
Abstract
Universal antiretroviral treatment with sustained viral suppression benefits patients and reduces HIV transmission. Effectiveness of therapy may be limited by antiretroviral drug resistance. Information on the resistance profile at treatment failure and its impact on antiretroviral drugs may subsidize subsequent treatment strategies. Partial pol sequences from 319 patients failing first-line therapy were analyzed for resistance associated mutations (RAMs) and HIV subtype. Demographic data, CD4 T cell count, viral load, and antiretroviral regimens and mutational profile at first-line failure were also investigated for associations to the response to second-line regimens. RAMs at the reverse transcriptase gene were frequent. Most sequences (88%) showed at least one mutation. A higher number of reverse transcriptase RAMs were associated to lower CD4 T cell counts and the use of tenofovir/lamivudine in first line. Among 205 with follow-up data, 76.6% were virally suppressed (below 200 copies/ml) after 24 weeks of second-line therapy. Most cases initiated second line with a regimen genotypic susceptibility score ≥2, but it did not predict viral suppression, that was independently associated with higher CD4 T cell counts and with the presence of nucleos(t)ide analog reverse transcriptase inhibitor (NRTI) RAMs. This study documented extensive resistance at first-line failure in this area in Brazil, highlights the risks of low CD4 T cell counts to second-line therapy, and supports the notion that recycled NRTIs may contribute to viral suppression even when genotypic resistance is present.
Introduction
U
Highly active antiretroviral combinations have been freely available through the Brazilian health system since the late 90s. Currently, about half a million patients are on ART in the country. Genotypic resistance tests and viral load are provided by the public health system to guide second-line and subsequent salvage regimens. 3
From 2004 to March 2017, the Brazilian guidelines have recommended an efavirenz (EFV)-based regimen as first-line treatment. In 2013, tenofovir (TDF) replaced zidovudine (AZT) as the preferred nucleos(t)ide analog reverse transcriptase inhibitor (NRTI) to be combined with lamivudine (3TC). 3 Nevirapine (NVP), ritonavir boosted atazanavir (ATV/r), and lopinavir (LPV/r) were available in special situations, including pregnancy, intolerance, or contraindications to the preferred regimen. Recently the integrase inhibitor dolutegravir became the recommended drug to be used with TDF/3TC in first-line therapy, with darunavir/r added as an alternative protease inhibitor (PI).
Data on HIV resistance profile in patients failing first-line regimens in Brazil are limited. In a study evaluating genotype reports from five cities, the authors found a high prevalence of resistance associated mutations (RAMs) after first-line failures, including M184V/I in 70% and K103N in 42% of cases. 4 Proportions of NRTI RAMs as high as 80% for M184V/I were observed in northern Brazil, but in this analysis patients who had failed two or more regimens (76% of the cases) were included. 5 Similarly, studies in Asia and Africa found a high prevalence of RAMs after first-line failure. 6,7 A French nationwide study, including patients with two consecutive viral load measures over 50 copies/ml, showed a somewhat lower resistance prevalence (56%), but information on the number of previous regimens was not available. 8 A comparable proportion of resistance (52%) was observed in patients failing the first-line regimen in China. 9 In both studies, patients were likely to be at early stages of failure when genotyping tests were performed. Since the mid-2000s, a decrease in resistance has been recorded in the United States 10 and France. 8 In Brazil, the assessment of 2.115 HIV-1 sequences from patients failing ART from 2002 to 2012 showed a decrease in the prevalence of PI and NRTI resistance, in contrast to an increase in resistance to non-nucleoside reverse transcriptase inhibitor (NNRTI), mainly due to K103N. 11
Evidence on the impact of RAMs on the efficacy of second-line regimens was also limited until recently, when three large randomized studies consistently showed that NRTI mutations do not compromise NRTI-based second line success. 12 –14 In contrast, lack of adherence, high viral load, 12,13 and low CD4 T cell counts 15 were strong predictors of second-line failure in randomized, as well as in observational, studies.
Data on the HIV mutational profile after first-line ART failure and correlates of second-line outcomes in real-life context in Brazil are scarce. In this study we evaluated viral drug resistance in 319 patients failing first-line ART in the state of São Paulo and their 24-week response to the second-line regimen.
