
Abstract
Widespread use of combined antiretroviral therapy (cART) increased HIV patients' life expectancy, however, favored the development of kidney and cardiovascular diseases. The aim of this study was to investigate endothelial glycocalyx (eGC) damage and its association with renal function in HIV patients receiving cART. This is a cross-sectional study with HIV-infected patients with no renal and cardiovascular disease, recruited in public health centers in Brazil. Clinical and laboratory parameters of HIV patients were compared according to cART use and with a healthy control group. Blood ICAM-1 and syndecan-1 levels were quantified by ELISA kit. Estimated glomerular filtration rate (eGFR) was evaluated. A total of 69 HIV patients were included, with mean age of 33.4 ± 8.9 years, and 77.3% were male. Serum urea, creatinine, and eGFR were similar in all groups. No HIV patient had decreased GFR <60 ml/min. All HIV patients had higher systemic syndecan-1 compared with healthy controls (71.8 ± 25.4 ng/ml vs. 36.5 ± 14.3 ng/ml, p < .001). Syndecan-1 showed a significant positive correlation with serum creatinine (r = 0.437, p = .001), serum urea levels (r = 0.352, p = .006), and a negative correlation with eGFR (r = −0.315, p = .015) in HIV patients. Syndecan-1 remained independently associated with serum creatinine and reduced GFR even after we forced variables related with HIV infection status, tenofovir use, treatment time, dyslipidemia, and others in a multivariate analysis. HIV patients using cART with no clinical renal and cardiovascular disease presented eGC damage and it is associated with clinical markers of kidney dysfunction. Syndecan-1 may be a useful early biomarker to monitoring renal dysfunction in HIV patients in chronic use of cART. Further research is needed to evaluate this applicability.
Introduction
S
Kidney disease is a well-known and frequent complication of HIV infection. 2,3 Patients with HIV have substantially elevated risk to develop renal disease due to several factors related to cART and direct effect of HIV on the glomerulus and renal tubules. HIV-associated immune complex glomerulonephritis and CKD-related risk factors, including exposure to tenofovir, hypertension, and other comorbidities, also led to renal dysfunction. 1,4
Both HIV infection and kidney diseases are associated with endothelial dysfunction and accelerated cardiovascular events. 4 Patients in cART may have endothelial dysfunction with subsequent hypertension and atherosclerosis. 4,5 Also, HIV infection itself may produce direct endothelial damage, increasing endothelial permeability and the expression of adhesion molecules such as ICAM-1. 4,6
The endothelial glycocalyx (eGC) is an atheroprotective carbohydrate-rich structure that protects the endothelium and forms a vascular barrier against insults. eGC is composed mainly by core proteoglycans, especially the syndecan family. 7 Syndecan-1 is a marker of glycocalyx damage and its shedding has been associated with CKD, lower estimated glomerular filtration rate (eGFR), and predicts the risk of developing acute kidney injury (AKI) in other diseases. 8 –11
In the present study, we aimed to investigate endothelial and glycocalyx damage in HIV patients with apparently no renal and cardiovascular disease, receiving cART and its association with renal function. To our knowledge, this is the first study to evaluate eGC damage, through syndecan-1 quantification, in HIV patients.
Materials and Methods
Study participants
This is a cross-sectional study with HIV-infected patients recruited in public health centers in Fortaleza city, northeast of Brazil. The study protocol was reviewed and approved by the ethics committee. All the included patients provided written informed consent.
Exclusion criteria were as follows: age less than 18 or greater than 65 years, use of nephrotoxic drugs, nephrolithiasis, urinary tract infection, history of renal disease (according to Kidney Disease Outcomes Quality Initiative recommendations—glomerular filtration rate lower than 60 ml/min/1.73 m2), 12 arterial hypertension, heart failure and cardiovascular events, diabetes mellitus, systemic lupus erythematosus, and other autoimmune diseases. Also, HIV patients with coinfections were excluded.
Three groups of HIV patients were included: (a) those who never received cART, (b) HIV patients receiving cART containing tenofovir/lamivudine/efavirenz, or (c) HIV patients receiving cART containing zidovudine/lamivudine/efavirenz. The cART regimens did not change during the treatment time. Also, a group of 13 healthy subjects were included as a control group.
