
Abstract
People who are asymptomatic and feel healthy, including pregnant women, may be less motivated to initiate antiretroviral therapy (ART) or achieve high adherence. We assessed whether ART initiation, and viral suppression 6, 12, and 24 months after ART initiation, were lower in HIV-infected members of serodiscordant couples who initiated during pregnancy or with higher CD4 counts. We used data from the Partners Demonstration Project, an open-label study of the delivery of integrated pre-exposure prophylaxis and ART (at any CD4 count) for HIV prevention among high-risk HIV serodiscordant couples in Kenya and Uganda. Differences in viral suppression (HIV RNA <400 copies/ml) among people initiating ART at different CD4 count levels (≤350, 351–500, and >500 cells/mm3) and during pregnancy were estimated using Poisson regression. Of 865 HIV-infected participants retained after becoming eligible for ART during study follow-up, 95% initiated ART. Viral suppression 24 months after ART initiation was high overall (97%), and comparable among those initiating ART at CD4 counts >500, 351–500, and ≤350 cells/mm3 [96% vs. 97% vs. 97%; relative risk (RR) 0.98; 95% confidence interval (CI): 0.93–1.03 for CD4 > 500 vs. <350 and RR 0.99; 95% CI: (0.93–1.06) for CD4 351–500 vs. ≤350]. Viral suppression was as likely among women initiating ART primarily to prevent perinatal transmission as ART initiation for other reasons (p = .9 at 6 months and p = .5 at 12 months). Nearly all HIV-infected partners initiating ART were virally suppressed by 24 months, irrespective of CD4 count or pregnancy status. These findings suggest that people initiating ART at high CD4 counts or due to pregnancy can adhere to ART as well as those starting treatment with symptomatic HIV disease or low CD4 counts.
Introduction
A
In known HIV serodiscordant couples, ART use has clearly identifiable treatment and prevention benefits. ART initiation, however, is commonly delayed among East Africans living with HIV and declines in adherence have been observed over time. 7,8 Personal barriers to accepting and adhering to ART include stigma and fear of side effects, and these can be exacerbated by structural barriers that include transportation costs and lengthy pretreatment processes. 9 –12 Providers have expressed a lack of motivation to initiate lifelong ART in asymptomatic healthy persons with high CD4 counts due to concerns about patient acceptance of ART, adherence, and stock-out of antiretroviral drugs stemming from unstable supply and funding levels. 13,14
Adherence is generally lower in chronic asymptomatic than symptomatic diseases, 15,16 because missing doses does not result in immediate physical symptoms. 17 Compared with symptomatic HIV-infected persons, asymptomatic individuals are significantly less likely to adhere to ART. 18 Adherence may also wane because healthy, asymptomatic persons are less motivated to take lifelong treatment. 19 In women who initiate ART during pregnancy, adherence may decline after delivery because of physical and psychological changes, stresses of newborn care, difficulties keeping appointments, and postpartum depression. 20,21 These factors may lead to poor adherence, disengagement from care, and the negative consequences of viral rebound, drug resistance, HIV disease progression, and eventually, mortality. 6,22
Prior studies have demonstrated inconsistent results. A systematic review of 30 studies in sub-Saharan Africa found no difference in virologic success after 24 months by CD4 threshold at ART initiation (86% among those with CD4 > 135 vs. 83% with CD4 ≤ 135 cells/mm3). 23 By contrast, viral suppression 24 months after ART initiation was significantly higher among those with CD4 ≥ 350 compared with <350 cells/mm3 (86% vs. 74%) in the UK Collaborative HIV Cohort Study. 24 Within a prospective interventional project among healthy East African HIV serodiscordant couples, in which ART was offered to eligible HIV-infected partners and pre-exposure prophylaxis (PrEP) to HIV-uninfected partners, we assessed ART initiation and effective adherence, as measured by viral suppression 2 years after ART initiation. Separately, we compared ART adherence among those who initiated ART at high CD4 counts and during pregnancy.
