
Abstract
Longitudinal studies of retention in care (RIC) and viral suppression (VS) in the southeastern United States (US), a region disproportionately affected by HIV infection, are lacking. HIV-infected adults with ≥1 medical visit at the Vanderbilt Comprehensive Care Clinic (Nashville, Tennessee) from 2004 to 2013 were included. RIC was ≥2 (a) laboratory dates [CD4+ counts or HIV-1 viral loads (VLs)] or (b) provider encounters and/or laboratory dates in the year of interest, ≥90 days apart. VS was a VL of <200 copies/ml at last measurement in the year of interest. Modified Poisson regression estimated relative risk (RR) of RIC and VS, adjusting for age, race, sex, HIV transmission risk, and socioeconomic status (SES). Among 4,641 persons, 76.8% achieved RIC and 70.2% achieved VS. RIC and VS increased from 2004 to 2013 (p < .001 each). For lack of RIC, younger patients (RR = 1.2 and RR = 1.1, 18–24 and 25–34 vs. 35–44 year-olds, respectively), Blacks (RR = 1.3 vs. Whites), and injection drug users (IDUs) (RR = 1.2 vs. heterosexual contact [Hetero]) fared worse (p < .05 each); those with male-to-male sexual contact fared better (RR = 0.8 vs. Hetero, p < .05). For lack of VS, younger patients (RR = 1.3 and RR = 1.2, 18–24 and 25–34 vs. 35–44 year olds, respectively), Blacks (RR 1.3 vs. Whites), Females (RR = 1.1 vs. Males), IDUs (RR 1.3 vs. Hetero), and those with low SES (RR = 1.1 vs. not low SES) fared worse (p < .05, each). RIC and VS increased over time, suggesting that efforts to improve outcomes have been effective. However, disparities persist and resources should focus on groups most at risk.
Introduction
A
Many previous HIV continuum of care studies have used cross-sectional study designs to measure and identify risk factors for poor retention and VS in a single year. 6 –12 However, cross-sectional studies may misestimate outcomes which are dynamic over intervals longer than the study period and may fail to capture temporal trends. A longitudinal study design that accounts for patients leaving and reengaging in care may more accurately describe long-term outcomes and elucidate disparities not evident with cross-sectional and serial cross-sectional studies. 10 –12
Few longitudinal continuum of care studies have included assessment of the agreement between laboratory-based and appointment-based retention. 13 However, retention measures which also include primary care provider visits regardless of laboratory testing may better describe engagement across the continuum, especially in subpopulations that require less robust surveillance such as those who have been in continuous long-term care, in high compliance, or with sustained VS. 14
Moreover, studies focused on HIV continuum of care outcomes in the Southeastern US are lacking. The Southeastern region of the US is disproportionately affected by the HIV epidemic, with the highest HIV incidence and prevalence of AIDS diagnoses, as well as the highest number of AIDS-related deaths. 14,15 Income inequality, as well as widespread stigma, is a prevalent social determinant of health in the South. In keeping with NHAS goals, the Southeastern US is an important region to focus efforts in reducing new HIV infections, improving health outcomes, and reducing HIV-related disparities. 2
We therefore sought to estimate RIC and VS longitudinally over 10 years among PLWH in care at a large, HIV primary medical home in the Southeastern US in an effort to monitor progress toward NHAS goals over time. In addition, we aimed to identify subgroups at risk for poor outcomes in an effort to monitor disparities over time. We sought to overcome the limitations of previous studies by utilizing a decade-long longitudinal design in which patients could enter, leave, and re-enter care as it occurs in real-world settings.
Materials and Methods
Study population
We conducted a retrospective observational cohort study among PLWH with ≥1 HIV healthcare provider appointment at the Vanderbilt Comprehensive Care Clinic (VCCC), in Nashville, Tennessee between January 1, 2004 and December 31, 2013. Observations in a patient's calendar year of death were excluded to ensure uniformity of risk for outcomes throughout the year; therefore patients who died during the same year as their first visit were excluded. This study was approved by the Vanderbilt University Institutional Review Board.