All enrolled personnel were submitted to full clinical assessment, including history taking and thorough clinical examination, including blood pressure measurements, waist circumference, and assessment of body mass index (BMI).
Sample processing
Random blood and urine samples were collected. Urine was centrifuged at 1,000 g for 15 min at 4°C to remove urinary sediment, including whole cells and other debris. Urine supernatant was aliquoted and immediately stored at −80°C. Venous blood was collected in BD Vacutainer® SST with silica clot activator and a polymer gel for efficient serum separation. After 15 min, the blood samples were centrifuged and the serum was aliquoted in specific aliquots to biochemical measurements and to quantify ICAM-1 and syndecan-1 levels. Finally, serum samples were stored at −80°C until analysis.
Clinical and biochemical measurements
Standard biochemical analyses were performed using a routine automated analyzer (Cobas C111; Roche®). In serum were quantified the creatinine, urea, albumin, glucose, phosphorous, triglycerides, and total cholesterol. In the urine, creatinine, glucose, and phosphorous were measured. Serum and urinary sodium and potassium were determined by ion selective electrolyte analyzer (9180, Electrolyte Analyzer; Roche) and the results expressed as mEq/liter. To assess tubular function, fractional excretion of sodium and phosphorous was calculated through standard formula. eGFR was estimated using the CKD-EPI equation. 13
Urinary albumin concentration was measured by automated immunoturbidimetric assay (Cobas C111; Roche). Urine protein excretion was quantified by the colorimetric pyrogallol red method (Labtest®). Urinary albumin and urinary protein/creatinine ratio (uPCR) were expressed as ratios to urinary creatinine concentration (mg/g-Cr) to correct the influence of urine concentration in random samples.
Quantification of ICAM-1 and syndecan-1
Endothelial biomarkers were measured in specific serum sample aliquots by ELISA kits. Syndecan-1 as a biomarker of eGC injury (Abcam, Cambridge, MA) and ICAM-1 as an endothelial adhesion molecule (Abcam, Cambridge, MA) were measured in duplicate.
These assays were sandwich ELISA based on the following: (1) uniform coating in 96-well plates of capture antibodies anti-syndecan-1 or anti-ICAM-1 specific to human syndecan-1 and ICAM-1 molecule, respectively; (2) binding of human syndecan-1 and ICAM-1 after adding patient serum samples; (3) binding of detection biotinylated antibodies with epitopes of syndecan-1 and ICAM-1 that were fixed by capture antibodies; (4) conjugation of streptavidin–horseradish peroxidase to the previously immobilized biotinylated antibodies; (5) and quantification of immobilized antibody biotin–streptavidin enzyme conjugates by monitoring horseradish peroxidase activities in the presence of the substrate 3,3′,5,5′-tetramethylbenzidine. Finally, the enzyme activity was measured by spectrophotometry at 450 nm, where the increase in absorbance is directly proportional to the concentration of syndecan-1 and ICAM-1 in the sample.
Statistical analyses
Statistical analyses were performed using SPSS 20.0 for Windows. Descriptive statistics are expressed as mean ± standard deviation or medians with the interquartile range for continuous variables and as frequency counts (percentages) for categorical data. To verify the normality of distribution of the observed data, all variables were tested using the Kolmogorov–Smirnov test. Levene's test was used to compare variability between the groups. Continuous variables were compared by Student's t-test and one-way analysis of variance with Tukey's post hoc as appropriate. In the case of non-normal data, the Kruskal–Wallis test was applied. Categorical variables were compared using the chi-square test. Pearson's correlation coefficients (r) were used to determine adjusted correlations between the analyzed variables. Multiple regression analysis was used to determine the independent association between the syndecan-1 with reduced GFR rate and serum creatinine as dependent variables. All tests were two sided, and p < .05 was considered statistically significant.
Results
Patient characteristics
After exclusion criteria, a total of 69 HIV patients were included in this study. The mean age was 33.4 ± 8.9 years and 51 patients were male (74%). There was no significant difference between age, gender, waist circumference, BMI, and blood pressure in the groups. Among HIV patients, 18 (26%) had never received cART, 30 (43.4%) received tenofovir, and 21 (30.4%) received zidovudine on cART. Patients' characteristics, according to cART use in comparison with controls, are show in Table 1.