Methods
Study population and procedures
Between November 2012 and June 2016, we followed HIV serodiscordant couples enrolled in the Partners Demonstration Project (
At enrollment, HIV-infected partners were 18 years or older, ART naive, and did not have a history of WHO stage III or IV HIV disease. They were counseled about the treatment and prevention benefits of ART, and advised to start ART according to national guidelines. These guidelines changed during the study period: in 2012, they recommended ART initiation with a CD4 count ≤350 cells/mm3 or symptomatic HIV disease, and in 2014, they were updated to recommend ART initiation for all HIV-infected partners in serodiscordant partnerships, regardless of immunologic status, including pregnant and breastfeeding women. According to participant preference, ART provision occurred at the study site or through referral to an HIV clinic of the participant's choice. Follow-up study visits for HIV-infected participants were scheduled 4 and 12 weeks after enrollment in the study and every 3 months thereafter for up to 24 months. Data on ART eligibility and initiation were collected at each scheduled visit using semi-structured interviewer-administered questionnaires. When participant follow-up concluded, HIV care was transferred to a public health clinic of the participant's choice.
All participants received HIV primary care services, including risk reduction counseling, free condoms, and syndromic diagnosis, and treatment of sexually transmitted infections. Study services were provided by nurse counselors and clinical officers; medical officers provided backup and attended to complex cases. Study staff framed ART as a health preserving strategy. 27 The HIV prevention benefits of sustained ART use with high adherence were promoted as a commitment to the relationship and the HIV-uninfected partner. HIV-infected partners were counseled to initiate ART as soon as possible to decrease risk of HIV-related illnesses and HIV transmission. Daily ART adherence was encouraged without breaks to protect against selection of antiviral resistance. With the integrated PrEP and ART strategy, HIV-uninfected partners were offered PrEP for the time period leading up to the ART initiation of HIV-infected partners (if any) and for ∼6 months after ART initiation while the process of viral suppression was ongoing. 25 We performed CD4 testing using flow cytometry (BD Biosciences), and plasma HIV RNA quantification using COBAS AmpliPrep/COBAS TaqMan HIV-1 test (Roche Diagnostics) at enrollment and every 6 months thereafter. Results from plasma viral load testing were incorporated into counseling on ART adherence at the next quarterly visit. Urine pregnancy testing for all women was performed when clinically indicated.
Statistical analysis
The primary outcome was the proportion achieving viral suppression (plasma HIV RNA level <400 copies/ml) by 6, 12, and 24 months after ART initiation. The cumulative probability of ART initiation was estimated using Kaplan–Meier methods. Follow-up time was counted from the date of ART eligibility to date of self-report of ART initiation. Analyses of viral suppression included only persons with plasma HIV RNA testing by 6, 12, and 24 months after initiation. In sensitivity analyses, we repeated our primary analysis by including subjects with missing viral loads, or lost to follow-up, as virally nonsuppressed. In addition, we calculated (1) the proportion of eligible HIV-infected persons initiating ART and (2) retention in care at 6, 12, and 24 months after ART initiation (among those who had not yet completed study follow-up). The proportion with plasma viral suppression among people initiating ART at different CD4 counts (≤350, 351–500, and >500 cells/mm3) and during pregnancy was estimated using Poisson regression with robust standard errors. Among pregnant women, the analysis examined viral suppression 6, 12, and 24 months after ART initiation in case of any effects of pregnancy on viral load due to hemodilution. 28 All analyses were conducted using SAS software, version 9.4 (SAS Institute).
Ethical approval
The Human Subjects Division at the University of Washington and ethical review committees for each study site approved the study protocol. Each participant provided independent written informed consent in English or his or her preferred language.
Results
Participant characteristics
A total of 1,013 HIV-infected partners (613 from Kenya and 400 from Uganda) were followed in the Partners Demonstration Project. Retrospectively, 106 were found to have a viral load <400 copies/ml at study screening and 3 were using ART at enrollment and excluded from this analysis. Of the remaining 904, 596 (66%) were women, 95% were married, and the median age of HIV-infected women and men was 26 years [interquartile range (IQR), 22–30] and 36 years (IQR, 30–42), respectively (Table 1). Most (67%) reported condomless sex and 6 (1%) women and 30 (10%) men reported sex with an additional partner in the month before enrollment. The median CD4 count and HIV RNA plasma concentration in HIV-infected women and men at enrollment was 432 (IQR 277–621) and 399 (IQR 219–565) cells/mm3 and 4.5 (IQR 4.0–5.0) and 4.9 (IQR 4.5–5.3) log10 copies/ml, respectively.
IQR, interquartile range; WHO, World Health Organization.