Data collection
Demographic, laboratory, medication, and appointment data were extracted from the electronic health record, including age at enrollment (categorized: 18–24, 25–34, 35–44, 45–54, 55–64, and ≥65 years), date of death, birth sex (male or female), race/ethnicity (categorized: White Non-Hispanic [White], Black Non-Hispanic [Black], Hispanic, and Other/Unknown), HIV risk factor (categorized: male-to-male sexual contact [MSM], injection drug use [IDU], heterosexual contact [Hetero], or other/unknown, including perinatal infection), socioeconomic status (SES, categorized: very low, low, or not low based on utilization of health insurance services with distinct income eligibility), CD4+ lymphocyte (CD4) values and dates, HIV-1 RNA viral load (VL) values and dates, and HIV healthcare provider visit dates.
SES was assessed each calendar year. Highly active antiretroviral therapy (HAART) was defined as receipt of antiretroviral regimens containing ≥3 agents, and HAART status was assigned in each calendar year (with receipt of ≥1 HAART regimen constituting access to HAART in that year). Patients were “low SES” if utilizing Tennessee's Ryan White program for medical services or drug assistance, including the Ryan White Insurance Assistance Program (IAP) (income eligibility threshold in Tennessee [TN] of ≤400% of the federal poverty level [FPL]). 16 Patients were “very low SES” if utilizing Medicare or Medicaid (income eligibility threshold in TN of ≤250% of the FPL). 17 Patients were “not low SES” if utilizing private or commercial insurance. Previous studies that used insurance alone as a proxy for SES in the post-antiretroviral therapy period have found associations between SES and poor HIV-related outcomes. 18,19 SES was assessed the year before the year in which RIC or VS was determined (i.e., lagged) to avoid reverse causation due to overlapping periods of ascertainment.
Outcomes
RIC and VS were both defined in keeping with CDC, Institute of Medicine, and NHAS definitions. 2,20,21 RIC was defined based on two data sources: (1) laboratory-based: ≥2 laboratory values (CD4 or VL) in calendar year of interest, ≥90 days apart; (2) laboratory and appointment-based definition: ≥2 HIV laboratory values or HIV healthcare provider visits in calendar year of interest, ≥90 days apart. VS was defined as ≥1 VL, with the last VL in calendar year of interest <200 copies/ml. VS was not conditioned on RIC. For example, a patient with a single visit or laboratory result would not be retained in a year; however, they could still be considered virally suppressed if they had a single VL and that single VL was <200 copies/ml. Patients with missing VL data were not included in the VS denominator in the pertinent calendar year.
Person-time was contributed from the date of VCCC enrollment until death date, loss to follow-up date, or last laboratory or healthcare provider visit date before study close. Loss to follow-up was the lack of a laboratory or healthcare provider visit during a calendar year without subsequent laboratory or healthcare provider visits during the study period.
Conversely, patients re-entering care with observations in a later year were not retained in care during gaps in care, but were included in population denominators during those years. To assess the sensitivity of our inferences to our definition of loss to follow-up, we performed a secondary analysis in which individual contributions of patient time differed from the primary analysis. Namely, patients were not censored after their final laboratory result or visit date during the study, but were instead assumed to be not retained and not virally suppressed after their final laboratory result or final visit date until the first of study close or death.
Statistical analysis
Modified Poisson regression provided unadjusted and adjusted relative risks (RRs) and 95% confidence intervals (95% CIs) for lack of RIC and lack of VS. 22 Negative outcomes were used in models so that increased risks for poor outcomes would be reflected by higher RR estimates. Generalized estimating equations were used to account for multiple outcomes per individual over time. Multivariate regression models adjusted for age at enrollment, current age, biologic sex, race/ethnicity, HIV risk factor, SES, calendar year of analysis, and time from enrollment (years). Calendar year of analysis and time from enrollment were modeled using a restricted cubic spline with four knots. To quantify temporal trends in the adjusted probability of retention and VS, marginal probabilities of the outcomes were extracted as the linear predictors from the fully adjusted model, set to mean covariate values.
