
Abstract
New South Wales has the greatest burden of HIV in Australia, with 2012 and 2013 recording the highest rates of new diagnoses in 20 years. Concurrently, there has been significant changes in antiretroviral treatments and testing paradigms. We compiled a statewide resistance database to characterize changes in HIV-1 resistance mutations over time. Genotypic antiretroviral resistance testing (GART) was performed on request at three reference laboratories using commercial and in-house methods. In total, 7629 HIV-1 polymerase sequences obtained from GART from 2004 to 2013 were retrospectively collated, reformatted, de-identified, and analyzed using Stanford HIVdb program 7.0 and the 2009 World Health Organization (WHO) surveillance drug resistance mutations (SDRMs). Analyses were performed on subgroups of known treatment naives, treatment experienced, and seroconverters. There has been a decrease in overall rates of prevalent drug resistance mutations from 57.8% in 2004 to 21% in 2013. Dual and triple class resistance mutations have decreased from 32.7% in 2004 to 5.8% in 2013 and 16.4% to 1.2%, respectively. In treatment-naive individuals (n = 450), the frequency of protease inhibitor (PI) mutations remains low at 2.7%. In seroconverters, rates of transmitted drug resistance (TDR) are 6.6%, 3%, 3%, and 1.5% for overall, PI, non-nucleoside reverse transcription inhibitor (NNRTI), and NRTI, respectively. In treatment experienced, rates remain stable with 36.0%, 18.9%, 29.1%, and 6.4% for overall, NNRTI, NRTI, and PI mutations. The most common mutations in treatment experienced occurred at position M184, T215 (NRTI); K103 (NNRTI); I54 (PI). Apparent decreases in prevalent SDRMs can be attributed to changes in GART testing indications over time. In treatment-naive and -experienced subgroups, rates have been stable with low rates of TDR in seroconverters.
Introduction
Australia is a high-income country with an estimated 27,150 (24,630–30,310) people living with HIV, 19,097 of whom are men who have sex with men (MSM). 1,2 In New South Wales (NSW), there are 349 new diagnoses on average over the past 6 years, with the exception of 2016 when there were 9% fewer diagnosed. 3 Eighty-two percent of those newly diagnosed reported MSM risk exposure. 3 An estimated 92% (8,291) of those in NSW receiving care through public services are on treatment. 3,4
Combination antiretroviral therapy has been universally available since 1997 through the publicly funded Federal Government pharmaceutical benefits scheme (PBS). Postexposure prophylaxis is freely available and recommended in national guidelines for high-risk exposures. 5 Although pre-exposure prophylaxis (PrEP) has not been approved for inclusion on the PBS, implementation trials commenced in 2016 in the most populous state, NSW. The state is in the midst of rolling out a multidimensional strategy to virtually eliminate HIV transmission in NSW by 2020. 6
Rates of transmitted drug resistance (TDR) in Australia are reported to be the highest worldwide [15.5% (12.8%–18.3%)] 7 ; however, populations sampled for these studies may not be representative as were from single centers, and included data collected during the pre-highly active antiretroviral therapy (HART) era. Rates as high as 23.2% were reported in an NSW-based study from 1992 to 2001, but this was from a single center in the pre-HART era and included only MSM. 8 Other states in Australia have reported TDR rates of 16% in Victoria 9 and 21.9% in South Australia. 10 In some states, there has been an increase in the number of non-B subtypes, mainly acquired heterosexually. 11,12 More recent clinical trial data from the Strategic Timing of AntiRetroviral Treatment study also suggests that Australia has the highest overall TDR rate in world (17.5%); however small sample size limits the interpretation. 13
Currently there is no national approach to surveillance of TDR in Australia. In the context of evolving treatment paradigms, and concurrent rollout of PrEP in NSW, the aim of this study was to describe prevalent HIV drug resistance mutations in NSW over the 10 years before implementation of current HIV strategies.