ART initiation and viral suppression
All 904 HIV-infected participants became ART-eligible during the 2-year study period. Three were chronically lost to follow up, and thus did not receive a recommendation to initiate ART from the study clinicians. The cumulative probabilities of initiating ART at 6, 12, and 24 months after receiving an ART recommendation were 86%, 94%, and 98%, respectively (Fig. 1). Of 865 retained after becoming eligible for ART during study follow-up, 824 (95%) initiated ART (Fig. 2). Of these, 23, 113, and 442 completed their planned follow-up before 6, 12, and 24 months had elapsed. Of the 791, 691, and 360 participants who remained with time in the study and attended visits 6, 12, and 24 months, respectively, after their ART initiation, plasma HIV RNA results were available for 764 (97%), 679 (98%), and 358 (99%). Among those retained and with viral load results, 91% were virally suppressed 6 months after initiating ART (90% of women and 94% of men), 95% by 12 months after initiating ART (93% of women and 98% of men) and 97% by 24 months after ART initiation (97% of women and 97% of men) (Table 2). In a sensitivity analysis, when those without viral load results or lost to follow-up were considered as not having achieved viral suppression, the proportion virally suppressed 6, 12, and 24 months after ART initiation was 87%, 90%, and 91%, respectively (Fig. 2).
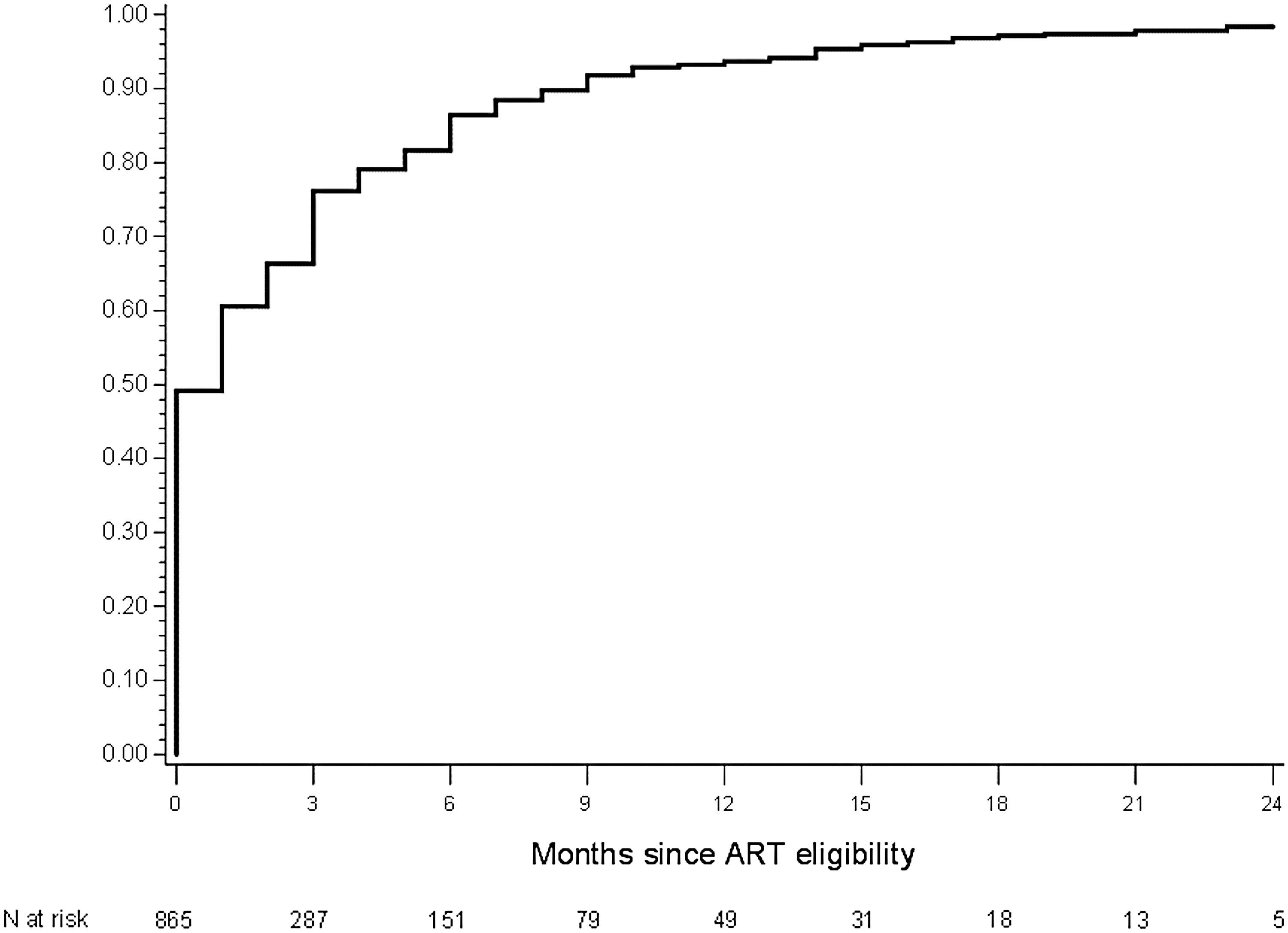
Cumulative probability of ART initiation. ART, antiretroviral therapy.
