 to examine the causal relationships between variables and to identify a minimally sufficient subset to include in multivariable analyses.
In utero ARVs
In the evaluation of BPb as an effect modifier, we considered two ARVs identified in previous SMARTT analyses as possibly influencing early childhood outcomes: atazanavir (ATV) 22 –24 and tenofovir disoproxil fumarate (TDF). 25
Statistical analysis
We calculated mean and median BPb for SMARTT children with results obtained between 1 and 2 years of age by calendar year, and proportions of children with elevated BPb by calendar year, geographic location, and race/ethnicity. Graphical summaries were used to present average BPb and percent with elevated BPb by calendar year, and to compare elevated BPb by calendar year and race/ethnicity for children in SMARTT and NHANES. Changes over time in mean BPb and in the proportion with elevated BPb were evaluated with a linear test for trend and the Cochran–Armitage test for trend, respectively.
For the evaluation of BPb and neurodevelopmental function and for the effect modification analysis, we included BPb obtained between 9 months of age and 3 months after the developmental assessment (Bayley-III or Bayley Screen). If multiple BPb were available for a child over the particular interval of interest, then the maximum BPb in that interval was used.
General linear and logistic regression models were used to evaluate associations of BPb with continuous and binary neurodevelopmental outcomes, respectively. Potential confounders were added individually to the univariable model, and variables that changed the effect estimate of BPb by >10% were kept in the final multivariable model. We decided a priori to include maternal education, age at developmental assessment, and geographic region in all models. For covariates with >5% missing data, missing value indicators were created.
To explore effect modification by BPb on associations between in utero ARV and developmental function, we first evaluated associations stratified by BPb (≥5/<5 μg/dl) using two-sample t-tests or chi-square/Fisher's exact tests. Multivariable regression models were then fitted, including interaction terms between BPb and each ARV, adjusting for potential confounders as described above.
Several sensitivity analyses were conducted. First, because maternal IQ was missing for ∼20% of participants, primary analyses included maternal education as a proxy for IQ. To assess the extent of residual confounding, we conducted a sensitivity analysis in the subset of participants for whom maternal IQ was available. In this subset, we compared the effect estimates obtained in multivariable models adjusting only for maternal education to those adjusting for maternal education and maternal IQ. Second, because some SMARTT children receive their primary care at clinics not associated with the SMARTT research clinics, their primary care charts are often not available. Also, some states do not require routine blood lead testing. We therefore assessed the effect of lack of BPb results in medical charts on the association between BPb and developmental function by excluding sites where medical chart results were available for fewer than (a) 60% and (b) 75% of participants. Third, for the NHANES comparison, we restricted the SMARTT group to sites where ≥75% had BPb from medical charts.
Results
As of January 2015, 3,301 children had enrolled in SMARTT. Of these, 1,431 (43.5%) had BPb obtained between 1 and 2 years of age in their medical chart. There were no BPb results in the medical charts of children from the Puerto Rican sites. Years of tests ranged from 1996 to 2010, reflecting the wide age range of children at enrollment (from newborns in Dynamic to children ≤12 years in Static).
There was a significant decrease in mean BPb (and in prevalence of elevated BPb by testing year (Fig. 1a, b, respectively). This decrease was evident across all four geographic regions (data not shown). Children from research sites in the Midwest had the highest prevalence of elevated BPb (20% 5–10, 6%> 10 μg/dl), followed by those in the Northeast (14% 5–10, 3%> 10 μg/dl), South (12% 5–10, 1%> 10 μg/dl), and West (8% 5–10, 1%> 10 μg/dl).