Cohen's kappa (κ) and percent disagreement (complement of percent agreement) were used to measure concordance between laboratory-based and laboratory- and appointment-based retention measures. Missing SES was multiple imputed using current age, age at enrollment, sex, race, and HIV risk factor. 23 In secondary analyses, effect modification of the associations between outcomes and age, sex, race, and SES by calendar year, assessing the narrowing/expansion of disparities over time, was modeled using interaction terms for joint effects in fully adjusted models. All tests were two tailed and considered statistically significant if p < .05. Analyses were conducted using Stata 14.0 software (StataCorp, College Station, TX).
Results
Among 4,641 patients included, median age at enrollment was 38 years (interquartile range: 30–45), 76.7% were male, 38.1% were Black, Non-Hispanic, 52.3% reported MSM as HIV transmission risk factor, and 31.9% reported Hetero as HIV transmission factor (Table 1). SES was missing for 16.0% of person-years among 1,406 (30.3%) persons, but missingness significantly decreased over the study period (35% in 2004 to 1% in 2013). There were significant differences in missingness of SES by age, race, HIV transmission factor, and calendar year (Supplementary Table S1; Supplementary Data are available online at
Included individuals contributed 18,050 person-years to analyses.
Hetero, heterosexual contact; IDU, injection drug use; MSM, male-to-male sexual contact; SES, socioeconomic status.
Overall, 76.8% and 73.2% were retained in care using the laboratory-based and laboratory- and appointment-based definitions, respectively; 70.2% was virally suppressed. The proportion of patients retained in care and virally suppressed increased significantly over the study period. Laboratory-based RIC rose from 69.8% to 73.2% (p < .034) and from 72.3% to 82.2% using the laboratory- and appointment-based definition (p < .001); VS rose from 39.6% to 85.6% (p < .001). During the final 3 years of the study, VS surpassed RIC (85.6% vs. 82.2% in 2013, respectively, p = .006). The marginal probability of RIC and VS at the end of the study resembled the unadjusted proportions throughout the study period, reaching 82.0% and 85.5% by the end of the study, respectively (Fig. 1).
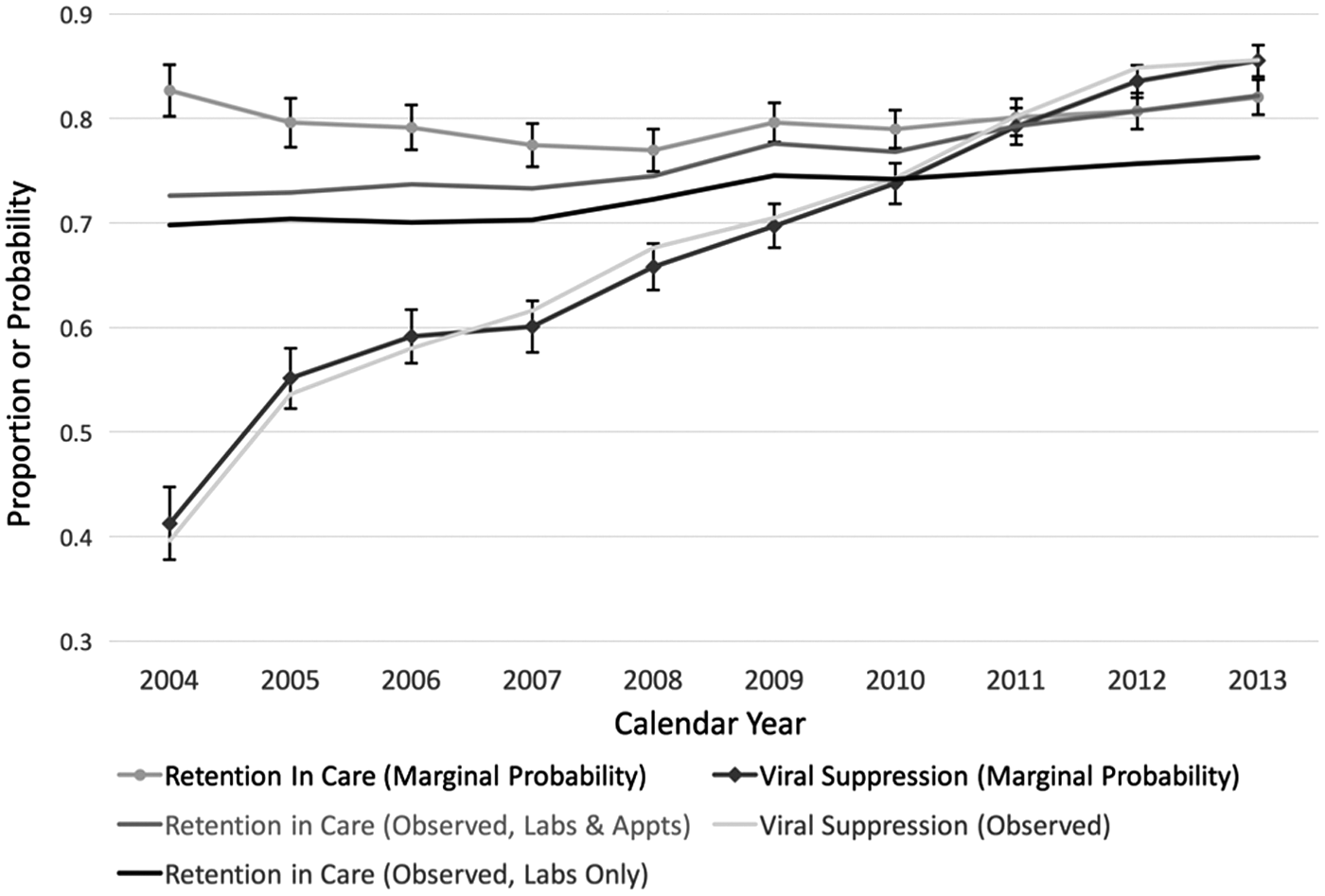
Marginal probabilities from adjusted regression models and observed proportions of retention in care and viral suppression, Vanderbilt Comprehensive Care Clinic, 2004–2013.