Materials and Methods
Indications for resistance testing
In NSW, genotypic antiretroviral resistance testing (GART) is currently performed at three reference laboratories (Lab 1, 2, 3). In the early years of this study, testing was restricted to treatment-experienced patients with virological failure; however, testing indications have since changed. Local and international guidelines recommended baseline GART since at least 2007. 14 In 2011, testing was made universally available and up to two tests per year are funded through the Medicare benefits schedule when performed at presentation, before antiretroviral therapy or at treatment failure, provided HIV load is >1,000 copies per mL plasma. 15
Ethical approvals
This low- to negligible-risk study was approved by the Human Research and Development Committee of St Vincent's Hospital with site-specific approvals obtained for Westmead Hospital (Pathology West) and Royal Prince Alfred Hospital. IRB approval: HREC: LNR/13/STV/387, STV RGO SSA: AU/7/D985117.
Data sources
HIV polymerase sequences were obtained from three reference laboratories. Additional data, including date of birth (DoB), sex, date of infection, seroconverter status, and ART treatment status, were extracted from the electronic health record of hospitalized patients at laboratories 1 and 2. This information was not available patients that were referred from other centers such as outpatient sexual health clinics.
Inclusion criteria
All GART performed from January 1, 2004 until December 31, 2013 was included for analysis. A single sequence containing protease and reverse transcriptase genes was included for a single patient per calendar year.
Exclusion criteria
Duplicate sequences per patient within calendar year were excluded. Duplicate individuals were flagged by identical DoB (2006–2013) and duplicate sequences were identified by phylogenetic distance (2004–2005) where DoB was not available. Poor-quality sequences containing stop codons or frameshift mutations were excluded. Integrase mutations were not included, as integrase region sequencing was not routinely performed during the study timeframe.
Definitions
Seroconverter status was recorded between 2004 and 2013 at a single site (Lab 1) using the following definitions: (1) laboratory confirmed HIV with documented negative serology within previous 6 months, (2) positive detuned BED IgG-Capture Enzyme Immunoassay (BED assay), and (3) ≤3 bands on western blot with positive p24 antigen or ≤3 bands on western blot with detectable proviral HIV-1 DNA or ≤3 bands on western blot with plasma HIV-1 RNA >10,000 c/mL.
Treatment status could only be determined from 2009 onward. Treatment-naive status was assigned when there was no known previous antiretroviral regimen and included all seroconverter as well as chronic infections. Treatment-experienced status was assigned when there was evidence of a current or previous antiretroviral regimen, regardless of the duration of infection.
Laboratory methods
Plasma samples were collected in whole blood ethylenediamine tetraacetic acid and transported to reference laboratories. Plasma is stored at −80°C and batched for population based genotypic resistance testing. For laboratories 1 and 2, Trugene® HIV-1 genotypic kit was used where as an in-house assay is used by laboratory 3. Sequences were assembled and proofread with GeneObjects (Lab 1) Seqscape® (Lab 2) and Sequencher® (Lab 3). Sequence file saved in FASTA format using laboratory generated accession number as file name. Individual FASTA files merged into multiFASTA file using DNA baser, and then converted to text format. All text file sequences were submitted to Stanford HIV Drug Resistance Database version 7.0 for quality analysis (stop codons and frameshift mutations). 16,17
Resistance mutations were defined according to World Health Organization (WHO) 2009 surveillance drug resistance mutation (SDRM) criteria. 18 Subtype was determined for reverse transcriptase gene according to the Stanford HIV Drug Resistance Database v7.0. 17
Statistical analysis
The main outcome was the frequency of resistance mutations for reverse transcriptase and protease genes defined according to WHO SDRM list. 18 Baseline characteristics, including age, sex, and subtype, were compared across sites. Frequency of SDRMs was determined overall and for non-nucleoside reverse transcription inhibitors (NNRTIs), NRTI, and protease inhibitor (PI) classes using population analysis with Calibrated Population Resistance tool version 6.0. 19 Stata 12.0 (StataCorp LP, TX) was used for statistical analysis.
