
Abstract
We studied the prevalence of HIV, syphilis, hepatitis B virus (HBV), and hepatitis C virus (HCV) infection and associated risk behaviors in the prison state system of Guanajuato, Mexico between September 2011 and February 2012. Blood samples were drawn from adult inmates in all State prisons who agreed to participate in this cross-sectional study. Data on risk behaviors were collected by using self-administered questionnaires. The prevalence of HIV, syphilis, HBV, and HCV infection was 0.6% [95% confidence interval (CI) = 0.2–1.1], 0.7% (95% CI = 0.4–1.0), 0.4 (95% CI = 0.04–0.74), and 4.8 (95% CI = 3.6–5.9), respectively. Female inmates had a higher prevalence of HIV (1.5% vs. 0.6%, p = .05), whereas male inmates had a higher prevalence of HCV (1% vs. 5%, p = .008). Twenty percent (n = 443, 95% CI = 15–26) of the participants were tattooed during incarceration, and most of them were tattooed with recycled materials. Around 60% (57%, 95% CI = 49–65) used drugs before incarceration, and 9.2% (n = 205) used injected drugs. During incarceration, 30% (95% CI = 23–39) used drugs and 43 continued injecting (20% of users). Consistent condom use was low among men before incarcerations but decreased by half during incarceration. The highest consistent condom use before incarceration was among men who have sex with men (MSM) (17.7%, 95% CI = 14–22), but it decreased (9%, 95% CI = 3–14) during incarceration. The prevalence of HIV, HBV, HCV, and syphilis in these inmates is higher than that of the local adult population. Most inmates had sex in prison, but few used condoms consistently. Access to condoms is apparently harder for MSM. Interventions to increase condom use, reduce use of shared or recycled materials for tattooing and injecting drugs, and treatment for drug abuse are needed.
Introduction
P
The United Nations has recommended the integration of preventive and care services for HIV/AIDS and STI for incarcerated people to national strategies for the control of these diseases. 6 Furthermore, the response program against HIV, AIDS, and STIs in Mexico acknowledges the vulnerability of prison inmates and has targeted them as a priority group for preventive efforts. 7 In reality, however, in most of the country, the main barrier for the implementation of government lead initiatives is the scarcity of knowledge and reliable information about HIV, other STIs, and blood-borne infections, and its associated risk behaviors in prisons.
Therefore, we conducted an initial assessment of the epidemiology of these infections, by estimating the prevalence of HIV, syphilis, hepatitis B virus (HBV), and hepatitis C virus (HCV), and we explored individual behaviors that may have led to the transmission of these infections within the prison state system of the State of Guanajuato.
Methods
Study setting
This study was implemented in the 10 detention centers (Centers for Social Re-insertion or CERESOs) managed by the General Directorate for Penal Execution and Social Re-insertion (DGEPRS)—a branch of the State Ministry of Public Safety of the State of Guanajuato 8 between September 2011 and February 2012. Guanajuato is located in central Mexico, and it has one of the lowest prevalence of HIV (0.01%) and STIs in the adult general population. 3,9 The incarceration rate is lower than the national average (77 vs. 204 per 100,000 inhabitant). There are currently no HIV Voluntary Counseling and Testing (VCT) services offered routinely within the prisons, and preventive services are limited. All centers have conjugal visits programs. Condoms are provided on request by the medical staff in each prison. Medical staff are hired by the DGEPRS and are paid by the prison system. The life-time prevalence of illicit drug use in Mexico is 5.2%, and that of injecting-drugs use is <0.01%. 10
Study design and study population
We conducted a cross-sectional, observational study. All inmates older than 18 years who were incarcerated in the 10 detention centers were invited to participate. We excluded inmates who could not give their informed consent due to physical, neurologic, or psychiatric conditions that limited the comprehension of potential risks and benefits of participation.
Sampling methodology and data collection
A team of Ministry of Health (MOH) staff visited the 10 centers, where inmates were offered group counseling 11 and voluntary testing for HIV, HBV, HCV, and syphilis. Around 100 inmates (±10) were accrued per day. A member of the study staff invited the group to participate in the research study, explaining the study aims, procedures, and risks of participating and highlighted that their participation in the study was voluntary. After the group meeting, all inmates were offered individual and private VCT services by the MOH staff. They were asked whether they wanted to be tested by using written informed consent, as mandated by a law in Mexico. Separately, participants were asked to consent to the use of their test results and to answer a risk behavior questionnaire. A written informed consent procedure approved by all participating institutions was used for this purpose. Those who refused testing were still invited to answer the questionnaire. Blood samples were drawn, and data on risk behavior were collected with an audio-assisted self-applied structured questionnaire (A-CASI).