Data are presented as mean ± standard deviation or as an absolute number with percentage in parenthesis.
One-way ANOVA.
Chi-square test.
Student's t-test.
Compared with control group. Significant p < .05.
BMI, body mass index; cART, combined antiretroviral therapy.
HIV patients receiving zidovudine in cART presented a significantly longer treatment time (23 ± 7.8 months vs. 14 ± 7.5 months, p < .0001) than patients using tenofovir. The majority of patients (63.6%) had undetectable viral load (<67 copies/mm3). Only three patients (4%) had higher levels of total cholesterol (>240 mg/dl) and 10 patients (14.5%) had triglycerides greater than 200 mg/dl.
Evaluation of renal dysfunction
Serum urea, creatinine, and eGFR were similar in all groups, including when comparing HIV patients with the healthy control group. No HIV patient had glomerular filtration rate less than 60 ml/min/1.73 m2. However, the urinary protein/creatinine ratio (uPCR) was higher in all HIV patients when compared to controls (72.3 ± 44 mg/g-Cr vs. 51.7 ± 22 mg/g-Cr, p = .018).
Sodium excretion fraction was significantly higher among HIV patients, mainly among those receiving cART with zidovudine, signaling for proximal tubular dysfunction (Table 2). However, there was no significant association between treatment time and sodium excretion fraction in the cART/zidovudine group (r = 0.133, p = .587).
Data are presented as mean ± standard deviation or as median (interquartile range).
One-way ANOVA.
Compared with control group. Significant p < .05.
Kruskal–Wallis test.
eGFR, estimated glomerular filtration rate; EFphosphate, EFNa, phosphate and sodium excretion fraction; sCreatinine, serum creatinine; sUrea, serum urea; eGFR, using CKD-EPI equation; sPhosphate, sNa, sK, serum phosphate, sodium, and potassium; uGlucose, urinary glucose; uPCR and uACR, urinary albumin and urine protein concentration per urinary creatinine concentration.
eGC injury in HIV patients
To investigate endothelial dysfunction, we have studied ICAM-1, as adhesion molecule, and syndecan-1, as a marker of eGC damage. Regarding ICAM-1, no difference between the groups was observed (p = .757). However, all HIV patients had higher systemic syndecan-1 compared with healthy controls (71.8 ± 25.4 ng/ml vs. 36.5 ± 14.3 ng/ml, p < .001). When we analyzed the different groups of HIV patients, by the one-way analysis of variance, we observed that higher levels of syndecan-1 remained statistically significant only in the group receiving cART/tenofovir (80.1 ± 39.8 ng/ml vs. 35.4 ± 14.3 ng/ml, p = .0001) and cART/zidovudine (76.7 ± 24.8 ng/ml vs. 35.4 ± 14.3 ng/ml, p = .001) showing that there is important endothelial dysfunction mainly in patients under specific treatment for HIV infection (Fig. 1). No significant correlation between syndecan-1 and ICAM-1 (r = 0.177, p = .154) was observed.

Endothelial glycocalyx damage by cART use in comparison with healthy control group. Values shown are mean ± standard errors. *p < .01 compared with healthy control group. cART, combined antiretroviral therapy.
eGC injury associated with renal dysfunction in HIV patients
The correlation analysis of ICAM-1 with other renal parameters in HIV patients revealed that systemic concentrations of ICAM-1 were not significantly correlated with any renal function parameter evaluated. However, syndecan-1 showed a significant positive correlation with serum creatinine (r = 0.437, p = .001), serum urea levels (r = 0.352, p = .006) and a negative correlation with eGFR (r = −0.287, p = .028) showing an important association between eGC damage and traditional renal function biomarkers in HIV patients (Fig. 2). The correlations between renal function tests and endothelial biomarkers are show in Table 3.