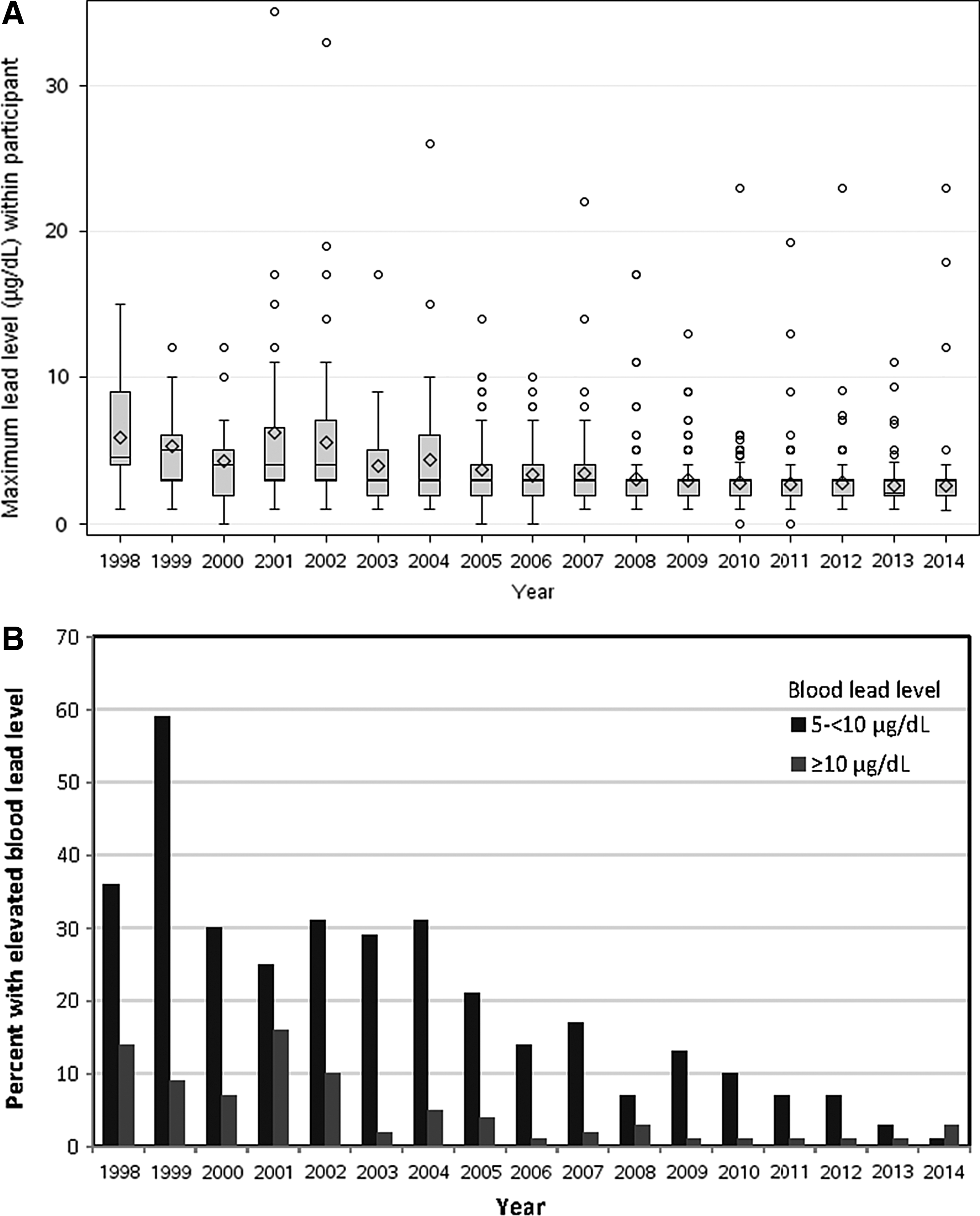
Trends in blood lead levels among 1,425 children aged 1–2 years enrolled in the PHACS SMARTT Study, from 1998 to 2014.
SMARTT children had a substantially higher prevalence of elevated BPb than children in NHANES, a difference consistent across all years (Supplementary Fig. S1; Supplementary Data are available online at
Background characteristics for children included in the neurodevelopmental function analyses are summarized in Table 1. There were 546 children with a Bayley-III at one year of age who had a BPb between 9 months of age and up to 3 months after the Bayley-III; the mean (range) time from blood lead testing to the Bayley-III was 0.8 months (−2.9, 11.5). Twenty-seven children (4.9%) had elevated BPb. There were 634 children with a Bayley Screen at 3 years of age and a BPb between 9 months of age and up to 3 months after the Bayley Screen; 85% of results were abstracted from medical charts and 15% from real-time testing at age 3 years. The mean (range) time from blood lead testing to the Bayley Screen was 16.2 months (−1.4, 34.0). Sixty-nine children (11%) had elevated BPb.
Chi-square test for categorical variables; Wilcoxon rank-sum test for continuous variables.