Serological assays for HIV, HVB, and HCV were performed by using a fourth-generation chemoluminiscence assay (ARCHITECT i2000 system; Abbott Diagnostics, Wiesbaden-Delkenheim, Germany) to detect plasma-specific antibodies against HIV-1/2 antigens and HIV p24 antigen, HCV (AcHCV), and HBV surface antigen (AgsHB). Syphilis was screened by using a non-treponemal, activated coal, flocculation slide test (VDRL; Licon Laboratorios, S.A. Tlalnepantla, México). Patients whose results were positive for HIV or HCV antibodies were subsequently submitted to RT-PCR by COBAS Amplicor™ HIV-1 Monitor Test, version 1.5 (Roche Diagnostics, Basel, Switzerland) or Cobas AmpliPrep/Cobas TaqMan HCV quantitative test, version 2.0 (CAP/CTM HCV test, v2.0). All tests were performed at the Guanajuato State Center for Blood Transfusion.
The survey included questions on demographic information, information of the current and previous incarcerations, and individual risk behaviors both before and during incarceration (sexual behavior, tattooing, and drug use). The survey was designed by experts' consensus using questions from different sources 12,13 and adapting them to the local context. Before the implementation phase of the study, 10 inmates in two different centers answered the survey; we then reviewed each question with them, assessed comprehension of each question, use of appropriate language, difficulty of use of the automated program, adequacy of the multiple-option responses, and modified accordingly before the study.
Statistical considerations and data analysis
We estimated the precision of different estimates for different sample sizes, considering that we planned to offer tests to all inmates and asked them to participate in the study, but an uncertain proportion would refuse (See Supplementary Data; Supplementary Data are available online at
Ethical considerations
The study protocol, informed consent, and questionnaire were approved by the Johns Hopkins School of Public Health Institutional Review Board, the Bioethics Committees for Research in Human Subjects of the State Ministry of Health, and the University of the State of Guanajuato. We abided by the principles of the Declaration of Helsinki.
Results
Accrual, participation, and missing data
During the study period, there were 4,268 inmates in the 10 centers. Male inmates were less likely to be accrued than women (84% vs. 99%). The main reason for non-participation was conflict with inmates' paid labor activities. Participation also varied by center, ranging from 62% to >99%. We obtained data on the gender and age of all inmates present during accrual activities. A small proportion (n = 647) of non-participants agreed to answer questions about demographics only, and 43 of them agreed to answer questions on incarceration also. Study participants and non-participants were not different in terms of age, education and former employment, number of previous incarcerations, and length of current incarceration. Non-participants were more likely to be single (93% vs. 32%, p < .001).
Inmates could either withdraw the survey at any moment or opt not to answer specific questions, so missing data are heterogeneous for each question and tend to increase as the number of questions increases. For instance, we had missing data of age in 29 (1.1%) participants, of drug use before incarceration in 525 (20%) participants, and of tattoos during imprisonment in 632 (23%) participants (Supplementary Table S2). We present the results of 3,192 inmates (75%) who consented to provide blood tests results and of 2,690 (63%) who consented to answer the questionnaire. There were 2,227 (52%) questionnaires with complete data (Fig. 1). We present all the results of the unweighted analysis without imputing missing data in Supplementary Tables S2 and S3.