Materials and Methods
The retrovirus laboratory of Adolfo Lutz in São Paulo, Brazil generated 458 pol sequences from patients failing their first antiretroviral regimen between 2013 and 2015. Sequences were analyzed for RAMs using the HIVdb algorithm v7.0.1 (Stanford University HIV Drug Resistance Database). A report was sent to the clinical services to subsidize treatment decision. We reviewed the national antiretroviral dispensing database (SICLOM) for each patient to confirm treatment history at sample collection. As this system was introduced and became consistently used by different clinical units at different time points, cases with an HIV diagnosis preceding ART initiation in more than 1 year were considered as having potential previous treatment exposure and were retained in the dataset but excluded in some analyses. Efforts were made to carefully review available documents and electronic systems to confirm information on treatment history provided by the assistant physicians at request forms and to obtain data on the virological and immunological outcomes. Patients with inconsistent incomplete information or with evidence of previous exposure to ART were excluded. We also reviewed viral load and CD4 T cell databases to identify cases with possible undocumented ART (e.g., changes over 0.5 log10 in viral load along with consistent CD4 T cell gains). These cases were excluded, as well as those with conflicting clinical information, with 319 cases with viral failure (viral load above 200 copies/ml after 6 months on treatment) included in this study. We then recorded the second-line regimen and dispensation date and searched the laboratory database for the first available CD4 T cell count and viral load measurements after 24 weeks of the recorded date. Cases were henceforth anonymized.
All sequences were generated from retrotranscribed plasma RNA, extracted with QIAamp Viral RNA Mini Kit (Qiagen, Germany) or a M2000 extractor (Abbott). A reverse transcriptase (RT)-polymerase chain reaction (PCR) was performed using commercial kit (TRUGENE; Siemens) or with a previously described “in-house” protocol. 16 Briefly, a one-step RT-PCR, using High Fidelity Taq platinum and SuperScript III, was followed by nested PCR and Big Dye (Life) incorporation, resolved in an ABI 3130XL.
Sequences were edited with Sequencer 4.7 software (Gene Codes) and/or with RECall (
CD4 T cell counts were performed by flow cytometry (BD) and HIV viral load by real time quantitative PCR (Abbott) after July 2013. Versant HIV-1 RNA 3.0 Assay (bDNA; Siemens) was used before July 2013. Viral load determination on samples collected for genotyping was performed at our reference laboratory. CD4 T cell counts and additional viral load determinations were performed at one of the national viral load/CD4 laboratories.
Virological response was dichotomized according to Department of Health and Human Services (DHHS) metric as suppressed (below 200 copies/ml) or viremic. 18 To evaluate the significance of dichotomous variable, we used two-tailed Fisher or Yates corrected, as appropriate (Epi6, CDC). Mann–Whitney was used to compare variables from two groups, Kruskal–Wallis for three or more groups, and Spearman correlation to evaluate two continuous variables (Stata 8; Stata Corporation). Logistic regression (Stata 8) was used to evaluate independence of associations, with variables included in the regression when the unadjusted significance was below 0.2. The study was approved by Institutional Committee (IAL84d2010) and Ethics Committee (CEP-IAL/0032010).
Results
Our laboratory generated 2,629 partial pol sequences from July 2013 to December 2015. Test request forms allowed for selection of 458 patients referred for testing due to first-line treatment failure. After exclusion of 139 cases with incomplete or conflicting information, 319 patients failing first-line therapy were available for analyses.
Most participants (71%) were men, and the median age was 40 years old (interquartile range [IQR] 32–48), with 12 cases below 12 years of age. Most patients were asymptomatic at collection. Fifty-nine cases (17%), although included as failing first line, started follow-up before electronic database could rule out previous nondocumented ART exposure and were excluded in some analyses (see Mutations according to first-line regimen section). Subtype B (74%) predominated and followed subtype F (11%), BF recombinants (8%), and subtypes C (6%). Two BC recombinants and one AG recombinant were also identified. Demographic and laboratory data available at genotype test collection are shown in Table 1.
PI used included LPV or ATV, with ritonavir boost.
Other regimens: EFV/AZT/DDI; AZT/DDI; EFV/ABC/3TC; LPV/ABC/3TC; ATVr/ABC/3TC.
Results expressed as median and IQR.