Northeast: New York, New Jersey, Pennsylvania; Midwest: Illinois; South: Alabama, Tennessee, Florida, Texas, Louisiana, Maryland; West: Colorado, California.
The following variables had missing observations: Bayley-III: race (9), maternal education (1), anyone else care for child (1), smoke exposure during pregnancy (20), smoke exposure in home (80), PI during pregnancy (2), ATV during pregnancy (2), TDF during pregnancy (2); Bayley Screen: race (18), Hispanic ethnicity (1), maternal education (3), live with partner (5), anyone else care for child (4), living situation (4), smoke exposure during pregnancy (37), smoke exposure at home (10), PI during pregnancy (4), ATV during pregnancy (4), TDF during pregnancy (4).
FSIQ, full-scale IQ; PI, protease inhibitor; ATV, atazanavir; TDF, tenofovir disoproxil fumarate; SD, standard deviation.
BPb and neurodevelopmental function
There were no statistically significant associations observed between continuous or elevated BPb and any Bayley-III domain at age 1 year in either unadjusted or adjusted analyses (Table 2). These findings persisted in all sensitivity analyses (Supplementary Table S1).
Models for all domains adjust for age at time of Bayley-III evaluation, maternal education, living situation, and region. Models also adjust for these additional covariates depending on domain: race (all domains but social–emotional), child exposure to smoking at home (language, social–emotional, general-adaptive), maternal primary language (language, motor, general-adaptive), and household annual income (motor).
CI, confidence interval.
Odds ratios (ORs) and 95% CI from univariable and multivariable models for developmental function at age 3 years are presented in Table 3. After adjusting for potential confounders, there was a 64% increased odds of delayed development in the cognitive domain among children with elevated BPb compared to children without elevated BPb (adjusted OR [aOR]: 1.64; 95% CI: 0.95–2.90). In sensitivity analyses excluding sites where results were available for ≤60% or ≤75% of participants, this association was somewhat attenuated (aOR: 1.55 and 1.46, respectively). We observed decreased odds of delayed fine motor function with elevated BPb that was statistically significant in these sensitivity analyses (aOR: 0.41 and 0.25, respectively). Sensitivity analyses adding maternal IQ did not change the estimated associations for any domains (Supplementary Table S2). With a cutoff of “at risk” versus “emerging”/“competent” for the Bayley Screen, no associations were observed for any domain (data not shown). There were no associations observed between continuous BPb and the Bayley Screen domains, with the exception of reduced odds of delayed fine motor function with increasing BPb (aOR: 0.90; 95% CI: 0.80–0.98).
OR for emerging/at risk performance (vs. competent) for subjects with lead level ≥5 μg/dl versus <5 μg/dl.
Models for all domains adjust for age at time of Bayley Screen evaluation, maternal education, race, region. Models also adjust for these additional covariates depending on domain: maternal primary language (receptive communication), household annual income, and sex (receptive communication, expressive communication).
OR, odds ratio.
Effect modification
There was no effect modification by BPb on the associations between in utero ATV exposure and any Bayley-III domain. There was evidence of effect modification in the association between TDF and the cognitive domain of the Bayley-III (Fig. 2); for children in the elevated lead category, TDF exposure was associated with an ∼11-point lower score (adjusted means = 99.2 vs. 110.8, p = .03), while there was no association in the lower lead category (adjusted means = 103.1 vs. 102.6, p = .68; interaction p = .03). There was no evidence of effect modification by BPb on the associations of ATV or TDF exposure with any of the Bayley Screen domains.

Adjusted differences in mean Bayley-III domain scores for children with versus without in utero TDF exposure, by blood lead level. Of 24 participants with lead level ≥5 μg/dl, 11 (46%) were exposed in utero to TDF; of 514 with lead level <5 μg/dl, 248 (48%) were exposed in utero to TDF. (Eight children were excluded because they were not exposed to or were missing information on ARVs during pregnancy.) Models for all domains adjust for age at Bayley-III evaluation, maternal education, and region. Models adjust for these additional covariates depending on domain: maternal drug use during pregnancy (all domains except for motor), household annual income (cognition, language, general-adaptive), p maternal use of tobacco during pregnancy (all domains except for motor). ARVs, antiretroviral medications; TDF, tenofovir disoproxil fumarate.
