
Abstract
Hypertension is a growing problem in the HIV population. The relationship between low nadir CD4 count and hypertension in the HIV-infected population has been reported. However, the effect of nadir CD4 on hypertension due to a different body mass index (BMI) is yet to be fully elucidated. In this cross-sectional study, 345 HIV-infected participants aged ≥40 years were recruited. They were frequency matched and compared with age, sex, and education with HIV-uninfected adults (n = 345). Hypertension prevalence was lower in HIV-infected than in HIV-uninfected participants (23.8% vs. 31.9%; p = .011), but this association was not significant after adjusting for potential confounders. Among HIV-infected individuals, older age, overweight, with a family history of cardiovascular diseases, and nadir CD4 count <50 cells/μl were independently associated with hypertension. Stratifying individuals with BMI category revealed that nadir CD4 count—regardless if it was operationalized as a dichotomous variable (<50 cells/μl) or continuous variable—was found to be associated with hypertension among individuals who were underweight and obese, but not among those who were normal weight and overweight. Among HIV-uninfected individuals, older age and having a waist circumference above cutoff were significantly associated with hypertension. This is one of the first studies to demonstrate that the association of nadir CD4 and hypertension is observed in underweight and obese HIV-infected patients. While these results suggest that the relationship between nadir CD4 count and hypertension might be mediated by body weight, future longitudinal studies will be needed to validate the findings, including its causal pathways.
Introduction
T
The existing literature reveals mixed findings on the prevalence of hypertension in HIV-infected versus HIV-uninfected individuals. Several studies observe a higher prevalence of hypertension in HIV-infected patients than HIV-uninfected individuals, 9,10 however, other studies find similar or lower prevalence of hypertension in HIV-infected patients. 11 –13 Such discrepancy may be due to the differences in weight and other common risk factors among the two types of individuals (HIV-infected vs. HIV-uninfected), as well as HIV disease and treatment characteristics.
HIV-infected individuals are at risk for hypertension due to traditional risk factors such as older age, smoking, and obesity, lipodystrophy, and other metabolic disorders due to HIV infection itself and adverse effects of anti-HIV drugs. 8,14,15 In addition, recent studies reveal an association between nadir CD4 count and hypertension in HIV-infected individuals. 14,16 The possible underlying mechanism is that low nadir CD4 count is associated with poor immune recovery, which in turn results in persistent immune activation, inflammation, endothelial dysfunction, and microbial translocation, 17,18 where all these have been postulated as contributing to the development of hypertension. 19 –21 However, research has shown that obesity is also associated with elevated levels of inflammation and immune activation among HIV-infected individuals. 22 –24 A recent study found that weight gain downregulates inflammation in underweight HIV-infected individuals but upregulates inflammation in obese individuals. 25 Such data encourage us to speculate whether the relationship between nadir CD4 count and hypertension may be dependent on weight as the impact of nadir CD4 count on hypertension is possibly attributed to inflammation. As the weight is a modifiable factor and easy to monitor, an understanding of these relationships may provide information for hypertension prevention among the HIV-infected population.
China launched its National Free Antiretroviral Treatment Program in 2002, and ∼38,200 received treatment in 2015. In 2016, China eliminated the CD4 threshold as a condition for treatment. For HIV-infected individuals, we predict that non-AIDS-related morbidity and mortality (especially age related) will became a major issue in China. 26 However, little is known about the prevalence of hypertension and associated factors among HIV-infected patients regardless of cART status comparable to the HIV-negative individuals in China.
Therefore, in this study, we aimed to investigate the prevalence of hypertension among middle-aged and older adults in China who are HIV infected versus HIV uninfected, and to identify factors associated with hypertension in the HIV population. Furthermore, we examined whether the association between nadir CD4 count and hypertension varied by different body mass index (BMI) categories among HIV-infected individuals.