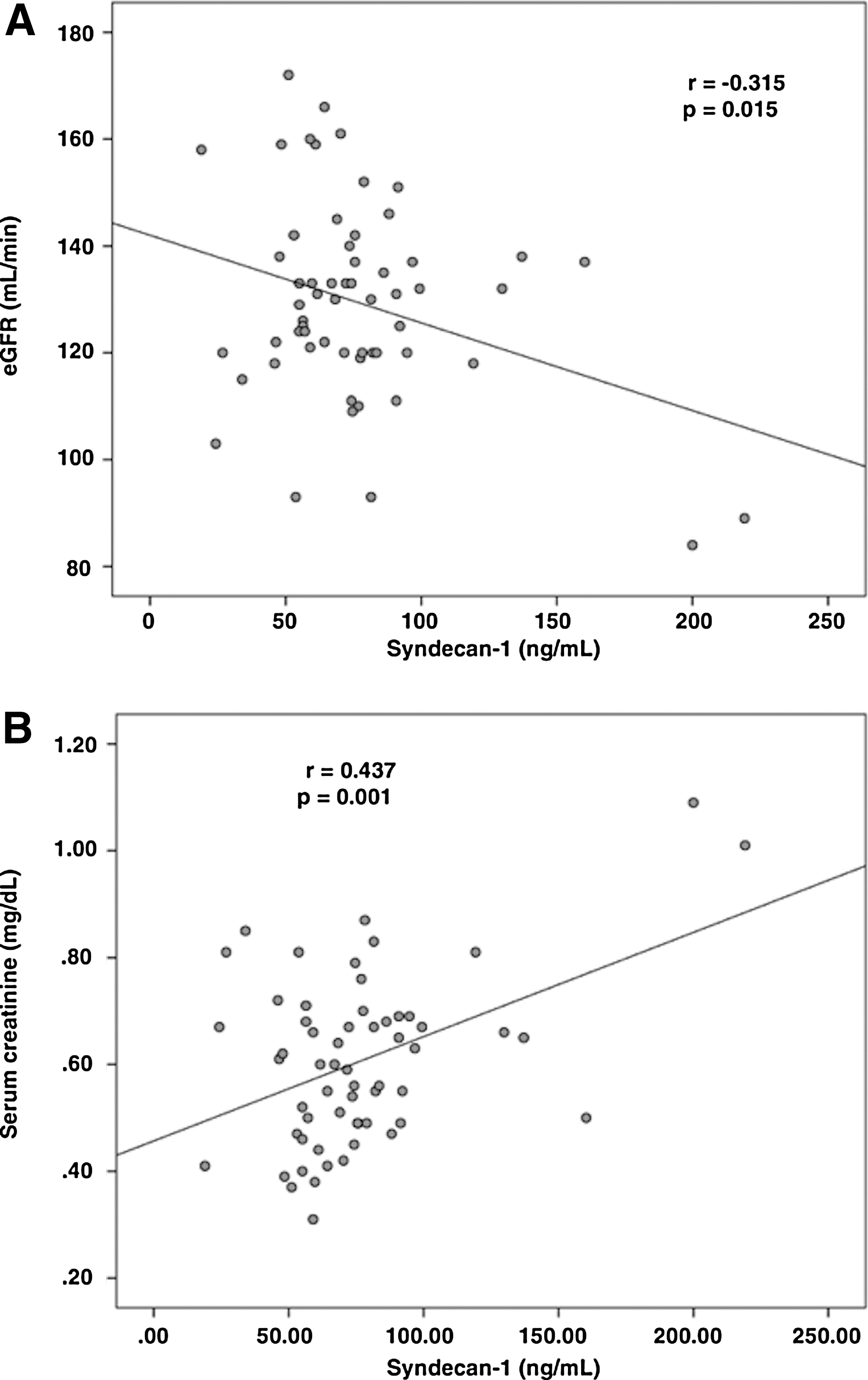
Scatter plots showing the correlation of reduced estimated glomerular filtration rate
r, Pearson's correlation coefficient; * p < .05 considered significant.
To further explore the association between syndecan-1 and renal dysfunction, models of multiple regression analysis were performed (Table 4). In these models, we forced variables related with HIV infection status (CD4 count, viral load), treatment time, dyslipidemia (triglycerides and total cholesterol), and also glucose and albumin. Even after forcing all variables into the model, syndecan-1 remained independently associated with serum creatinine and reduced GFR.
Multiple regression analysis results.
sCr, serum creatinine.
Discussion
To our knowledge, this is the first study to show a significant association between renal biomarkers and eGC damage markers among asymptomatic HIV patients receiving cART. In this study, we have evaluated endothelial and glycocalyx damage and its association with renal function in HIV-infected patients. For the first time, syndecan-1 was found to be higher in HIV patients, evidencing systemic glycocalyx injury.