Discussion
The prevalence of elevated BPb decreased over time in perinatally HIV-exposed, uninfected children in SMARTT, a decrease also observed nationally. However, children in SMARTT were more likely to have elevated BPb than children in the NHANES cohort. This elevated prevalence persisted after accounting for differences in race and ethnicity between the cohorts. The higher prevalence likely reflects the fact that most SMARTT children live in low-income households predominantly in urban northeastern and midwestern cities.
Children with elevated BPb were more likely than children with lower levels to have delayed cognitive function at 3 years of age; we did not observe an association for 1-year olds. One year of age might not be the period during which lead exposure is harmful to neurodevelopmental function. 26,27 There are few studies assessing the effect of lead exposure and development function in this age group. One study found a harmful effect of prenatal, but not postnatal, BPb on cognitive function at 1 year of age. 28 Another identified more problematic behaviors in 1-year olds with BPb ≥10 μg/dl 4 . At 1 year of age, most children may not be sufficiently mobile to encounter lead in their environment, or may not yet have been exposed for a long enough period of time. We do not routinely collect BPb longitudinally in SMARTT and do not know whether children with elevated BPb at 1 year of age continued to have elevated levels in later years; therefore, we cannot distinguish between these potential explanations.
The association between elevated BPb and better fine motor skills at age 3 years was unexpected and is contrary to observations in previous studies. 29,30 This association may be explained by considering that children who have stronger fine motor skills may be more mobile or better able to pick up and ingest paint chips and other lead-contaminated dust particles.
We observed some evidence of effect modification by BPb on the association between in utero TDF exposure and cognitive function in 1-year olds, with an apparently harmful effect of TDF only among children who also had elevated BPb. This observation should be reexamined in studies with larger sample sizes to determine whether it can be replicated and to explore possible mechanisms. For instance, emtricitabine (FTC) is often given in combination with TDF. We found a similar association as for TDF when examining the effect of BPb on the association between FTC and developmental function (data not shown). It will be important to examine whether this association is due to TDF, FTC, a combination of both, or perhaps even due to other drugs given in the absence of FTC and TDF.
It is worthwhile to again point out that while we did observe possible effect modification between BPb and in utero TDF exposure in 1-year olds, we did not observe a main effect of BPb at this age. One possibility is that, as mentioned above, the duration of exposure to lead at this age is not sufficient for its effect on cognitive function to be observed, particularly if the association is a modest one. However, in the situation where two potential harmful agents are present, their combined effect is stronger, and since we had a continuous measure of neurodevelopmental function at age 1 year, we could observe this increased risk. At age 3 years, however, while we did observe a main effect of lead on cognitive function, we had insufficient power to detect potential effect modification since we were limited by our categorical measure of neurodevelopmental function and the fact that the measure at age 3 may be a less sensitive screening measure.
Our study's strengths include its large sample size, the large number of years over which we measured the BPb of children in SMARTT, and our measurement of important confounders. Our study has several limitations. It was underpowered to test for effect modification, and there may be interactions between BPb and ARVs that we were not able to detect. Lead testing was not performed at a central laboratory, but at the local laboratories of our clinical research sites. Since uniform testing was not undertaken, we expect that this would contribute to increased variability in test results and nondifferential exposure misclassification. While we observed an association between BPb and cognitive function at age 3, the association was not statistically significant. We were not able to evaluate cognitive function at age 3 as a continuous measure, and the Bayley Screen may not have been the ideal evaluation with which to detect a modest association between BPb and cognitive development. One important unmeasured confounder is the quality of the home environment. 31 However, adjustment for maternal IQ, one of the most important predictors of child IQ, did not materially affect our effect estimates. Finally, the possibility for selection bias exists since there is evidence that even in states where lead testing is required, some pediatricians preferentially test children who they perceive to be at high risk. 32 The most likely scenario would be that pediatricians screen children who manifest neurodevelopmental delay and live in housing perceived as being more likely to contain lead. Indeed, children included in our analyses had lower Bayley-III and Bayley Screen scores than those excluded (data not shown), and were less likely to live in homes their families owned. Therefore, selection bias is a possibility. However, our ability to adjust for living situation in our analyses reduces the impact that such selection bias may have had.