Results
Out of a total of 7,639 GART performed in NSW from 2004 to 2013, 6,901 (90%) contained unique sequences within a calendar year. Seven hundred thirty-eight duplicates within calendar year were excluded. Treatment history was available for 799 (12%) sequences from 2009 to 2013 only as summarized in Table 1. A mean 690 GART were performed each year, with 550 in 2004 and a maximum of 788 in 2010 (Table 1). Table 2 summarizes characteristics of those who had demographics available; 5,028 (90%) were male with a median age of 41 years (IQR 33–48).
Number of Genotypic Antiretroviral Resistance Tests Performed
Data from Table 2, page 27 of Annual Surveillance Report 2016.
Baseline Characteristics
ART, antiretroviral resistance testing; SD, standard deviation.
Surveillance drug resistance mutations
There has been an overall decrease in frequency of prevalent SDRM from 57.8% in 2004 to 21% in 2013, with corresponding declines in PI (24%–4.6%), NRTI (52.3–11.8%), and NNRTI (37.5%–12.3%) resistance mutations over this time (Fig. 1). From 2009 to 2013, there was a significant decrease in overall frequency of SDRMs from 54.8% to 30% (p < .01) for treatment-experienced patients (Table 3). There were corresponding declines in PI, NRTI, and NNRTI classes in treatment-experienced group, whereas SDRM rates in treatment-naive individuals have been stable with overall rate of 13.6% (Table 4). In a subpopulation of seroconverters at a single laboratory (n = 136) the overall rate of SDRMs was 6.6% (9/136), 1.5% (2/136) in PI, 3% (4/135) in both NRTI and NNRTIs.
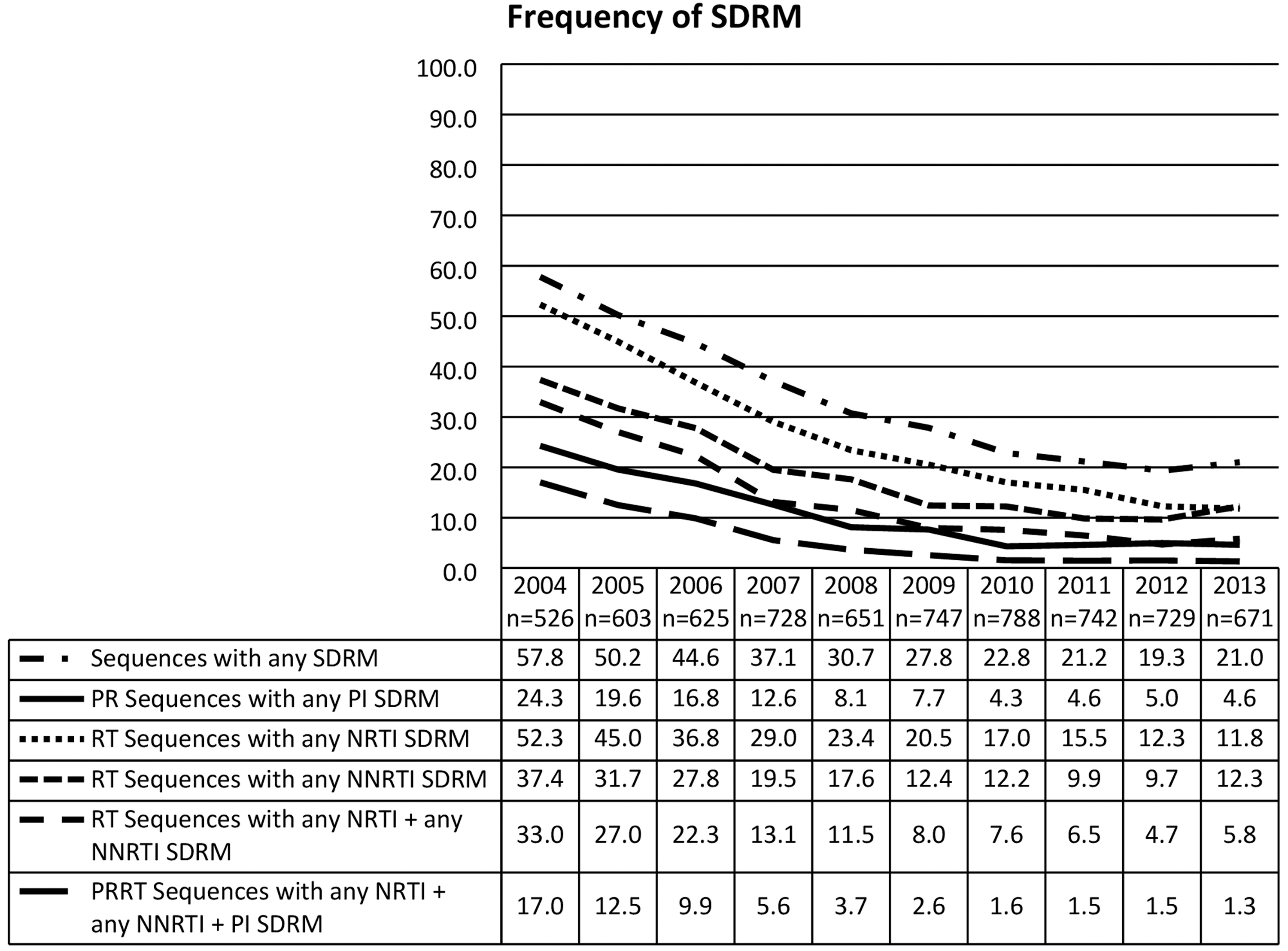