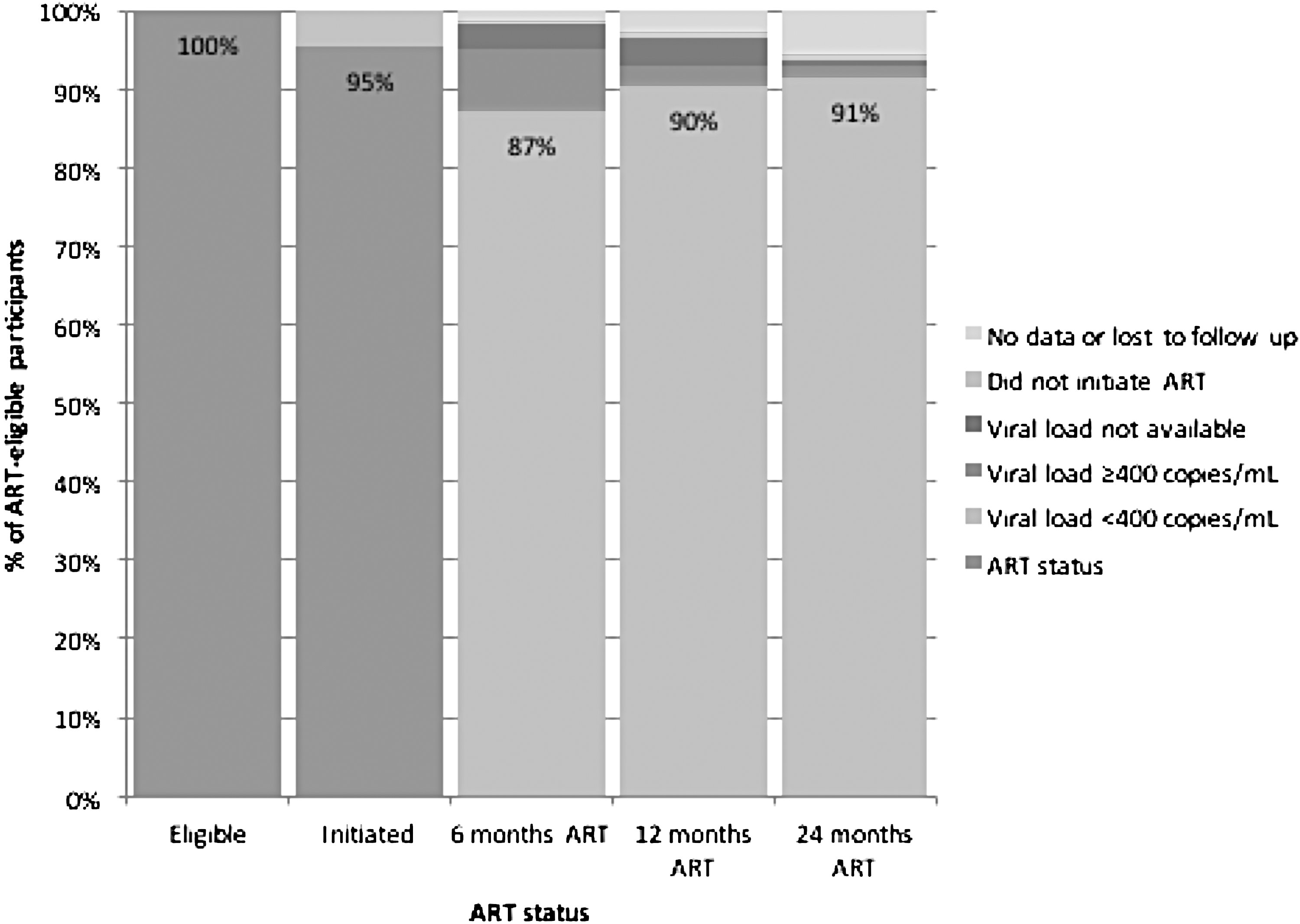
HIV care cascade.