Materials and Methods
Study setting and population
We used a cross-sectional design to collect data in Taizhou prefecture of Zhejiang province, China, as described previously. 27 Specifically, between June 2014 and May 2015, we consecutively recruited and enrolled 345 HIV-infected adults aged 40 and older who registered with the Chinese National Information System for AIDS Prevention and Control (CNISAPC). HIV-uninfected participants were recruited from persons receiving HIV voluntary counseling and testing clinics or receiving routine physical examination at the same Center for Disease Prevention and Control (CDC) during the study period, and were eligible if they were HIV negative at the enrollment (n = 1,216). For current analysis, 345 HIV-uninfected individuals were randomly selected and frequency matched to cases in 1:1 ratio according to sex, education, and 5-year age categories.
The study was approved by the Institutional Review Board (IRB) of Fudan University, Shanghai, China. Written informed consent was obtained from all study participants.
Antiretroviral therapy
In China, all HIV-infected individuals with a CD4 count of 200 cells/μl or World Health Organization stage 3 or 4 disease before 2008 were eligible for free standard three-drug antiretroviral therapy. In 2008, CD4 count threshold for treatment was increased to 350 cells/μl. 28 The first-line treatment regimens were stavudine (d4T) or zidovudine (AZT) plus lamivudine (3TC) plus efavirenz (EFV) or nevirapine (NVP). 28 Since 2010, d4T has been replaced with tenofovir (TDF).
Data collection
Participants were evaluated using a structured questionnaire to collect information such as age, sex, education, medical history of hypertension, and family history of cardiovascular diseases (e.g., hypertension, diabetes, and stroke). Physical examination of height, weight, waist circumference, hip circumference, and blood pressure (BP) was carried out after the questionnaire had been completed. A second measure of BP was taken and used if systolic BP was >135 mm Hg or diastolic BP >85 mm Hg. Otherwise, no further measurements were taken.
Hypertension was defined as systolic BP ≥140 mm Hg or diastolic BP ≥90 mm Hg, or current use of antihypertensive therapy with previous diagnosis of hypertension. Weight was categorized by BMI (kg/m2) as <18.5 (underweight), 18.5 to 23.9 (normal weight), 24 to 27.9 (overweight), and ≥28 (obese) using the Working Group on Obesity in China criteria. 29 The cutoff of waist circumference for abdominal obesity is 85 cm for men and 80 cm for women as defined by the Chinese Joint Committee for Developing Chinese Guidelines on Prevention and Treatment of Dyslipidemia in Adults. 30 The cutoff of waist to hip ratio (WHR) for abdominal obesity is 0.9 for men and 0.85 for women as recommend by the World Health Organization and other studies conducted in China. 31,32
HIV-related characteristics were extracted from the national HIV epidemiology and treatment databases. The nadir CD4 count was defined as the lowest ever measured CD4 count since the date of HIV diagnosis. The current CD4 count was defined as the most recent measured CD4 count (within 2 months before survey or within 1 month after survey).
Statistical analysis
Analysis was performed using SAS software (version 9.11). Differences between groups were assessed by χ 2 test or Fisher exact test for categorical variables, and by t-test or Mann–Whitney test for continuous variables, as appropriate. Univariable and multivariable logistic regressions were performed to explore the determinants of hypertension. Variables included in the multivariable model were those with p < .15 in univariable analysis. Backward selection was used with retention at a p < .10. Separate models were fit for nadir CD4 < 50 cells/μl or as a continuous variable in multivariable models.
Results
Characteristics of participants
This study included 345 HIV-infected and 345 HIV-uninfected individuals. In both groups, the mean age was around 52.7 years, 77.7% were male, and 53.0% had at least middle school education. The median of waist and hip circumferences was 82 and 90 cm in HIV-infected individuals and 90 and 94 cm in HIV-uninfected individuals, respectively. Compared with HIV-uninfected individuals, HIV-infected individuals had less waist circumference above cutoff (40.6% vs. 55.9%, p < .001), but more WHR above cutoff (62.0% vs. 54.2%, p = .037) and family history of cardiovascular diseases (32.7% vs. 23.5%, p = .007).
In terms of HIV-related characteristics, the median time since HIV diagnosis was 3.0 years and 10.4% had nadir CD4 < 50 cells/μl. Eighty-seven percent of HIV-infected participants were receiving cART with median treatment duration of 2.2 years, and 92.6% had a plasma HIV load of <400 copies/ml.