Frequency (%) of SDRMs in all sequences 2004–2013. NNRTI, non-nucleoside reverse transcriptase inhibitor; NRTI, nucleos(t)ide reverse transcriptase inhibitor; PI, protease inhibitor; RT, reverse transcriptase; SDRM, surveillance drug resistance mutation.
Frequency (%) of Surveillance Drug Resistance Mutations for Treatment Experienced
NNRTI, non-nucleoside reverse transcriptase inhibitor; NRTI, nucleos(t)ide reverse transcriptase inhibitor; PI, protease inhibitor; PR, protease; RT, reverse transcriptase; SDRM, surveillance drug resistance mutation.
Frequency (%) of Surveillance Drug Resistance Mutations for Treatment Naive
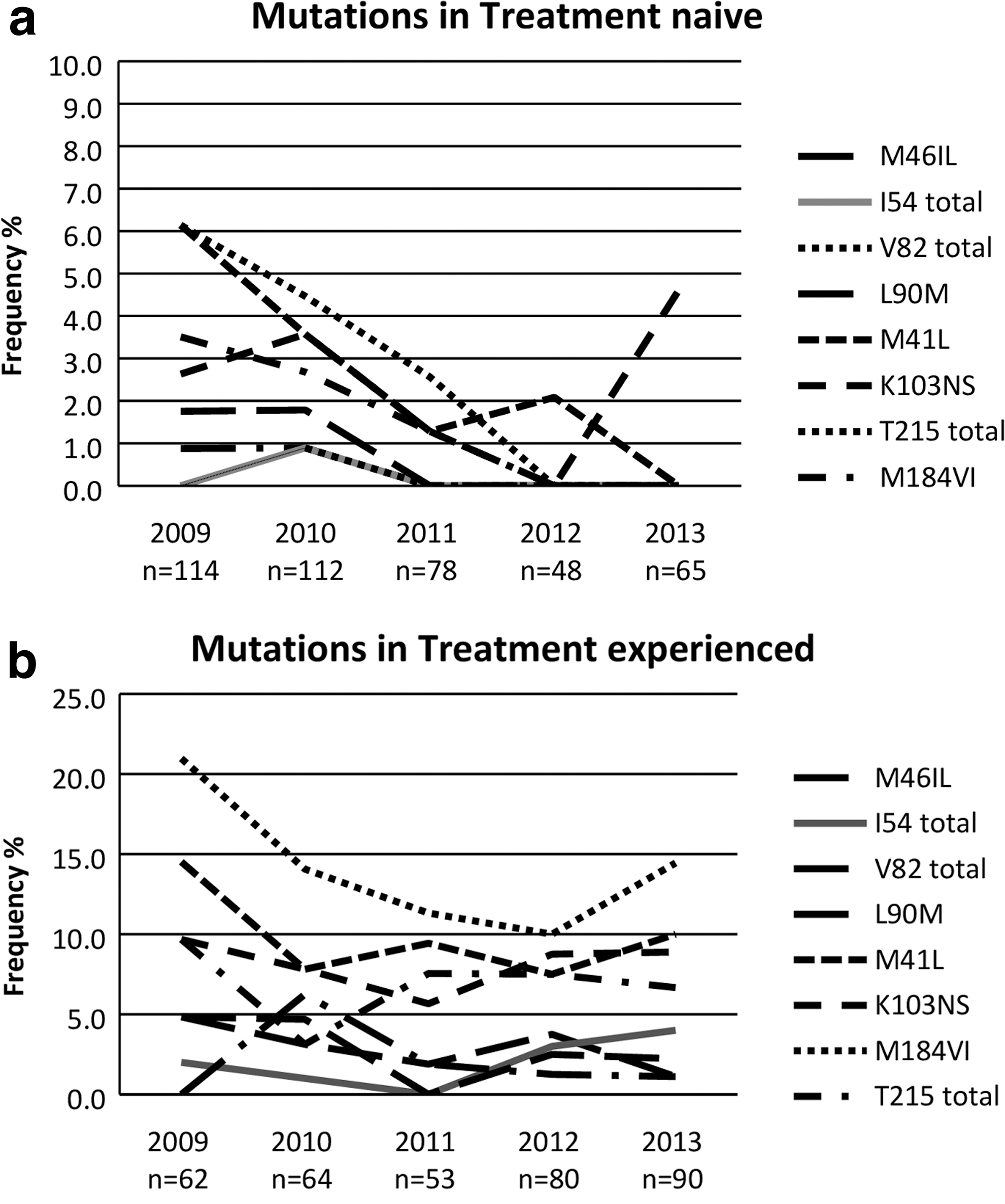
The most frequent mutation in the treatment-naive group was T215, which has shown a decline since 2009, whereas M184VI also showed a declining trend until 2012 in treatment-experienced group (Fig. 2a, b). T215 was seen most frequently in treatment-naive group (3.6% overall), whereas M184 was the most frequent mutation (14% overall) in treatment-experienced individuals. In the treatment-experienced population 85% (295/347) isolates retained susceptibility to tenofovir, with 1.1% (4/349) containing K65R mutation and 3.4% (12/349) with K70R mutation.
Discussion
This is the first analysis of all GART performed in NSW over a 10-year period. There has been a decline in frequency of SDRM in treatment-experienced populations, reflecting the availability of better-tolerated regimens and improved adherence. Rates in treatment-naive patients have been stable. Owing to the referral pathway for resistance testing, the true rate of TDR could not