3TC, lamivudine; ABC, abacavir; ART, antiretroviral therapy; ATV, atazanavir; AZT, zidovudine; DDI, didanosine; EFV, efavirenz; IQR, interquartile range; LPV, lopinavir; NNRTI, non-nucleoside reverse transcriptase inhibitor; NRTI, nucleos(t)ide analog reverse transcriptase inhibitor; NVP, nevirapine; PI, protease inhibitor; TDF, tenofovir.
Mutations according to first-line regimen
Most sequences (88%) showed at least one RAM, 79.3% with one to seven NRTI mutations. Among the 256 sequences from patients using NNRTI, 92% had one to six NNRTI mutations. Mutations at codon K103 were observed in 56.7% of them.
Most patients used either AZT/3TC (67%, n = 214) or TDF/3TC (31%, n = 100) as NRTI backbone. Duration on therapy was longer among AZT than TDF users (median 48 months, IQR 27–81 vs. 11 months, IQR 7–22; p < .0001). The proportion of patients using AZT or TDF with at least one NRTI RAM (79.4% vs. 80%) or NNRTI RAM (78.5% vs. 79%, respectively) was similarly high, but the number of mutations differs. Although the number of TAM1 and TAM2 was higher among AZT users, the total number of NRTI mutations were significantly higher among TDF users (1.78 ± 1.4 vs. 1.39 ± 1.3 for AZT, p = .003), mostly due to discriminatory mutations. The number of NNRTI mutations were also higher among TDF users (2.01 ± 1.4 vs. 1.46 ± 1.0 for AZT users; p = .0003). These differences remained significant even when patients with a long period from HIV diagnosis were excluded, as well as when analysis was restricted to patients on NNRTI or on EFV-based schemes, but not if only cases with higher CD4 (>500 cells/mm3) were considered (data not shown).
M184V/I were the most common mutations, observed in 74.3% of all cases. K65R was observed in 32% of patients exposed to TDF/3TC. Table 2 describes NRTI RAMs according to first-line treatment. The proportions of samples with K65R were higher among subtype C (46%) and F (75%) than in subtype B (30%) or recombinant (20%) genomes, but the differences were not significant (p = .5).
PI used included LPV (lopinavir) or ATV (atazanavir), with ritonavir boost. Mutation Q151M and codon 69 deletion were not observed.
Other regimens: EFV/AZT/DDI; AZT/DDI; EFV/ABC/3TC; LPV/ABC/3TC; ATVr/ABC/3TC.
Considering the 63 patients failing PI-based regimens, one to five major PI mutations were observed in 25%. In this subgroup, a NRTI mutation was detected in 60% of the cases; this proportion was significantly higher when PI mutations were present (94% vs. 49%, p = .004). Among these patients, 9% had nonpolymorphic (98AG, 101E, K103N, 190A, or 225HP) and 10% polymorphic NNRTI mutations (V90I, 106I, or 138A).
Mutations and CD4 T cell counts
Patients with virus harboring at least one mutation at genotyping tended to have lower CD4 T cell counts than those without RAMs (277 cells/mm3 vs. 336 cells/mm3, p = .046). A similar difference was observed for the presence of NNRTI mutations (271 vs. 335, p = .03). A CD4 T cell count lower than 200 cells/mm3 was strongly associated with a higher number of NRTI (mean 2.07 vs. 1.39, p < .0001) and NNRTI RAMs (2 vs. 1.6, p = .008). However, if M184V/I was the only NRTI mutation detected, CD4 T cell values were significantly higher in comparison with cases with M184V/I plus additional NRTI mutations (348, IQR 222–582 vs. 82, IQR 55–246 cells/mm3, p < .0001).
Overall, patients failing TDF tended to have a lower CD4 count at genotype test than those failing AZT (206 cells/mm3 vs. 327 cells/mm3, p < .001), but the CD4 T cell counts from cases failing TDF with or without K65R were comparable (182 cells/mm3 vs. 211 cells/mm3, p = .45).
Second-line therapy characteristics
A second-line therapy was documented for 259 patients (81%). The regimen was initiated before the availability of the genotype test results in 9% of these cases. The median time from genotype collection to initiation of the second-line regimen was 2.2 (IQR 1.4–4.2) months.
The NRTI backbone combination most frequently selected was TDF/3TC (75% of patients), with AZT/3TC used by 16% of the patients. Regimens with three NRTI (6%), single NRTI (1%), and no NRTI (2%) were also used.