As shown in Table 1, HIV-infected individuals were less often overweight and obese (20.9% and 4.3%) compared to uninfected individuals (40.6% and 5.8%) (p < .001). In both HIV-infected and HIV-uninfected groups, male sex, waist circumference above cutoff, and WHR above cutoff were less common among underweight participants compared to normal weight, overweight, and obese participants. Furthermore, underweight HIV-infected participants had the disease for a longer period, lower median nadir CD4 counts, longer duration of treatment, and more prior d4T exposure compared to normal weight, overweight, and obese HIV-infected participants (Table 1).
Data are presented as no. (%), mean ± standard deviation, or median (interquartile range).
One HIV-uninfected individual was excluded from Table 1 because of missing weight measurement for BMI calculation.
≥80 cm/≥85 cm (women/men).
≥0.85/≥0.9 (women/men).
Data are for 231 HIV-infected participants.
Data are for 300 HIV-infected cART recipients.
BMI, body mass index; cART, combination antiretroviral therapy; d4T, stavudine; WHR, waist to hip ratio.
Prevalence of hypertension in HIV-infected versus HIV-uninfected individuals
HIV-infected individuals had a significantly lower prevalence of hypertension than HIV-uninfected individuals (23.8% vs. 31.9%; p = .011), and this association was observed in the same direction after adjusting for potential confounding variables, including age, BMI, waist circumference above cutoff, and family history of cardiovascular diseases, but was not significant (odds ratio [OR] = 0.75; 95% confidence interval [CI] 0.52–1.08; p = .119).
Correlates of hypertension in HIV-infected versus HIV-uninfected individuals
Among HIV-infected individuals, multivariable analyses revealed that older age (OR = 1.83; 95% CI: 1.37–2.46), being overweight (OR = 2.30; 95% CI: 1.37–6.19), family history of cardiovascular diseases (OR = 3.18; 95% CI: 1.81–5.57), and nadir CD4 count <50 cells/μl (OR = 2.35; 95% CI: 1.02–5.39) were significantly associated with the presence of hypertension. Of note, obesity (OR = 3.23; 95% CI: 0.93–11.20; p = .065) and waist circumference above cutoff (OR = 1.79; 95% CI: 0.95–3.38; p = .072) were marginally significantly associated with hypertension (Table 2). We repeated the analysis from Table 2 but treating nadir CD4 count as a continuous variable; nadir CD4 count (50 cells/μl) was not significant with hypertension in both univariable (OR = 0.95; 95% CI: 0.85–1.06; p = .393) and multivariable (OR = 0.90; 95% CI: 0.79–1.02; p = .109) models. In subgroup analysis restricted to those on ART only, older age, overweight, and family history of cardiovascular diseases remained significantly associated with hypertension (data not shown), but nadir CD4 count <50 cells/μl was marginally significantly associated with hypertension (OR = 2.20; 95% CI: 0.92–5.24; p < .078).
Variables included in the final multivariable models were those with a p < .15 at univariable regression analyses, and backward selection was used, with retention at p < .10
≥85 cm/≥90 cm (women/men).
≥0.85/≥0.9 (women/men).
CI, confidence interval; OR, odds ratio.
Among HIV-uninfected participants, in multivariable analysis, only older age (per 10 years) (OR = 1.49; 95% CI: 1.16–1.91) and waist circumference above cutoff (OR = 1.85; 95% CI: 1.07–3.17) were significantly associated with hypertension (Table 2).
Association between nadir CD4 count and hypertension by BMI category
Figure 1 depicts the prevalence of hypertension by HIV status and nadir CD4 count stratified by BMI category. Among underweight individuals, the prevalence of hypertension in HIV-infected individuals with nadir CD4 count <50 cells/μl was more than two times higher than those with nadir CD4 count of 50–199 cells/μl and HIV-uninfected individuals, respectively. None of the underweight HIV-infected individuals with nadir CD4 count ≥200 cells/μl had hypertension. Among both the normal weight and overweight individuals, the prevalence of hypertension was similar in all four groups. Among the obese individuals, the prevalence of hypertension was highest in HIV-infected individuals with nadir CD4 count <50 cells/μl and was lowest in those with nadir CD4 count ≥200 cells/μl.