Kidney disease is a frequent complication of HIV infection, with an estimated prevalence varying from 6% to 48% among infected patients. 14 –16 Before the widespread use of cART, HIV-associated nephropathy or “HIVAN,” manifested by collapsing glomerulopathy, was the main form of HIV-associated CKD. 17 Prolonged use of cART increased life expectancy of HIV patients and new patterns of CKD have emerged. 18 Exposure to cART itself may lead to tubular toxicity, electrolyte abnormalities, and subclinical renal impairment in patients with normal traditional renal function tests. 19,20
In the present study, relevant abnormalities in renal parameters were not observed, and the studied HIV patients had no clinical evidence of renal disease. Several observational studies have assessed proximal tubular dysfunction in HIV patients, using serum phosphorous, potassium, and sodium, fractional excretion of phosphorus and sodium, and glycosuria with normal serum glucose. 21 Interestingly, we observed a higher EFNa in HIV patients using zidovudine on cART, which can be a signal of proximal tubular defect. This could be explained by the fact that the HIV group using zidovudine had a significantly longer treatment time than patients in the tenofovir group. Hence, a higher EFNa appears to be associated with chronic use of cART. Moreover, other studies suggest that higher urinary sodium excretion is associated with increased risk to CKD progression. 22
CKD in HIV patients can progress to end stages even when cART maintains viral suppression. 23 Kidney function decrease has been associated with increased cardiovascular risk related to endothelial dysfunction, hypertension, diabetes, and atherosclerosis. 24 Hypertension and cardiovascular diseases are important risk factors for end-stage renal disease in HIV patients. 25 In this study, HIV patients had similar levels of blood pressure, glucose, triglycerides, total cholesterol, and waist circumference. Interestingly, ICAM-1 levels were not significantly different in HIV patients compared with healthy controls, even among the cART-treated group and never-treated patients. The inflammation induced by HIV infection may increase endothelial activation and secretion of ICAM-1 in the blood, which is associated with cardiovascular disease. However, during cART use, this mechanism is inhibited by suppressing both viral load and HIV-induced inflammation. 26 Fourie et al. evidenced in 144 HIV patients that the odds ratio for endothelial activation represented by intercellular adhesion molecule 1 (ICAM-1) and vascular cell adhesion molecule 1 (VCAM) were substantially higher in never-treated (no-ART) than in treated (ART) individuals. 26 Thus, we suggest that chronic cART use in our group contributed to decreased ICAM-1 levels, despite the tendency to be significant between groups.
On the contrary, we observed that ICAM-1 levels were not associated with renal dysfunction in multivariate analysis. Other studies also presented no association between ICAM-1 levels and chronic renal diseases, suggesting that this molecule may not be a confident biomarker to evaluate renal dysfunction. 27 In this study, the ICAM-1 levels were not significantly different between the groups and appear to have no important role in endothelial and renal pathology of HIV patients. We cannot exclude the important limitation of our sample size and cross-sectional design. Given the role of ICAM-1 in inflammation and endothelial dysfunction on pathogenesis of HIV, further prospectively studies are necessary to investigate the role of ICAM-1 in renal dysfunction during cART treatment.
Importantly, we observed significantly higher levels of serum syndecan-1 in HIV patients, mostly in cART groups, which reflect eGC damage. Endothelial dysfunction is an important mechanism involved in the increased cardiovascular risk seen in the HIV population. 4 Recent studies evidence that HIV infection itself may cause endothelial damage and that it is associated with increased circulating levels of potential serum markers of endothelial dysfunction. 28,29 eGC covers the endothelium and appears to present early changes when there is endothelial dysfunction. Syndecan-1 is a recognized marker of glycocalyx degradation. 30,31 The eGC perturbation leads to shedding of syndecan-1 into the blood stream. 7 Moreover, increased levels of circulating syndecan-1 in the blood are associated with reduced thickness of the eGC. 30,31 This contributes for glycocalyx degradation and damage. As a result, higher levels of syndecan-1 in the blood may be associated with early endothelial dysfunction and increased vascular permeability, favoring inflammation and atherosclerosis. 32 In this study, the levels of systemic syndecan-1 were more elevated in cART groups with tendency to significance between no-treated groups. Other studies suggest the important role of efavirenz-containing regimens in endothelial activation and injury. 33,34 In fact, all HIV patients using cART in our study had efavirenz-containing regimens. Hence, we suggest that efavirenz may play an important role in glycocalyx degradation and damage evidenced by systemic syndecan-1.