Conclusions
The long-term evaluation of deleterious effects of in utero HIV and ARV exposures on the health outcomes of perinatally HIV-exposed, uninfected children is an important undertaking. Consideration of other risk factors must be incorporated to ensure accurate and precise effect estimates. Many of these children live in low-income households and are parented by mothers who have to manage the emotional, cognitive, and physical challenges that accompany HIV infection. They are therefore at potentially elevated risk for developmental, behavioral, or emotional impairment. Their relatively high exposure to environmental lead is another factor that might negatively affect their developmental health. Given the disadvantaged living environments of children affected by HIV, and the recently reported exposures to high levels of lead in drinking water in communities across the United States, increased vigilance in screening for environmental lead exposure should be a public health priority.
Footnotes
Acknowledgments
We thank the children and families for their participation in PHACS, and the individuals and institutions involved in the conduct of PHACS. The study was supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development with cofunding from the National Institute on Drug Abuse, the National Institute of Allergy and Infectious Diseases, the Office of AIDS Research, the National Institute of Mental Health, the National Institute of Neurological Disorders and Stroke, the National Institute on Deafness and Other Communication Disorders, the National Heart Lung and Blood Institute, the National Institute of Dental and Craniofacial Research, and the National Institute on Alcohol Abuse and Alcoholism, through cooperative agreements with the Harvard T.H. Chan School of Public Health (HD052102) (principal investigator: George Seage; project director: Julie Alperen) and the Tulane University School of Medicine (HD052104) (principal investigator: Russell Van Dyke; co-principal investigators: Kenneth Rich, Ellen Chadwick; project director: Patrick Davis). Data management services were provided by Frontier Science and Technology Research Foundation (PI: Suzanne Siminski), and regulatory services and logistical support were provided by Westat, Inc (PI: Julie Davidson). Role of the sponsors: representatives of the National Institutes of Health were part of the study team, and therefore, the sponsor was involved in the design and conduct of the study; in the interpretation of the data; in the review and approval of the manuscript; and decision to submit the manuscript for publication. Note: the conclusions and opinions expressed in this article are those of the authors and do not necessarily reflect those of the National Institutes of Health or U.S. Department of Health and Human Services.
The following institutions, clinical site investigators, and staff participated in conducting PHACS SMARTT in 2015, in alphabetical order: Ann and Robert H. Lurie Children's Hospital of Chicago: Ram Yogev, Margaret Ann Sanders, Kathleen Malee, Scott Hunter; Baylor College of Medicine: William Shearer, Mary Paul, Norma Cooper, Lynnette Harris; Bronx Lebanon Hospital Center: Murli Purswani, Emma Stuard, Anna Cintron; Children's Diagnostic and Treatment Center: Ana Puga, Dia Cooley, Patricia A. Garvie, James Blood; New York University School of Medicine: William Borkowsky, Sandra Deygoo,Marsha Vasserman; Rutgers—New Jersey Medical School: Arry Dieudonne, Linda Bettica; St. Jude Children's Research Hospital: Katherine Knapp, Kim Allison, Megan Wilkins; San Juan Hospital/Department of Pediatrics: Midnela Acevedo-Flores, Lourdes Angeli-Nieves, Vivian Olivera; SUNY Downstate Medical Center: Stephan Kohlhoff, Ava Dennie, Susan Bewley; Tulane University School of Medicine: Russell Van Dyke, Karen Craig, Patricia Sirois; University of Alabama, Birmingham: Marilyn Crain, Paige Hickman, Dan Marullo; University of California, San Diego: Stephen A. Spector, Kim Norris, Sharon Nichols; University of Colorado, Denver: Elizabeth McFarland, Carrie Chambers, Jenna Wallace, Emily Barr; University of Florida, Center for HIV/AIDS Research, Education and Service: Mobeen Rathore, Kristi Stowers, Saniyyah Mahmoudi, Ann Usitalo; University of Illinois, Chicago: Karen Hayani, Kenneth Rich, Lourdes Richardson, Renee Smith; University of Miami: Gwendolyn Scott, Sady Dominguez, Anai Cuadra; University of Southern California: Toni Frederick, Mariam Davtyan, Guadalupe Morales-Avendano; University of Puerto Rico School of Medicine, Medical Science Campus: Zoe M. Rodriguez, Ibet Heyer, Nydia Scalley Trifilio.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.