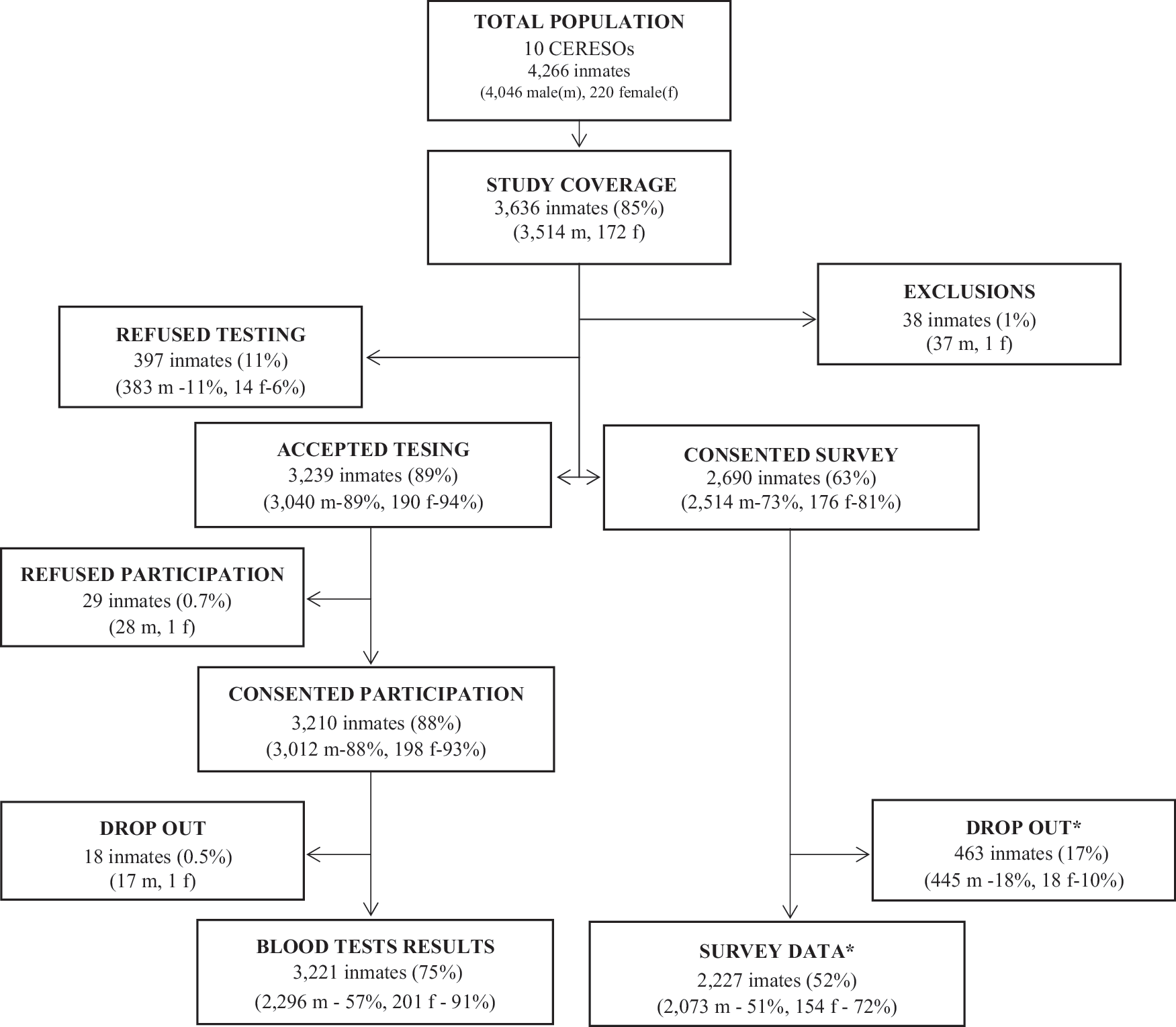
Accrual and participation of study population. *Drop-out from the study before finishing the questionnaire. There are incomplete survey data available on these subjects that were used for the analysis. There are complete survey data on 2,227 participants.
Characteristics of study population
Demographic characteristics are presented in Table 1 and Supplementary Table S3. The proportion of women in the sample was similar to that in the total prison population. Age distribution was similar across gender. Although the proportion of married participants was similar across both sexes, men were more frequently single (never married) as opposed to women, who were more frequently divorced or widowed. Overall, a higher proportion of women were below the median years of education than the general population in Mexico (9 years).
Weighted proportions according to the inverse probability of refusal participation by gender and center.
Missing data were imputed by using multiple-chain equation multivariate models for multiple imputations.
Fisher's exact test, except when indicated.
Housewife option was not available for men.
National median = 9 years.
CI, confidence interval; NA, not applicable.