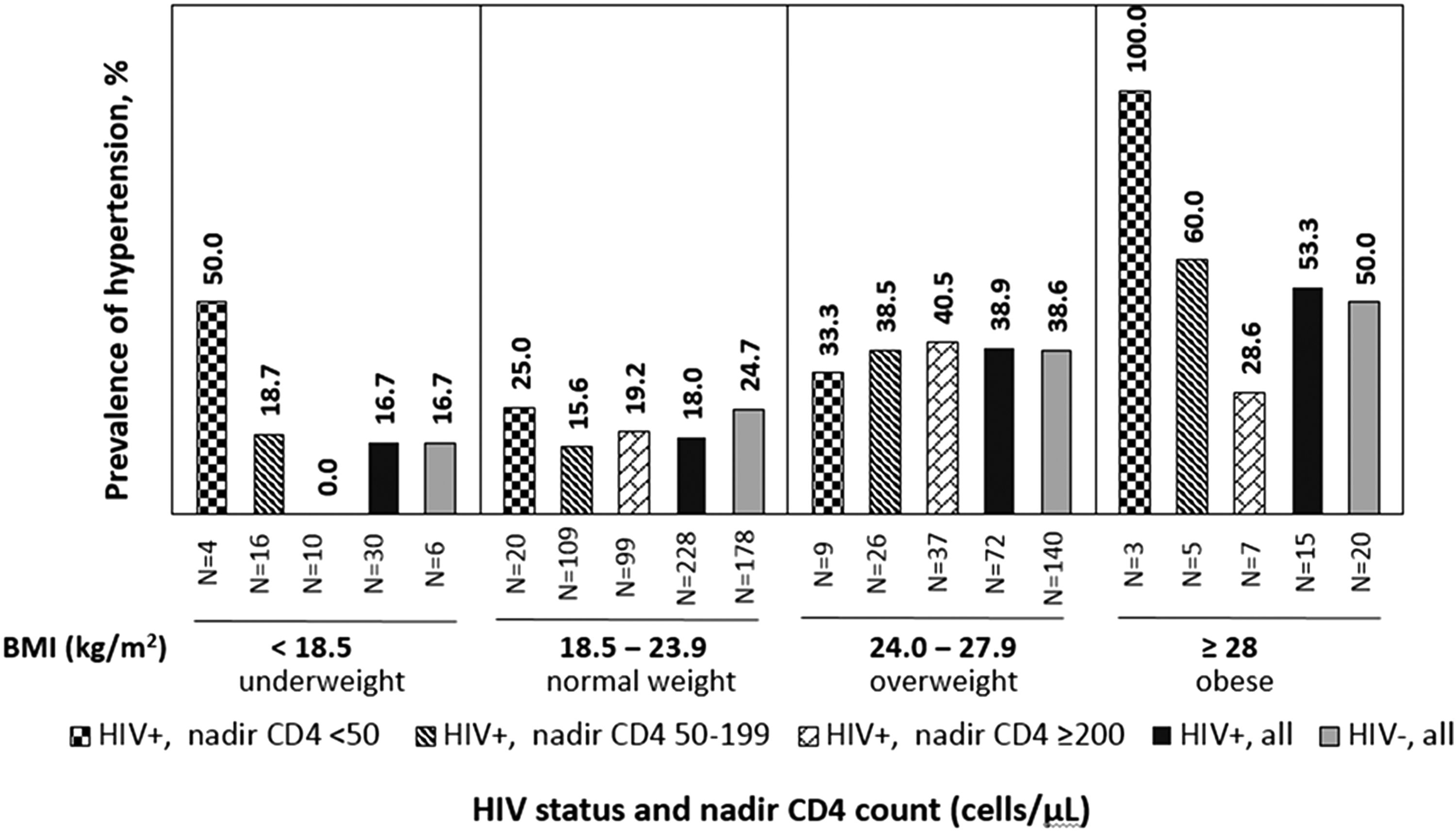
Prevalence of hypertension by HIV status and nadir CD4 count, stratified by BMI category at survey. BMI, body mass index.