The identification of endothelial dysfunction has a huge importance for any group of patients. It allows the implementation of measures to prevent or at least attenuate cardiovascular diseases, which represent an important cause of death in HIV-infected patients, especially among CKD patients. 4 According to this study, eGC damage might be a common factor between kidney dysfunction and cardiovascular risk. We observed in our HIV patients, who had no CKD, a significant positive correlation between syndecan-1 and traditional renal function biomarkers (serum urea, creatinine) and an inverse correlation between syndecan-1 and eGFR. These results showed an important association between shedding of the atheroprotective glycocalyx and biomarkers of CKD, pointing to an early endothelium damage and incipient kidney dysfunction. Nevertheless, syndecan-1 levels were not associated with urinary protein/creatinine ratio (uPCR) and urinary albumin/creatinine ratio (uACR), important CKD biomarkers. 35 Our HIV patients were selected to have no renal disease or risk factors to kidney disease development. Furthermore, the levels of PCR and ACR were low in our HIV patients and had no differences between healthy individuals. Thus, we suppose that possible intrinsic renal injury in these HIV patients was undetectable by PCR or ACR and not sufficient to find a correlation with systemic syndecan-1 levels.
We forced in a multivariate model, variables related with chronic exposure to cART, atherosclerosis, and other laboratory findings. Interestingly, even after controlling these variables in the model, only syndecan-1 remained associated with serum creatinine and reduced glomerular filtration rate in HIV patients. A possible mechanism for eGC damage and shedding of syndecan-1 in CKD may be associated with the presence of uremic toxins such as urea, loss of ability to excrete salt and water, inflammatory factors, and hypertension. 9,36 Chronic inflammation, hypertension, atherosclerosis, and CKD are important contributing factors for cardiovascular morbidity and mortality in HIV patients. 2,4 Furthermore, chronic exposure to some antiretroviral agents may also increase the rate of cardiovascular disease and kidney damage among HIV patients. 37 –40 This association has not been previously demonstrated for syndecan-1 in HIV patients. Diagnosis of early renal dysfunction in HIV patients is highly necessary and can affect patient survival. 17 Further prospective studies are necessary to understand the role of syndecan-1 in early CKD development, including novel CKD biomarkers such as FGF-23, ADMA, and MCP-1.
The present study has some limitations. The multiple testing may induce false-positive results as in correlation analyses. We had a small sample size because it is not easy to find HIV patients in our region with no comorbidity and with normal kidney function (at least taking into consideration the traditional biomarkers). Moreover, the cross-sectional design of the study makes it difficult to get evidence of a causal association between syndecan-1 shedding and kidney dysfunction. Furthermore, we did not evaluate other inflammatory mediators that could help explain some pathophysiological mechanisms of HIV-associated endothelium dysfunction and kidney disease. We acknowledge that our findings should be considered preliminary until validated in larger studies, with other antiretroviral agents in a long follow-up design.
In conclusion, HIV patients in chronic use of cART with apparently no renal and cardiovascular disease present eGC damage, evidenced by elevated levels of syndecan-1, and it is associated with clinical biomarkers of kidney dysfunction. For the first time it was demonstrated that syndecan-1 may be a useful early biomarker to monitor renal and endothelial dysfunction in HIV patients. Further larger studies are necessary to establish its application in clinical practice.
Footnotes
Acknowledgments
We are very grateful to the team of physicians, nurses, pharmacists, residents, and medical students from the healthcare facilities in Fortaleza, providing great assistance to the HIV patients in our region, and for the technical support provided for the development of this research. This study was supported by the Brazilian Research Council–Conselho Nacional de Desenvolvimento Científico e Tecnológico, CNPq (financial support number 442469/2014-4) and Edson Queiroz Foundation/University of Fortaleza (project number 2006/2016).
Author Disclosure Statement
No competing financial interests exist.