Prevalence of HIV, syphilis, HBV, and HCV infection
The overall weighted prevalence of HIV, syphilis, HBV, and HCV infection was 0.6% (95% CI = 0.2–1.1), 0.7% (95% CI = 0.4–1.0), 0.4 (95% CI = 0.04–0.74), and 4.8 (95% CI = 3.6–5.9), respectively. The prevalence of HIV infection was higher among female inmates (1.5% vs. 0.6%, p = .05). Male inmates had a higher prevalence of HCV infection (1% vs. 5%, p = .008). Women had a higher prevalence of syphilis (1.6%, 95% CI = 0–4.3) than men (0.6%, 95% CI = 0.4–0.9) (Table 2) and Supplementary Table S4.
Weighted proportions according to the inverse probability of refusal participation by gender and CERESO.
95% CI estimated by using the Taylor linearization method with stratification by gender and cluster effect by center.
The overall estimated prevalence in Mexico is 0.23% (95% CI = 0.14–0.45) for adults aged 19–45. The estimated prevalence for adult men (19–45 years old) is 0.48% (95% CI = 0.26–0.92) and for adult women, it is 0.05% (95% CI = 0.02–0.13). 7 Previous HIV prevalence estimates among blood donors in the state vary between 0.08 and 0.39. The overall HIV prevalence among blood donors in a single blood bank in Irapuato Gto was 0.24% (0.28% among male donors and 0.11% among female donors). 52,53
No available estimates at the national or state level.
Overall prevalence of HBV among blood donors in a single blood bank in Irapuato Gto was 1.12% (1.04% among men and 1.42% among women). 53
Overall prevalence of HCV among blood donors in a single blood bank in Irapuato Gto was 1.14% (1.07% among men and 1.42% among women). 53
HBV, hepatitis B virus; HCV, hepatitis C virus.
Individual risk behaviors
Tattoo practices
A high proportion of inmates had been tattooed before current incarceration (n = 1,018, 47%, 95% CI = 44–50). Among these, 109 (11%, 95% CI = 9–13) were tattooed in previous incarcerations. Twenty-two percent (95% CI = 15–29, n = 443) were tattooed during current incarcerations. We summarized high-risk tattoo practices in Table 3 and Supplementary Table S5. Noticeably, tattoos were mostly applied by either fellow inmates who were “specialized” in tattooing (43%, 95% CI = 35–51) or cell mates (28%, 95% CI = 23–33). Handmade “tattooing machines” (52%, 95% CI = 46–58) were the most frequently used devices to get tattooed within the centers. About half of the participating inmates who got tattoos in these centers either did not know whether tattooing materials had been previously used or were tattooed with materials that were known to be used with other inmates.
Total number of inmates who reported having got a tattoo during current incarceration.
Numerators and denominators presented are raw data as answered by participants. The denominator represents the total number of inmates who answered each question.
Missing data were imputed by using multiple imputations by the chained equations procedure (mice) to estimate the proportions and 95% CI with 50 imputed datasets.
Weighted proportions according to the inverse probability of refusal participation by gender and center and 95% CI estimated by using the Taylor linearization method with stratification by gender and cluster effect by center.
Substance use
Most participants (63%, 95% CI = 57–69, n = 1,336) had used drugs before the current incarceration. Drug use during imprisonment decreased to 34% (95% CI = 24–44). The most commonly used drugs before imprisonment were marijuana and cocaine, each of which was used by 68% of inmates. During imprisonment, marijuana and cocaine continued to be the most frequently used drugs (Table 4 and Supplementary Table S6). Among drug users, 16% (95% CI = 13–18) responded having injected drugs at least once before incarceration (corresponding to 9.2% of all participants). Almost half (46%) of the IDU shared materials to inject or did not know whether needles or other materials had been previously used by other injectors (Table 4). Injecting-drugs use decreased during imprisonment (1.9% of participants and 6% of drug users), and less so was the frequency of high-risk injecting practices among those who continued injecting (Table 4).
Number of participants who answered the questionnaire.
The numerators and denominators presented are the raw data as answered by participants. The denominator indicates the total number of inmates who answered each question, excluding those who preferred not to answer that were managed as missing data.
Missing data were imputed by using multiple imputations by the chained equations procedure (mice) to estimate the proportions and 95% CI with 50 imputed datasets.
Weighted proportions according to the inverse probability of refusal participation by gender and CERESO and 95% CI estimated by using the Taylor linearization method with stratification by gender and cluster effect by center.
During the year preceding current imprisonment.