We further evaluated the association of nadir CD4 count as a dichotomous (<50 cells/μl vs. >50 cells/μl) and as a continuous variable, respectively, with hypertension in the HIV-infected group within different BMI categories (Table 3). In the multivariable model adjusting for age only, among the underweight individuals with nadir CD4 count being operationalized as a dichotomous variable, it was significantly associated with hypertension, whereas when nadir CD4 count being operationalized as a continuous variable the association was marginal. Among the obese category, the OR for the association between nadir CD4 < 50 cells/μl and hypertension could not be estimated because all obese HIV-infected individuals with nadir CD4 count <50 cells/μl had hypertension; nadir CD4 as a continuous variables was not significantly associated with hypertension. Among both the normal weight and overweight individuals, both nadir CD4 count operationalized as a dichotomous and continuous variable was not associated with hypertension.
Adjusted for age only, as it is the potential confounder of the association between nadir CD4 count and hypertension.
OR cannot be estimated because all obese HIV-infected participants with nadir CD4 count <50 cells/μl had hypertension, as depicted in Figure 1.
In subgroup analysis restricted to patients on cART only, the multivariable model adjusting for age only revealed that nadir CD4 < 50 cells/μl remained significantly associated with hypertension among the underweight category only (OR = 18.0; 95% CI: 1.04–313.15; p = .047).
Sensitivity analysis
Considering that HIV-infected individuals with lower nadir CD4 count or underweight might be more anxious on the day of enrollment and thereby affecting the BP measurement, we repeated the analysis in HIV-infected individuals from Table 2. For this, we defined hypertension according to prior hypertension diagnosis (n = 27) to check the robustness of results. Furthermore, 55 patients who were diagnosed with hypertension according to BP measurement at enrollment but without a prior diagnosis of hypertension were excluded from analysis. In the multivariable model, nadir CD4 <50 cells/μl was no longer significantly associated with hypertension (OR = 1.96; 95% CI: 0.52–7.36; p = .318). However, when treating nadir CD4 as a continuous variable, it was marginally significantly associated with hypertension (OR = 0.80; 95% CI: 0.63–1.01; p = .064). In addition, older age, waist circumference above cut-off and family history of cardiovascular diseases were significantly independently associated with hypertension, as given in Table 2.
Discussion
Previous studies postulate that HIV infection may lead to accelerated aging, which may contribute to elevated hypertension in HIV-infected adults compared to age-matched uninfected adults. 10,11,33 In the present study, we found that HIV-infected individuals have a lower prevalence of hypertension than uninfected individuals—a finding also being observed in some earlier studies. 12,13 Nonetheless, our finding could be due to the fact that the proportion of being overweight or obese was significant higher among HIV-infected participants than their age-, gender-, and education-matched uninfected controls. Alternatively, it is possible that the duration of treatment was relatively short; thereby, the metabolic disorders associated with treatment are not common as those with long duration of treatment. It is anticipated that the prevalence of obesity will continue to increase in the HIV-infected population as indicated by some recent studies in Western countries, 34,35 the same phenomenon likely to occur in China as well.
Consistent with the global literature, 14,16 we observed that lower nadir CD4 count is independently associated with hypertension in HIV-infected individuals. After stratifying by BMI category, this association remained significant or marginally significantly in the underweight and obese groups, but was not apparent in the normal weight and overweight groups. The pattern is also noted in the prevalence of hypertension by HIV status and nadir CD4 category, showing that within the underweight and obese categories HIV-infected individuals with nadir CD4 count <50 cells/μl had the higher prevalence of hypertension than those with nadir CD4 counts of 50–199 and ≥200 cells/μl and HIV-uninfected individuals, but similar prevalence of hypertension in all groups. Taken together, these findings suggest a possibility that the impact of low nadir CD4 count on hypertension may be present only in HIV-infected adults who are underweight or obese. Research suggests that higher serum inflammation levels found in underweight or obese HIV-infected individuals may contribute to an increased likelihood of adverse health outcomes. 23 –25 It is possible that maintaining a healthy weight may ameliorate immune activation, inflammation, and/or endothelial dysfunction caused by low nadir CD4 count. However, given this was a cross-sectional study and the markers of inflammation were not measured, we cannot determine the temporal associations of change in weight, inflammation, and BP after treatment.
