
Abstract
Laboratory assays that identify recent HIV infections are important for assessing impacts of interventions aimed at reducing HIV incidence. Kinetics of HIV humoral responses can vary with inherent assay properties, and between HIV subtypes, populations, and physiological states. They are important in determining mean duration of recent infection (MDRI) for antibody-based assays for detecting recent HIV infections. We determined MDRIs for multi-subtype peptide representing subtypes B, E and D (BED)-capture enzyme immunoassay, limiting antigen (LAg), and Bio-Rad Avidity Incidence (BRAI) assays for 101 seroconverting postpartum women, recruited in Harare from 1997 to 2000 during the Zimbabwe Vitamin A for Mothers and Babies trial, comparing them against published MDRIs estimated from seroconverting cases in the general population. We also compared MDRIs for women who seroconverted either during the first 9 months, or at later stages, postpartum. At cutoffs (C) of 0.8 for BED, 1.5 for LAg, and 40% for BRAI, estimated MDRIs for postpartum mothers were 192, 104, and 144 days, 33%, 32%, and 52% lower than published estimates of 287, 152 and 298 days, respectively, for clade C samples from general populations. Point estimates of MDRI values were 7%–19% shorter for women who seroconverted in the first 9 months postpartum than for those seroconverting later. MDRI values for three HIV incidence biomarkers are longer in the general population than among postpartum women, particularly those who recently gave birth, consistent with heightened immunological activation soon after birth. Our results provide a caution that MDRI may vary significantly between subjects in different physiological states.
U
We hypothesized that the observed discrepancies reflect, in part, particular characteristics of the ZVITAMBO trial participants, all postpartum women. The discrepancy is consistent with evidence that postpartum women exhibit elevated immunological responses, such that antibody levels increase more rapidly than in women who are neither pregnant nor postpartum. 7 This hypothesis predicts that MDRI values should be lower in women who seroconvert soon after parturition than in those who seroconvert later. Accordingly we compared MDRI estimates for women seroconverting during the first 9 months postpartum, with those seroconverting later.
In the ZVITAMBO trial, 9562 women who tested HIV negative at recruitment, within 96 h of parturition, were followed up at 6 weeks, 3 months, and then at 3-month intervals for up to 24 months postpartum. We estimated MDRI values, using nonlinear mixed modeling for BED and LAg, and Turnbull survival analysis for BRAI, 8 for women first testing HIV positive by 9 months postpartum, and others who seroconverted later. MDRI was defined here as the mean time during which subjects have an optical density, or avidity index, <C during a period T = 24 months postseroconversion. To qualify for the study, a case provided at least two HIV positive samples after seroconverting, with time between last negative and first positive HIV tests at most 120 days. All error limits are 95% confidence intervals.
At cutoff values (C) of 0.8 for BED, 1.5 for LAg, and 40% avidity index (AI) for BRAI, estimated MDRIs, using all seroconverting samples, were 192 (180–201; n = 96), 104 (98–110; n = 101), and 144 (128–160; n = 96) days, respectively. These were 33%, 32%, and 52% lower than published estimates of 287 (248–328), 152 (128–178), and 298 (262–338) days for respective assays of clade C samples. 1,3,6 Other analyses (data not shown) showed that MDRIs do not differ significantly with the estimation method.
MDRI estimates are a function of the estimated time of detection and this varies depending on the HIV test system employed. Kassanjee et al. used a Western blot to define infection 3 : the ZVITAMBO study employed two independent third-generation Elisa tests, with a Western blot tie-breaker, where Elisa results were discordant. 9 These two systems have associated diagnostic delays that differ only by about 5 days. 10 This difference is small compared with the differences of 154, 48, and 95 days for BRAI, LAg, and BED, respectively, between our estimates and those from the literature. 3
When ZVITAMBO data were divided into those seroconverting in the first 9 months or at 12 months or later postpartum, BED, LAg, and BRAI MDRIs for the former group were 185 (176–195; n = 65), 99 (92–106; n = 70), and 139 (115–164; n = 65) days, respectively. These were 7%, 13%, and 19%, respectively, shorter than those for the latter group: 195 (171–231; n = 31), 113 (101–126; n = 31), and 171 (153–189; n = 31) days, respectively. For all chosen values of C, MDRI point estimates were lower for women seroconverting in the first 9 months postpartum, although the differences were generally not significant at the 5% level of probability (Fig. 1). The small number of cases seroconverting >9 months postpartum limited the power of the statistical tests. It is noteworthy that the MDRIs for those in the late seroconverting group were still significantly lower than published estimates, consistent with the idea that their immunological responses had not returned to the levels typical of nonpregnant women.