Adjusted for study site.
Type 3 p-value for the composite null hypothesis that CD4 > 500 and 351–500 levels have the same effect on viral suppression as CD4 ≤ 350 cells/mm3.
ART, antiretroviral therapy; CI, confidence interval; RR, relative risk.
CD4 count and ART use
Of the 824 ART initiators, 264 (32%) had CD4 > 500 cells/mm3 when they first received a recommendation to initiate ART from a study clinician (Table 2). The median time from ART eligibility to ART initiation was 25 days (IQR 2–85): 13 days (IQR 1–39) for those with CD4 ≤ 350 cells/mm3 and 75 days (IQR 7–148) for those with CD4 > 500 cells/mm3. Viral suppression after ART initiation was similar across CD4 count groups: 92% versus 90% [relative risk (RR) 1.01; 95% confidence interval (CI): 0.96–1.06] by 6 months, 96% versus 89% (RR 1.01; 95% CI: 0.97–1.05) by 12 months and 96% versus 97% (RR 0.98; 95% CI: 0.93–1.03) by 24 months for CD4 counts >500 compared with ≤350 cells/mm3. Comparisons for CD4 351–500 versus ≤350 cells/mm3 were similar. We did not observe meaningful differences in loss to follow-up by CD4 count at treatment initiation. The proportion lost to follow-up was 1% by the time of the 6-month visit, 2% by the time of the 12-month visit, and 3% by the time of the 24-month visit.
Pregnancy and ART use
Of 596 HIV-infected women, 45 (8%) initiated ART solely because of incident pregnancy during the study. The median time from their first recommendation from a study clinician to initiate ART to treatment initiation was 24 days (IQR 2–84): 4 days (IQR 0–23) for pregnant women, and 27 days (IQR 5–84) for nonpregnant women. The prevalence of viral suppression was similar among pregnant and nonpregnant women by the 6-month (91% vs. 90%), 12-month visits (95% vs. 92%), and 24-month visits (100% vs. 97%; p > .05 for all comparisons).
Discussion
In a large prospective study of high-risk East African HIV serodiscordant couples, 98% of HIV-infected partners initiated ART by 24 months and 97% achieved viral suppression within 24 months. Rates of ART uptake and viral suppression were similar among people initiating at CD4 counts above and below 500 cells/mm3. Viral suppression did not wane among women who initiated ART due to pregnancy; pregnant women on ART were as likely to be virally suppressed 12 months after receipt of ART than women who initiated ART for other indications.
We did not observe differences in viral suppression by CD4 count at treatment initiation despite concerns that asymptomatic HIV-infected persons with high CD4 cell counts may not be as motivated to take ART. Our findings are comparable with a South African study, 29 in which the proportion virally suppressed in the CD4 > 500 and ≤500 cells/mm3 groups after 18 months of ART was similarly high at ∼100% versus 94%, respectively, and with the START trial in which achieving viral suppression 12 months after initiation was nearly universal. 1 The overall proportion achieving virologic success after 24 months of ART in our study (97%) is similar to that reported from six cohort studies in sub-Saharan Africa, 30 –35 in which >90% achieved viral suppression. A CD4 count >500 cells/mm3 is generally reflective of a healthy state, and thus ART initiation during this time is more likely motivated by a desire to preserve health, care for family, continue working, and prevent HIV transmission rather than a need to overcome overt illness and symptoms that are more common with lower CD4 counts. 36,37 With our counseling, we strived to overcome the perception that ART is only indicated for symptomatic persons by emphasizing its health-preserving benefits and normalizing ART use while healthy, rather than delaying until symptomatic. 27 Sharing of viral load results may have encouraged ART adherence and improved virologic outcomes. 12
Women who initiated ART during pregnancy were as likely to achieve viral suppression after 12 months of treatment than women who initiated ART for other reasons. ART adherence during pregnancy and breastfeeding is often motivated by maternal concerns about perinatal HIV transmission as well as a desire to improve own health. 38,39 Some cohorts of pregnant women have seen declines in adherence after delivery due to changing motivation for treatment, lifestyle changes, stresses of newborn care, and postpartum depression. 40 –43 Other work has found no difference in HIV RNA levels between pregnant and nonpregnant women using ART suggesting pregnancy has no effect on the virologic or immunologic response to ART. 44,45 Pregnant women in our study received counseling about ART benefits beyond those for reducing perinatal transmission, and may have benefited from increased partner support and counseling about adherence during the postpartum period to anticipate and overcome adherence challenges during this time. For women delaying ART initiation due to personal concerns, preparing for the birth of a child can be an opportunity to optimize personal health, and pregnant women can be counseled about the clinical and prevention benefits of ART.