The laboratory-based retention measure significantly underestimated the proportion retained compared to the laboratory- and appointment-based measure, both overall and in each calendar year (overall percent disagreement = 3.6%, κ = 0.90, p < .0001). The percent disagreement between laboratory-only and laboratory- and appointment-based retention estimates increased from 2.8% in 2004 to 3.6% in 2013 (Table 2). Stratifying to assess whether HAART receipt may have influenced laboratory monitoring frequency and, therefore, retention proxy measures, the agreement between retention measures was similar among patients when receiving HAART (percent disagreement = 3.6%, κ = 0.88) and when not receiving HAART (percent disagreement = 3.6%, κ = 0.93).
p-value for comparison of laboratory-based and laboratory- and appointment-based measures of retention in care.
In adjusted regression using the laboratory- and appointment-based definition of poor retention, younger patients (<35 years of age) were more likely, and older patients (≥45 years of age) were less likely, to be not retained compared to patients 35–44 years of age. Compared to males, females were at lower risk of not being retained. Patients of Black, Non-Hispanic race were more likely to be not retained compared to White, Non-Hispanics, while Hispanics were less likely to be not retained. MSM patients were less likely to be not retained compared to Hetero patients. SES in the year prior was not associated with poor retention (Table 3).
All variables in the table were included in the adjusted analyses, as well as calendar year of analysis and time from enrollment (in years).
CI, confidence interval; RR, relative risk. Figures in bold indicate statistical significance (p < 0.05).
In adjusted analysis, younger patients (<35 year of age) were at higher risk, while older patients (≥45 years of age) were at lower risk, of not being virally suppressed compared to those 35–44 years of age. Females were at significantly increased risk of not being virally suppressed compared to males. Compared to Non-Hispanic Whites, Non-Hispanic Blacks were at significantly increased risk of not being virally suppressed. IDU patients were at significantly increased risk of not being virally suppressed vs. Hetero patients. Patients with low and very low SES were at increased risk of not being virally suppressed compared to those who were not Low SES (Table 3).