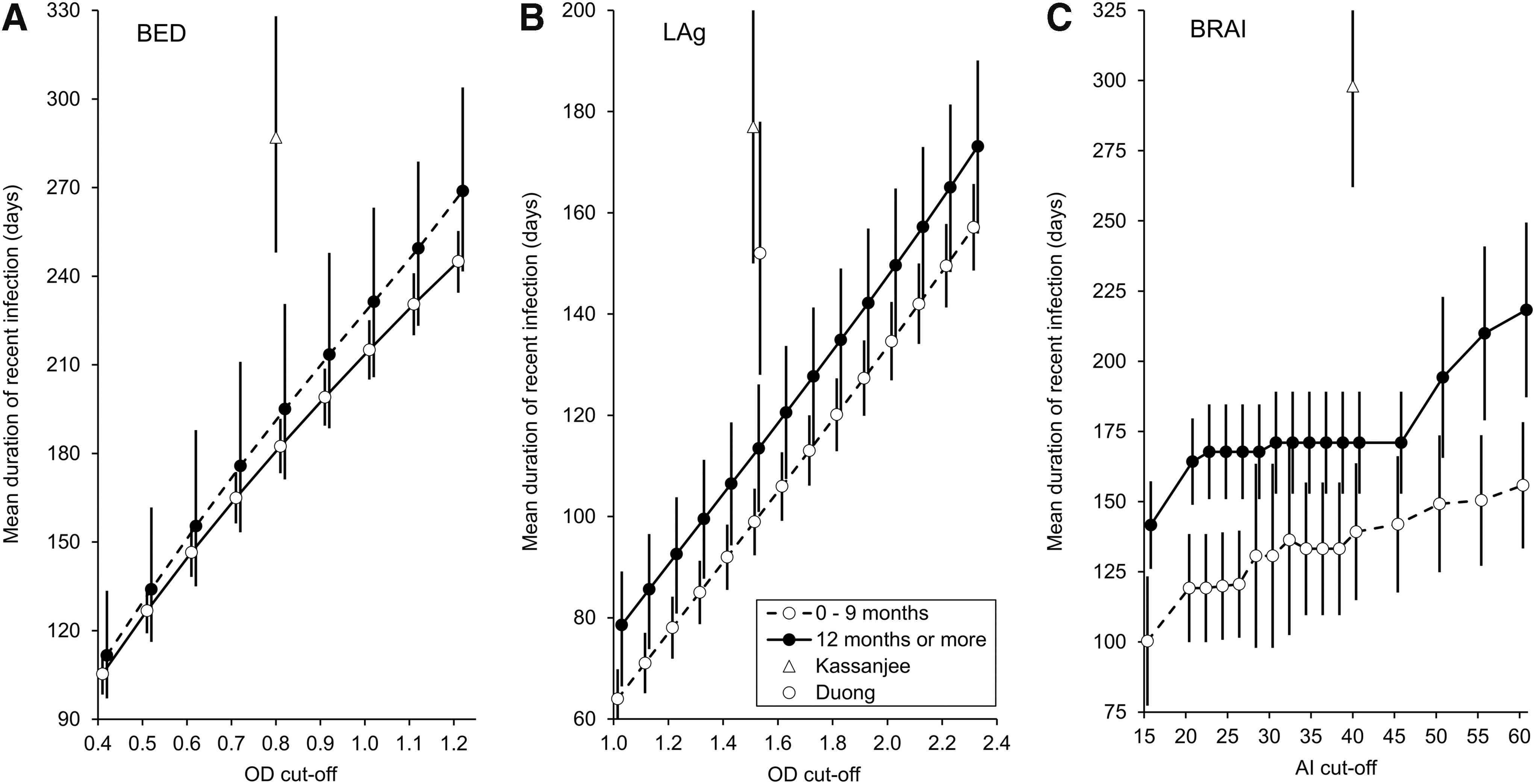
Mean duration of recent infection (MDRI) for the
Further work is required to establish more conclusively whether MDRI values for postpartum women are indeed systematically shorter than for other HIV positive cases in the population. What is clear, however, is the huge difference between our estimates and those from the literature. MDRI values estimated at different cutoffs (Fig. 1) emphasize that our MDRI point estimates, at the highest cutoffs investigated using BED and BRAI, and for LAg up to a cutoff of 2.0, are lower, for both subgroups analyzed, than published estimates at the much lower standard cutoffs.
We investigated whether the particularly short MDRI values might result from the vitamin A treatment given to half of the mothers. However, for ZVITAMBO participants, MDRIs for each of the three biomarkers differed by <10% between those receiving a large dose of vitamin A postpartum and those receiving a placebo: nor was there any significant difference between the MDRIs among primiparous and multiparous women.
Despite the tentative conclusion already reached, our findings are consistent with work showing that the postpartum period is characterized by heightened and activated innate and specific immune defenses, compared with nonpregnant women, and that these responses are accentuated in women who breastfeed, rather than formula feed, their infants. 7 In the ZVITAMBO situation, where 99.1, 94.0, and 59.1% of the women breastfed their babies for at least 6, 12, and 18 months postpartum, it is not then surprising that we find decreased MDRI values for women seroconverting during the first 9 months, relative to the second year, postpartum.
Pregnant women exhibit immunosuppression, relative to nonpregnant women, increasing the tolerance to fetal antigens. 11,12 This suppression involves, however, cell-mediated responses: it is unclear what happens to the humoral responses that would presumably affect MDRI levels. More work is thus required to estimate how MDRIs vary with physiological status.
Since incidence estimates change linearly with the inverse of the MDRI, serious errors in MDRI estimates will lead to significant errors in incidence estimates. Using our estimate of 196 days for the BED MDRI results in an HIV incidence, adjusted for a 4.8% false recent rate (FRR), of 3.5% (95% confidence interval 2.3–4.8) during the first 12 months postpartum in the ZVITAMBO trial. This is 34% higher than the incidence of 2.3% (1.5–3.2), resulting from the use of the published MDRI estimate of 287 days, 3 underlining the importance of ensuring the use of an appropriate MDRI value. The FRR was defined as the proportion of cases testing as recent infections, among those known to be HIV positive for more than 12 months
Reduced MDRIs among postpartum, compared with nonpregnant, women are consistent with heightened antibody responses after birth. This study provides a caution that we need to know how MDRIs vary by gender, physiological status, geographical region, ethnic group, and clade of virus.
Footnotes
Author Disclosure Statement
No competing financial interests exist.