Our results suggest that ART initiation need not be deferred in asymptomatic healthy persons with high CD4 counts due to concerns about poor adherence to lifelong therapy. Although ART may be deferred on a case-by-case basis because of concerns about lack of readiness to start ART, patient preferences, or structural barriers, 13 people meeting national ART guidelines should be counseled and considered for a recommendation to initiate treatment as soon as possible. 46 Counseling can prioritize messages that ART is recommended to reduce risk of sexual transmission of HIV, and high adherence is required for ART effectiveness. When appropriate, a recommendation for couples based counseling and testing can foster support for mutual disclosure and improved outcomes for ART use and HIV prevention. 47
The strengths of our study include the large multinational cohort of high-risk HIV serodiscordant couples, the heterogeneity of urban and peri-urban HIV research clinics where HIV-infected persons received counseling and ART, use of viral load results to motivate ART adherence in a setting where HIV RNA monitoring was not standard-of-care at the time of the study, and the comparison of virologic outcomes in pregnant and nonpregnant women. Our study has a number of limitations. We enrolled healthy HIV-infected persons in HIV serodiscordant partnerships, which may limit generalizability of our findings to other high risk populations. Participants received HIV care at clinical trial research clinics as well as public health clinics, and it is possible that heterogeneity of care in the geographic region influenced our results (i.e., clinic burden, quality of clinical services). Additionally, the short duration of post ART follow-up may limit the generalizability of our findings to present day situations with high penetration of ART availability for pregnant women.
In conclusion, nearly all women and men in serodiscordant relationships, many initiating lifelong ART at high CD4 counts and with asymptomatic disease, were virally suppressed after starting treatment, regardless of CD4 count or pregnancy status at initiation. Our study indicates that high ART uptake and adherence can be achieved among key populations at risk for HIV transmission, and supports WHO guidelines for initiating ART among all HIV-infected persons immediately after diagnosis.
Footnotes
Acknowledgments
We thank the couples who participated in this study for their motivation and dedication and the referral partners, community advisory groups, institutions, and communities that supported this work. The Partners Demonstration Project was funded by the National Institute of Mental Health of the U.S. National Institutes of Health (grant R01 MH095507), the Bill & Melinda Gates Foundation (grant OPP1056051), and through the generous support of the American people through the U.S. Agency for International Development (cooperative agreement AID-OAA-A-12-00023).
Partners Demonstration Project Team: Coordinating Center (University of Washington) and collaborating investigators (Harvard Medical School, Johns Hopkins University, Massachusetts General Hospital): Jared Baeten (protocol chair), Connie Celum (protocol co-chair), Renee Heffron (project director), Deborah Donnell (statistician), Ruanne Barnabas, Jessica Haberer, Harald Haugen, Craig Hendrix, Lara Kidoguchi, Mark Marzinke, Susan Morrison, Jennifer Morton, Norma Ware, Monique Wyatt.
Project Sites: Kabwohe, Uganda (Kabwohe Clinical Research Centre): S.A., E.T.; Kampala, Uganda (Makerere University): E.K., N.B.; Kisumu, Kenya (Kenya Medical Research Institute): E.A.B., J.O.; Thika, Kenya (Kenya Medical Research Institute, University of Washington): N.M., K.N.; Data Management was provided by DF/Net Research, Inc. (Seattle, WA). PrEP medication was donated by Gilead Sciences.
These data were reported, in part, at the 11th International Conference on HIV Treatment and Prevention Adherence, May 9–11, 2016, Fort Lauderdale, FL (abstract no. 43).
Author Disclosure Statement
The authors report no conflicts of interest. The contents are solely the views of the authors and do not necessarily represent those of the funding organizations. Gilead Sciences donated the PrEP medication but had no role in data collection or analysis. The results and interpretation presented here do not necessarily reflect the views of the study funders.