In secondary analyses examining effect modification of the associations between poor outcomes and age, sex, race, and SES by time, patients 18–24 (ratio of RRs = 1.0; 95% CI 1.0–1.1; ratio of RRs = 1.0; 95% CI 1.0–1.1) and 25–34 (ratio of RRs = 1.0; 95% CI 1.0–1.0; ratio of RRs = 1.0; 95% CI 1.0–1.0) years of age at enrollment expanded their deficits in retention and VS compared to those aged 34–45 over the study period, respectively, while those aged 55–65 (ratio of RRs = 0.97; 95% CI 0.94–1.0; ratio of RRs = 0.95; 95% CI 0.92–0.98) significantly improved upon their advantages over time.
The relative disadvantage of females compared to males with respect to poor retention decreased over time (ratio of RRs = 0.97; 95% CI 0.95–1.0) although their relative advantage in poor VS decreased slightly (ratio of RRs = 1.0; 95% CI 1.0–1.1). Similarly, compared to Non-Hispanic Whites, Non-Hispanic Blacks (ratio of RRs = 0.98; 95% CI 0.95–1.0) experienced a narrowing in retention disadvantage over time, but a widening of VS disadvantage (ratio of RRs = 1.1; 95% CI 1.1–1.1) (Table 4).
All variables in the table were included in the adjusted analyses, as well as calendar year of analysis and time from enrollment (in years). Figures in bold indicate statistical significance (p < 0.05).
In a sensitivity analysis in which patients were not censored for loss to follow-up after their final laboratory result or visit date, associations between age <35 and race and poor RIC lost statistical significance; however, the point estimates remained in the same directions. In addition, associations between female sex and poor VS lost significance although the point estimate remained in the same direction. All other adjusted associations were substantively similar to those from the primary analysis (Supplementary Table S2). There were no statistically significant differences in loss to follow-up status by either sex, Non-Hispanic Black race, MSM risk, or Very Low SES. Patients of younger age, of Hispanic ethnicity, IDU risk, and of Low SES were much more likely to be lost to follow-up by the end of the study (Supplementary Tables S3 and S4).
Discussion
In this population of HIV-infected persons in care in the Southeastern US, RIC and VS improved over a 10-year period. Although overall retention improved to 82.2% by 2013, more effort is needed to reach the NHAS goal of 90% by the year 2020. In 2011, among those successfully linked at the VCCC, the proportion virally suppressed surpassed the NHAS goal of 80% for year 2020. 2 VS among IDU surpassed 80% in 2011, while continuing to lag among young people (18–24 years), with only 78% reaching VS in 2013.
It is likely that improvements in antiretroviral therapy (ART), including reduced pill burden and improved tolerability, had an impact on HIV continuum of care outcomes. 24 In addition, several quality improvement projects were implemented at the clinic level aimed at improving retention and VS. 25,26 These include implementation of appointment reminders through phone call and text, as well as more enhanced medical case management, both of which have been shown to improve continuum of care outcomes. 26 –29 In addition, in recent years the Tennessee Department of Health (TDH) was awarded the Care and Prevention in the United States (CAPUS) Demonstration Project from CDC. 30 As part of CAPUS, the VCCC referred patients without a clinic visit or laboratory test in the previous 12 months to TDH staff who performed contact tracing and facilitated reengagement into HIV care.
Similar to prior work, we found that retention measures based solely on laboratory visits significantly underestimated retention compared to measures based on both laboratory and healthcare provider visits. Current guidelines for laboratory monitoring recommend VLs every 3 to 4 months and CD4s every 3 to 6 months during the first 2 years of ART. After 2 years, VLs may be obtained every 6 months, and CD4s yearly, if CD4 > 300 cells/μl and VLs are no longer needed once CD4 > 500 cells/μl. 31 Subpopulations that require less frequent monitoring may not be captured under current retention definitions that use laboratory measures as a surrogate marker for retention. Our data suggest that future RIC definitions which use laboratory measurements may need to be revised to be consistent with changing HIV laboratory monitoring guidelines.