We did not find an association of cART status and treatment duration with hypertension. There is growing evidence that cART provides a beneficial effect on risk of cardiovascular diseases, through reduction of inflammation, immune activation, and endothelial dysfunction by suppressing HIV replication, 17,36 which may neutralize the adverse effect on metabolic changes, resulting in no significant association. 37 The other possible explanation is the short duration of treatment in the sample.
Previous literature demonstrated that many HIV-infected individuals, particularly those receiving cART, exhibit abnormal fat distribution, including peripheral fat atrophy and visceral lipohypertrophy. 38,39 The abnormal fat distribution is related to metabolic syndrome, which increases the risk of cardiovascular diseases, including hypertension. 40,41 Brown et al. found that waist circumferences increase more rapidly in HIV-infected than HIV-uninfected individuals, thus yielding a more rapid increase in the WHR among these individuals. 42 Indeed, our data indicated that HIV-infected individuals had a higher prevalence of WHR above cutoff than controls. It is interesting to note that HIV-infected individuals had lower waist circumference and hip circumference compared with controls, but difference in hip circumference was larger than difference in waist circumference between the two groups, resulting in the higher proportion of WHR above cutoff in the HIV-infected group. Consistent with prior studies indicating that waist circumference is a better predictive of metabolic syndrome and hypertension than WHR in the Chinese population, 31,43,44 we observed a positive association between waist circumference above cutoff and hypertension in both HIV-infected and HIV-uninfected individuals.
The positive association of overweight with hypertension is consistent with the literature. 8 We did not find such an association of family history of cardiovascular diseases among HIV-uninfected individuals. These findings are consistent with the known literature that family history of cardiovascular diseases is associated with acute coronary syndrome in HIV-infected individuals but not in HIV-uninfected individuals. 24
Our study had several limitations. This was a cross-sectional study, and hence, the temporality or causation between nadir CD4 count, BMI, and the development of hypertension could not be determined. Second, all participants were from a rural area of China and received cART for a relatively short period, and thus, generalizability for all the HIV-infected patients should be cautioned. Third, the small number of HIV-infected participants in the underweight and obese categories limited our ability to detect the significant differences in the association between nadir CD4 count and hypertension. Also, the observed prevalence of hypertension suffers from a large variance and may be overestimated. Fourth, hypertension in this study was operationalized using indicators taken in one visit, which could result in measurement bias. Nonetheless, there is low likelihood such measurement error was consistent, over- or underestimation of BP, and contributes to the interaction effect between BMI and nadir CD4 counts. Finally, other important components of the metabolic syndrome such as dyslipidemia and diabetes were not measured, therefore limiting our understanding of the underlying mechanism of metabolic disorders in the HIV-infected population.
In summary, the prevalence of hypertension is lower in HIV-infected than in HIV-uninfected adults in our study population. However, there are good reasons to expect an increasing prevalence of hypertension in HIV-infected adults in China because of the increasing weight and metabolic syndromes associated with early initiation of HIV treatment and prolonged duration on cART. It is unclear whether the beneficial effect of early cART initiation would be outweighed by the adverse effects of metabolic syndromes associated with cART. Our findings also suggest that past severity of impaired immune function, as indicated by low nadir CD4 count, appears to be relevant for the development of hypertension in HIV-infected individuals. Of note are the findings that the association of nadir CD4 and hypertension was present only in underweight and obese HIV-infected patients, raising the possibility that weight may play a mediating role between nadir CD4 and hypertension. Considering the cross-sectional design, future longitudinal studies will be needed to validate the findings and dissect causal relationships.
Footnotes
Acknowledgments
We thank all the participants. This work was funded by the Shanghai Municipal Health and Family Planning Commission (grant nos. GWTD2015S05, 15GWZK0101) and the Natural Science Foundation of China (grant nos. 81373062, 81402725).
Authors' Contribution
Y.D. and N.H. conceived and designed the study. Y.D. and H.L. supervised the participant recruitment and data collection. X.L. and Y.Z. recruited the participants and collected data. Y.D. analyzed the data and wrote the first draft of the manuscript. N.H., F.Y.W., Y.V.S., and V.C.M. contributed to data interpretation and writing of the manuscript.
Author Disclosure Statement
No competing financial interests exist.