Most regimens (93.8%) included a boosted PI (46.7% ATV/r, 40.5% LPV/r, 4.6% darunavir/r, and 1.9% fosamprenavir/r). Nonanalogous nucleosides were used by 18 (8.5%) patients (etravirine in four cases), and the integrase inhibitor raltegravir was used by 31 (12%) patients.
Considering all 19 drugs evaluated at HIV db, the median global GSS was 13.5 (IQR 11–16), while the median GSS for the NRTI class was 4.25 (IQR 2.25–4.25). Full activity to all drugs was detected in 19 sequences (7.3% of patients). The median regimen GSS predicted for the 259 second-line antiretroviral combinations was 2 (IQR 2–2.5, range 1–4), whereas the median regimen GSS for the NRTI backbone was 1 (IQR 1–1, range 0–3).
Predictors of viremia control after week 24
Of the 259 patients with a documented second-line prescription, 205 patients (79%) had an available viral load measurement after 24 weeks after initiating the regimen. The median time for the first measurement after this period was 34 weeks (IQR 27–39). Most patients (76.6%) had a viral load less than 200 copies/ml at this measurement. In four cases, viral suppression was documented before completing 24 weeks of second-line therapy, but confirmed at a later collection. For the 149 patients with available CD4 T cell counts after week 24, the median gain was 80 cells/mm3 (IQR 11–195). After week 24, viremic cases had a net loss of 9 cells/mm3 (IQR −49 to −64), whereas those suppressed, a net gain of 111 cells/mm3 (IQR 10–217). There was a strong correlation between CD4 T cell counts at genotype sampling and after 24 weeks of second-line therapy (Spearman's rho = 0.75, p < .0001).
Compared to patients with a CD4 T cell count above 200 cells/mm3, those with CD4 T cell counts below 200 cells/mm3 at genotyping were less likely to achieve viral suppression at week 24 (64% vs. 83%, p = .004).
Most patients with viral load less than 1,000 copies/ml at genotype sampling were virally suppressed at week 24, but there was no significant difference between them and those with viral load above 1,000 copies/ml at sampling (89% vs. 75%, respectively, p = .14). Likewise, higher viral load at collection was not associated to lack of response to the second-line regimen. There was no noticeable association between viral subtype or other variables with viral suppression after week 24 (Table 3).
Logistic regression of variables at the genotyping collection associated to virological suppression after week 24. AZT use in first-line NRTI compared to TDF. Adjusted analysis using any NRTI mutation, instead of only M184I/V, also shows significant independent association, along with low CD4T cell count, to viral suppression.
Mutations according to IAS list.
GSS, genotypic susceptibility score.
The predicted GSS for the second-line regimen did not correlate with virological success. On the contrary, greater predicted regimen activity was associated with worse viral load suppression. Indeed, while failures were documented in 38% of the 47 patients using three or more active drugs, it was observed in only 19% of the 158 patients with less than three active drugs (p = .01). Of the 35 cases with a regimen GSS >2, 71.4% achieved suppression, with 91% of the 11 cases suppressing with a regimen GSS = 1.
The presence of at least one NRTI RAM, detected in 69% of the viremic and in 89% of the viral suppressed patients, was associated to virological success (p = .001). The total number of NRTI mutations among cases with virological success (mean 1.75 ± 1.39) was higher than in those with failure (1.17 ± 1.14, p = .0063). As nonadherent patients could be overrepresented in the group with no mutations, we restricted the analysis to those cases with at least one NNRTI or PI mutation, and the association between the presence of NRTI mutations and virological success at 24 weeks persisted. On the same line, the significant difference remained after excluding from the analysis cases with a GSS = 1 to all antiretroviral drugs (78% of suppression for cases with no NRTI RAMs vs. 95% for cases with NRTI RAMs, p = .002).
When each NRTI RAM was evaluated individually, the M184V/I, present in 82.4% of virally suppressed cases and in 54% of viremic cases, showed a strong association with virological success (p = .0002). Except for mutations at codons K65 and K70, which were somewhat more prevalent in failure cases, most NRTI RAMs were more prevalent in the group of virological success. Figure 1 depicts NRTI RAMs according to virological outcome.