be determined for all sequences in this study, as testing indication (recently infected, newly diagnosed, and antiretroviral naive vs. treatment failure) is not routinely available to the reference laboratories. SDRM rates in a subpopulation of recently infected seroconverters are an alternate method for approximating the rate of TDR, and has the advantage of lower rates of reversion mutations. 20 The rates reported in our seroconverter population were lower than reported in previous publications from the previous decade. 8
Based on data from the Australian HIV observational database (AHOD), the proportion of patients currently receiving antiretroviral treatment in NSW has increased from 88.8% (539/607) in 2004 to 96% (923/961) in 2013. 21,22 Despite the increases in treatment uptake seen over the 10-year period, SDRMs in the treatment-experienced population has declined. Contemporaneous knowledge of the prevalent rate of drug resistant mutations at a statewide level is important to inform and update local antiretroviral guidelines. This is of particular relevance to NSW, which is participating in a large-scale PrEP implementation trial that has enrolled >4,000 high-risk individuals. 23 This study has a coverage of an estimated 83% (6,901/8,291) of those on treatment in NSW, providing a background rate of HIV-1 drug resistance prevalence before implementation of this strategy, allowing comparisons with future surveillance studies. Despite universal access to ART and availability of subsidized GART in Australia, there is currently no national antiretroviral resistance surveillance program.