Sexual behavior
Sexual behaviors by gender are summarized in Table 5 and Supplementary Tables S7 and S8. Most male (94%) and female (97%) inmates had sex before current imprisonment. More than half of the men (58%) and women (56%) also had sex during imprisonment. Among the men who reported having sex before incarceration, 1,783 (93%, 95% CI = 91–95) agreed to having sex with women and 244 (12%, 5% CI = 3.4–16) agreed to having sex with men. The proportion of male and female inmates who agreed to having always used condoms during sexual intercourse before current imprisonment was low. Briefly, 10% of men and women agreed to having always used condoms for heterosexual intercourse before imprisonment. Among those who reported having had sex with men, 18% reported having always used condoms during sexual intercourse with other men. This proportion decreased by half during incarceration. In contrast, the proportion of men and women who reported having always used condoms during heterosexual sexual intercourse while incarcerated (9%) was similar to the frequency before imprisonment (Table 5).
Estimated by using the Taylor linearization method with strata by sex and cluster effect by CERESO.
Discussion
In this observational study to estimate the prevalence of HIV, syphilis, HVB, and HCV and individual risk behaviors that was conducted in the 10 Centers for Social Re-Insertion of the State of Guanajuato in Mexico during 2011 and 2012, we found the prevalence of HIV, syphilis, HBV, and HCV to be 0.6%, 0.7%, 0.4%, and 5%, respectively. In comparison, the estimated prevalence of HIV in the general population in the State is 0.2% among adults who are 18–65 years old (Guanajuato has one of the lowest HIV-prevalence in Mexico) 18 ; syphilis prevalence in the country is low (0.014%) 19,20 ; and the prevalence of both HBV and HCV infections has been consistently reported to be lower than 1% among blood donors. 19,21 The prevalence of these infections in the Guanajuato State Prisons are in the low range of prevalence previously reported for imprisoned populations in other developing countries. Our results, however, are in overall agreement with the consistently higher prevalence of STIs and blood-borne infections than that for the local, non-imprisoned, general, adult population reported worldwide. 1,14,15 Our findings are also similar to overall prevalence of 0.0%, 10%, and 0.6% of HBsAg, HCV, and HIV, respectively, in one prison in Durango City in 2002; and 0.2%, 3.2%, 2%, and 0.7% of HBsAg, HCV, syphilis, and HIV, respectively, at four Mexico City prisons in 2010. 4,5
We also observed that in these prisons, unprotected sex is the most frequent risk factor for HIV-infection and other STIs. The majority of male and female (58%) inmates reported having had sex during imprisonment, but only a minority consistently used condoms. High-risk sexual practices have been identified as an important behavioral risk factor associated to HIV among prisoners worldwide, 6 but previous data on inmates' sexual behavior and condom use in Mexican prisons or elsewhere are scarce and little detailed. 14,15 Interestingly, we found that the proportion of male inmates who consistently used condoms before incarceration (17% during sex with men and 9% during sex with women) decreased by half during incarceration. In contrast, in equally low proportions (9%), women reported having used condoms consistently during sex with men both before and during incarceration.
Considering that in these prisons inmates have access to condoms free of charge but condoms are provided on request by medical staff, we hypothesize that the characteristics of the social and policy environment appear to affect men and women differently. Restricted access to condoms for men may explain their decrease in use during imprisonment regardless of whether they are having sex with men or women. Although it is clear that physical environment and policies to make easy and expedite the availability of condoms are important factors for condom use among prisoners, 22 –24 less is known about social norms and beliefs as barriers for condom access and use. For instance, Calzavara found that the fear of being labeled as gay, the fear of being suspected of transporting drugs, and the perceived low risk of HIV transmission by same-sex activity were common barriers for inmates to request and use condoms in Canadian prisons. 25 Naturally, these barriers that are not necessarily related to condom-distribution policies but are more likely determined by social norms and values may vary from prison to prison. A more detailed explanation to this observation will require qualitative data gathering in future approaches to this population. The Joint United Nations Programme on HIV/AIDS (UNAIDS) recommends the provision of condoms and water-based lubricants for men and women in all closed settings.