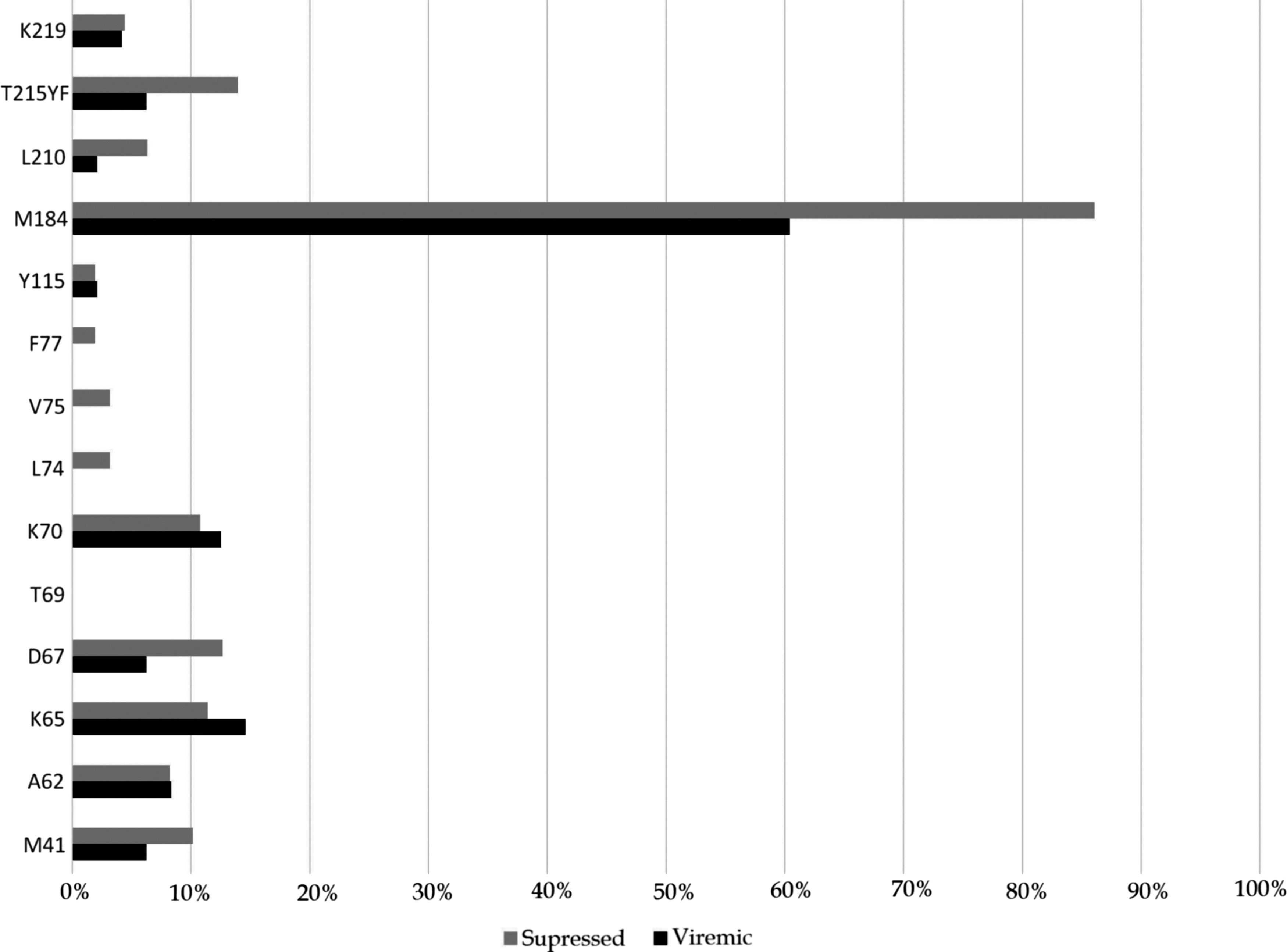
Proportion of mutations (IAS list) to nucleos(t)ide analog reverse-transcriptase inhibitors detected at genotype test performed during first-line failure according to virological outcome to second-line treatment, considering suppression a plasma HIV RNA determination <200 copies/ml at the first test after 24 weeks of second-line therapy.
Suppression was not related to the presence of either NNRTI (77% with vs. 74% without mutations, p = .9) or PI RAMs (89% with vs. 76% without PI mutation, p = .69).