During the study period, there has been a shift in the resistance testing paradigm, initially only available to those failing a combination antiretroviral regimen. Since July 1, 2011, laboratories received reimbursement for testing when performed at presentation, before ART and with treatment failure. 15 This change has altered the population being tested in NSW, and needs to be considered in interpretation of study results. The apparent decrease in prevalence of SDRMs can be attributed to an increased proportion in treatment-naive patients undergoing testing in the years leading up to 2011.
One limitation of this study is the ability of the reference laboratory to identify prior ART exposure. This was possible for some of the sequences; however, this review only included hospital-based records. Thus, treatment that was commenced at an earlier time in the community would not have been captured. This may have led to an overestimation in treatment-naive individuals, partly explaining the higher than expected prevalence of M184 and T215 mutations in this group. Given the absence of treatment status data at Lab 3, which also had the highest proportion of non-B subtypes, comparison of differences in mutations between subtypes was not performed as this would be limited by small numbers and selection bias.
This study differs from most resistance surveillance reports that focus solely on TDR. Owing to format and availability of sequence data collected, this study reflects the prevalent rates of mutations at a population level. The inclusion of acquired drug mutations also can provide insights into the longevity and tolerability of various regimens. For those known to be treatment experienced, there was a decrease in the rate of acquired drug resistance, reflecting newer better-tolerated antiretrovirals and a shift toward single tablet regimens (STRs). The most common regimen from 2008 to 2014 in the AHOD cohort was emtricitabine (FTC), tenofovir disoproxil fumarate (TDF), efavirenz (EFV), which has been available as an STR since January 1, 2010. 21 Importantly, the frequency of mutations specific to EFV (P225H) was low in both naive and experienced populations, although it is now recommended as an alternative regimen in Australian guidelines. Rates of TDF mutations are low in comparison with global rates, possibly reflecting the availability of other ART-based regimens such as ABC/3TC, which is also listed as a recommended regimen in national guidelines. 24,25
The rate of TDR found in seroconverter population in this study is not as high as reported in recent literature, and reflects the need for prospective SDRM surveillance to be linked to clinical and epidemiological notification databases. The rates of TDR in the seroconverter population is comparable with that reported in an antiretroviral-naive population in the United Kingdom, with similar frequencies of common mutations reported. 26 A large population study analyzing routine resistance testing in the United States has also reported decreasing trends in prevalence of resistance in all classes with the exception NNRTI class that increased. Our study also did report an increased rate of NNRTI class resistance in treatment-naive population in 2013, but follow-up data are needed to determine if this is an ongoing trend. 27
The increase in non-B subtypes in this state is consistent with what has been reported in other parts of Australia. 11 The most prevalent non-B subtype CRF01_AE is supported by an increasing proportion of diagnoses in people born in Southeast Asia, where this subtype is common. 1
In summary, the prevalence of overall SDRMs in NSW is decreasing. The increase in non-B subtype prevalence is consistent with other states in Australia. The rate of TDR has remained stable, whereas the rate of acquired drug resistance has decreased. The rates of TDR reported in seroconverters are lower than previously reported in Australia, reflecting the need for TDR surveillance linked in real time with epidemiological notifications data.
Footnotes
Authors' Contributions
A.P., D.D., R.G., T.K., and D.A.C. conceived and designed the experiments. A.P. performed the experiments. A.P. and K.P. analyzed the data. A.C., K.T., H.S., and A.S. contributed reagents/materials/analysis tools. A.P., K.P., and T.K. wrote the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
A.P. is recipient of NHMRC postgraduate research scholarship APP1074467.