In addition, a fair proportion of the inmates (20%) were tattooed while incarcerated, and more than half of them were tattooed in conditions of high susceptibility for high-risk practices. Tattooing is common among prison inmates around the world, including other prisons in northern Mexico, 4,14,26 and it is closely associated to injecting-drugs use. 26 –29 Tattooing has been both directly and indirectly associated to HCV and HIV among prisoners: Several studies have documented how inmates share and improvise needles and equipment given the scarcity of materials for this practice. 24,26,28 –30 Tattooing within prisons has also been identified as a risk factor for HCV infection among inmates and HIV seroconversion during incarceration. 27,31,32 Although legalization of tattoos in prisons and access to sterile materials for inmates to tattoo are contentious, 33,34 the potential threat to inmates who are getting tattooed within these State prisons requires the implementation of a program that at least reduces the sharing and reuse of equipment for tattoos and other forms of skin penetration, as recommended by UNAIDS/UNODC. 6
Finally, we found that drug use and injecting-drugs use among inmates before (63% and 9%, respectively) and during imprisonment (34% and 2%) are alarmingly high, and they should be considered and addressed as public health emergencies by themselves, considering that in Mexico only 5.5% of people between 12 and 65 years have used illicit drugs during their lifetime and less than 0.1% have ever injected drugs. 10 The relevance of this finding and its implications for the implementation of HIV and preventive programs for blood-borne infections should not be understated, as injecting drugs is a leading factor that is associated to HIV and HCV risk among inmates in developing and industrialized countries. 1,35 –40 Moreover, incarceration may increase the risk of HIV infection among drug injectors 27,32,35,41 even as much as three or four times among those who continue to inject during incarceration. 35,41 Drug use and injecting-drugs use have also been associated with an increased risk of high-risk sexual practices. 42,43
This study has several limitations that are worth considering. First, cross-sectional studies are well known to be susceptible to different biases, 44 and obtaining reliable data on sexual and drug use behavior remains challenging. 45,46 Second, considering the relatively low accrual rate, high proportion of refusal among approached inmates, and dissimilar characteristics between participants and non-participants, selection bias is particularly concerning for us. We consider that, notwithstanding its limitations, our study does not lack internal validity. First, our results are overall consistent with what has been previously found among prison inmates. Second, we implemented several strategies to limit the role of bias by narrowly defining and selecting a homogeneous population, defining a priori variables of interest, and using a self-applied structured questionnaire, and all study procedures were implemented systematically. 44,47 In addition, the use of self-applied computerized interviews appears to significantly reduce bias, 48 improve data quality, 49 and can be considered an accurate and reliable method to collect sensitive data. 50,51 We also used robust analysis methods to attempt to correct biases arising from lack of participation and missing data.
In conclusion, we observed that in this group of State Prisons in a region of Mexico with a low prevalence of HIV, syphilis, HBV, and HCV, inmates have a relatively high prevalence of STIs and blood-borne infections. Moreover, they frequently engage in high-risk behaviors such as sharing materials for tattoos and injecting drugs, and having unprotected heterosexual and homosexual intercourse. Although the prevalence of HIV and HCV is relatively low in comparison to prisons elsewhere, a carefully planned but prompt response should include interventions to increase condom use; reduce use of shared or recycled materials for tattooing and injecting; provide treatment and harm-reduction services to people in need of them; and offer routine, voluntary testing and treatment for HIV, HCV, and other STIs.
Footnotes
Acknowledgments
This work was supported by the Mexican Government through the National Council for Science and Technology (Consejo Nacional para la Ciencia y Tecnologia, CONACYT). The MOH of the State of Guanajuato provided logistic support and transportation. Pablo F. Belaunzaran-Zamudio received support for traveling and living expenses from the Universidad de Guanajuato and the Johns Hopkins Center for Global Health.
Authors' Contributions
P.F.B.Z. and J.L.M.G. conceived the study; P.F.B.Z., J.L.M.G., A.M.H., J.S.M., and C.B. designed the study protocol; P.F.B.Z., J.L.M.G., and S.R.R. carried out enrollment, blood samples and survey data collection, and blood tests results collection; P.F.B.Z. did the statistical analysis; P.F.B.Z. and J.L.M.G. drafted the article; and P.F.B.Z., J.L.M.G., A.M.H., J.S.M., S.R.R., and C.B. critically revised the article for intellectual content. All authors read and approved the final article. P.F.B.Z. is the guarantor of this article. The authors thank Jennifer Cuellar-Rodríguez for her critical review of the article.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.