Despite broad progress, we found disparities in these care continuum outcomes by age, sex, race, HIV risk factor, and SES, consistent with other studies. 32,33 When examining changes in retention and VS disparities over time, both progress toward goals and opportunities for improvement were identified. Although Non-Hispanic Blacks and females experienced a narrowing of retention disparities (compared to Non-Hispanic Whites and males, respectively) over time, significant gaps remained. In contrast, the disparity for retention widened over time for younger patients compared to older patients. The pattern of disparity for VS by age over time was similar to those for retention, but, alarmingly, both females and Non-Hispanic Black patients experienced a widening of VS disparities.
Although our primary models treated age, sex, and race separately, holding covariates constant and producing adjusted independent associations of each with respect to retention and VS outcomes, subanalyses stratifying by age-sex-race combinations (e.g., comparing outcomes among black males <30 years old to those of white males ≥30 years old, etc.) also identified younger black men and black women as having substantially poorer outcomes compared to older, non-black male and female cohort members.
Our analysis showed that patients of lower SES status have poor outcomes despite receiving care at a Ryan White-funded center. These outcomes may be attributed to unmeasured social and behavioral factors, including unstable housing, lack of transportation, and food insecurity. These results are consistent with findings in the current literature demonstrating a relationship between low SES and poor HIV outcomes, including an increased risk of death in the post-HAART period. 29,34,35 Our findings suggest that continued effort is required in eliminating socioeconomic barriers to care.
This study has several limitations. First, this is a single-center study; results may not be generalizable to other settings, either internationally or in other US regions. Second, we were not able to determine if patients classified as lost to follow-up had moved or transferred care. In the primary analysis, patients exiting and not returning to care before study end were considered lost to follow-up and therefore not included in population denominators, potentially leading to misclassification and underestimation of retention.
Third, patients without a VL in the year of interest were not included in the denominator for VS, which may have resulted in an overestimation of the proportion virally suppressed. However, sensitivity analyses in which out-of-care follow-up time was included for patients after clinic departure demonstrated that associations among age, sex, race, HIV risk factor, and SES were robust to alternate assumptions about patient care beyond direct observation. Point estimates from these analyses remained in the same direction, even if statistical significance was diminished. Fourth, the fact that missing SES status decreased over the study period may have led to a weak imputation model, with patterns from more recent years strongly influencing prediction of SES in earlier years. This change is most likely explained by improving data collection over the decade.
Fifth, we did not directly examine the effect of HAART receipt on laboratory measure frequency, which could theoretically alter the accuracy of laboratory-based metrics as valid proxies for visit-based retention. In this case, HAART receipt likely acts as a mediator and time-dependent confounder of the repeated outcomes of RIC and VS. However, >85% of our population were on HAART throughout their follow-up period, and there was very strong agreement between both retention metrics in our cohort, even when stratifying by HAART status. Therefore, it is unlikely that the inclusion of HAART status in our models would substantially alter our inferences. Finally, unmeasured confounders may have altered our inferences. These include lack of transportation, stigma, and housing instability, which are prominent in the Southeastern United States. 32,36
In conclusion, RIC and VS have improved over time in this population of HIV-infected persons linked to care in the Southeastern US. However, disparities among subgroups persist and limited resources and intensive interventions should be targeted at these high-risk subgroups to improve retention and VS outcomes. RIC should be measured both using laboratory measures and healthcare provider visits, and consideration should be given to revision of benchmarks to be consistent with recent changes in guidelines for laboratory monitoring. Further study is needed to investigate the association of additional key social and behavioral determinants of health that could be intervened upon to improve outcomes and decrease subgroup disparities.
Footnotes
Acknowledgments
This work was supported by the National Institutes of Health (K08 AI104352-Pettit) and the Tennessee Center for AIDS Research (P30 AI110527).
This work was presented in part at the 11th International Conference on HIV Treatment and Prevention Adherence, May 9–11, 2016, Fort Lauderdale, Florida, United States. Abstract #65.
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.