Logistic regression analysis of the associations between variables and virological success is shown in Table 3. CD4 cell counts above 200 cells/mm3 (OR 2.8, 1.5–5.5, p = .002) and the presence of NRTI RAM were independently associated to virological success (OR 4.2, 1.9–9.1, p = .001). However, when only cases with an NRTI mutation other than M184V/I were considered, this association was not significant (OR 1.38, 0.7–2.7, p = .35). In contrast, the detection of M184V/I at first-line failure, independent of the presence of other RAMs, showed a strong association with virological success after the switch to a second-line regimen (OR 4.1, 1.9–8.4, p < .001). CD4 T cell counts above 200 cells/mm3 remained independently associated to viral suppression either if any NRTI RAM or only M184V/I was used in the regression.
Discussion
Resistance to antiretroviral drugs may cause treatment failure or emerge due to lack of viral suppression. In any case resistance profile may impact subsequent therapy. Our aim was to describe RAMs in patients failing first-line therapy, CD4 T cell counts and viral load at the time of genotype test, and, most importantly, its impact on short term (week 24), second-line therapy response. We evaluated in this study HIV sequences from 319 individuals failing first-line therapy. Overall, presence of RAMs at RT, both to NRTI and NNRTI drug classes, was common, with at least one IAS list mutation in 88% cases. These high rates have been observed in studies in Africa and other resource limited settings 19 –21 and could reflect accumulation of mutations during failure. However, in a EuroSIDA study, 22 a high proportion of TAM1 was observed in Europe at 1 year of failure, with a lower than anticipated rate of accumulation among those maintaining the failing regimen. This might suggest that patients acquire most resistance in the first months of failure, with a slow accumulation thereafter.
We were able to compare two commonly used nucleos(t)ide combinations, AZT/3TC and TDF/T3C. Patients using TDF/3TC tended to have more RAMs, but different factors might have confounded our findings. We made subgroup analyses as evaluating only cases with similar time on treatment, cases with treatment initiation at more recent years, and excluding those using PI (as more AZT users had a PI as a second class), but the number of RT RAMs remained consistently higher among TDF users. These differences lose significance at higher CD4 cell counts. Differences in adherence to the regimens could influence, but at least one surrogate for adherence, the proportion of cases with any mutation, was similarly high (79% vs. 80% for NRTI RAM) for both combinations.
The prevalence of TDF resistance observed in our study (32%) was higher than that observed at the TenoRes study for patients in high-income settings (present in 25% of virological failures), but was in the range of that observed in sub-Saharan Africa (28%–50%). 19 The literature is not conclusive whether virological failure on TDF or AZT containing regimens leads to more resistance mutations. A Systematic Cochrane review in 2010 found more resistance in TDF users, but the conclusions were based in limited information, and the authors warn for the fact that the studies reviewed evaluated different drug combinations. 23 Some articles point to more mutations among AZT users, 24 while others document a higher prevalence among TDF users. 25 This latter study was done in South Africa where subtype C predominates, whereas our study population was mostly subtype B infected. The small sample size of non-B subtypes in our study hinders a proper evaluation. However, our data tended to be consistent with clinical and in vitro data suggesting that subtype C viruses are more susceptible to developing the K65R. 26,27
We found a relatively high proportion of NNRTI in patients failing PI at first line. However, many mutations are polymorphisms that were already detected among naive cases in the regions, 16 and nonpolymorphic residues, as at codon K103, show similar prevalence to that observed in different transmitted resistance studies in the area. 16,28 Although we tried to exclude all cases with undocumented antiretroviral exposure, we cannot totally rule out this possibility.
Another objective of our study was to evaluate the response to a second-line therapy. To access the short-term (week 24) response to second-line therapy, we used public laboratory electronic database to search for viral load results. Cases using public antiretroviral dispensary but followed at private laboratories are not to be part of these databases, so the actual denominator to calculate the response to second line could not be determined. Considering this limitation, we observe that most patients (76.7%) in the study were able to suppress viremia after 24 weeks on second-line regimen. NRTI drug recycling was common, with many patients switching one of the NRTI, but keeping 3TC. The extend of NRTI recycling did not show any impediment to suppression to a second line, nor the NRTI combination used at first line, and comparable rates of viral suppression after week 24 were documented in cases failing a regimen with AZT/3TC (76.4%) or TDF/3TC (78.1%). Rates of suppression were also similar across second-line regimens (data not shown), but the study did not have power to discriminate individual regimen success rate.
The predicted second-line regimen GSS did not correlate to virological success and it was actually higher in nonsuppressing cases, but 96% of the cases started second line with a fully active PI or integrase inhibitor. Even when we exclude cases where the genotype test did not detect any mutation (potentially cases with inadequate adherence), still the GSS tended to be comparable, or even higher, among nonsuppressing cases. This finding is similar to the study of Jiamsakul, with a median GSS for the second-line regimen of 2 and no significant association with virological outcome. 29 This study also documented a relation of low CD4 T cell counts to the presence of RAMs.
Multivariable logistic regression shows that both low CD4 T cell counts and the presence of NRTI RAMs were independently associated to virological success after week 24. However, when we evaluated individual mutations, the presence of M184V/I was necessary to observe this association and cases with only other NRTI mutations did not show the association of NRTI RAM to suppression. However, the number of cases with only NRTI RAMs other than M184V/I was small, so the study cannot evaluate properly the role of other individual RAM.
Mutations at codon M184 (valine or isoleucine) confer high cytosine analog resistance, reducing susceptibility to these drugs >100-fold and low-level resistance to abacavir. However, it increases susceptibility and slows the emergence of AZT and TDF resistance, 29 –31 a fact that may favor these drugs in second-line therapy. M184V/I is associated with reduced viral replication in vitro and in vivo. 32,33 In the TenoRes study the prevalence of M184V/I was highest in sub-Saharan Africa and Latin America and lowest in western Europe. 19 It is important to note that all our cases used generic 3TC, and results might differ for emtricitabine, but recent meta-analyses suggest comparable clinical outcome with either drug. 34 Due to its negative impact in viral fitness, M184 RAM may reverse in the absence of therapy more often than other mutations. Therefore its presence could be only a good marker of adherence. However, one cannot rule out both its effect in TDF and AZT activity, as well as its direct impact in viral fitness. The significantly higher CD4 T cell counts among cases with only M184 RAM, compared to cases with only another NRTI RAMs, may support this assumption. Recent data on the evolution of dolutegravir resistance suggest that it may be limited by the effect of M184 mutations on viral fitness. 35 If RAM at codon M184 is proven to be associated to salvage therapy success, for any reason, it may be part of simpler RAM detection point of care devices, which could identify key mutations at positions such as M184 and K65, subsidizing salvage regimens.
The retrospective nature of the study, different exposure time to the first-line regimens, longer among AZT users, and lack of adherence information are clear limitations to the study. We could however evaluate this issue in a rather homogeneous population, with similar access to antiretroviral drugs and monitoring resources. Our findings are in line with large trials 12 –14 that show that NRTI resistance or class recycling is not an impediment to virological success of second-line therapy. However, long-term monitoring is needed to guarantee sustained success of ART in limited resource settings.
Conclusions
Patients failing first-line regimen in public services in São Paulo have high rates of mutations to first-line therapy, but the use of second-line PI based regimens with partially active or inactive NRTI was able to suppress most patients. A high CD4 T cell count at genotype and the presence of NRTI RAMs, especially M184V/I, were independently associated to virological success. Evaluation of long-term suppression is necessary to further support the usefulness of partially active analogs in second and subsequent therapeutic regimens.
Footnotes
Acknowledgments
The authors are grateful to study participants, clinical staff, and other caregivers from the public services involved in the study and to State and Federal AIDS program personnel responsible for the laboratory and drug dispensary data systems. Partially supported by grant no. 2013/194417 São Paulo Research Foundation. Salvage Therapy Working Group: Joao Leandro de Paula Ferreira, Norberto Camilo Campos, Cilene Proenca, and Laís Prado from the Centro de Virologia, Instituto Adolfo Lutz, São Paulo, Brazil; Denise Lotufo and Simone Queiroz from the Centro de Referência e Treinamento em AIDS, São Paulo, Brazil; Luiz Carlos Pereira Junior and Margareth Eira from the Instituto de Infectologia Emílio Ribas, São Paulo, Brazil; Mariana Carvalho e Silva de Carvalho from the Departamento de Clínica Médica, Faculdade de Ciências Médicas da UNICAMP, Campinas, Brazil; Valeria Almeida from the Centro de Referência de AIDS, Campinas, Brazil; and Rafaella S. Gomes and Flavia Gennari Pinheiro from the Ambulatório de Doenças Infecciosas, Jundiaí, Brazil.
Sequence Data
GenBank accession numbers: KY639846–KY640165.
Author Disclosure Statement
No competing financial interests exist.