
Abstract
Beijing has seen a rising epidemic of HIV among students. However, little information was known about the molecular epidemiologic data among HIV-infected students. In this study, the diversity and the prevalence of transmitted drug resistance (TDR) in pol sequences derived from 237 HIV-infected students were analyzed. TDR mutations were found in five men who have sex with men (MSM) population among students. The overall prevalence of TDR in students was 2.1%, comprising 1.3% of protease inhibitors and 0.8% of non-nucleoside reverse transcriptase inhibitors. Our finding indicates a low-level prevalence of TDR mutations among students in Beijing.
B
The epidemic of HIV-1 in Beijing has been on a rapid growth stage since 1998. 4 But according to the data shown by the Beijing Municipal Commission of Health and Family Planning and the Beijing Center for Disease Control and Prevention (Beijing CDC), the growth rate of the HIV epidemic in Beijing has slowed down since 2013. Overall seroprevalence in the Beijing population was ∼0.07% in 2016, which revealed a low-level prevalence of the HIV epidemic in Beijing. However, the data on the Beijing MSM (men who have sex with men) sentinel surveillance system have shown a high-level prevalence in recent years. 3 The HIV prevalence in the Beijing MSM population was 7% in 2015. 5
Sexual transmission is the primary mode of transmission, and the cases attributed to sexual transmission continue to increase in China. 6 According to the recent report on the HIV epidemic in Beijing, the proportion of people infected through sexual contact is still on the rise, increasing from 87.1% in 2011 to 96.9% by the end of October 2016. The trend was particularly apparent for it in MSM, which increased from 61.7% in 2011 to 73.9% by the end of October 2016. 3
The growth rate of the HIV epidemic in 15- to 24 year-old young people is higher than that of the whole population in Beijing. 3 The WHO report “Health for the world's adolescents” addressed that HIV has been confirmed as the second cause of deaths in adolescents globally. 7 The young students are better educated, sexually liberated, and active at their age. The ever-increasing homosexual behavior among students is more likely to encourage the spread of HIV. A study about the HIV epidemic at schools of China reported that the HIV surveillance system has seen a growing number of HIV-infected young students each year. 8 By the end of 2014, the number of surviving HIV-infected young students exceeded 7,200 cases, accounting for 1.4% of all those who survived in China. In 2014, the newly diagnosed HIV-infected students, among whom 98% were boys, exceeded 100 cases in 13 provinces that were distributed across the whole of China. Most of them got infected through sexual contacts, among whom 81% were infected through MSM and 17% through heterosexual transmission. These data have shown that the HIV epidemic among students has been rising in recent years.
Antiretroviral therapy (ART) has dramatically extended the lifespan of patients infected with HIV. A policy called “National Free Antiretroviral Treatment Program, NFATP” has been implemented in Beijing since 2005. The new guideline in Beijing for ART has been changed to recommend all HIV-diagnosed individuals to receive ART since 2013. By the end of June 2016, a total of 12,637 patients had received free ART in Beijing, of whom 11,379 are still alive (unpublished data).
HIV-1 replication is error prone, resulting in the diversity of HIV genome in vivo in which resistance may emerge. 9 Antiretroviral drug resistance mutations, whether derived within a patient or transmitted to newly infected individuals (transmitted drug resistance [TDR]), can have a potentially significant impact on future HIV mortality and may lead to treatment failure for infected people who received ART. 10 TDR is of particular concern because it indicates that individuals failing therapy are transmitting the virus to new individuals. However, there is no information about TDR and other molecular epidemiological data about the HIV epidemic among students in Beijing.
The objective of our study was to determine the prevalence of TDR among treatment-naive students whose occupation was reported as a student in the Chinese national AIDS prevention and control information system. Participants accepted free ART in Youan Hospital or Ditan Hospital, Capital Medical University (CMU), as soon as vein blood samples were collected. Ethical approval was obtained from the local ethics committee at the Beijing Center for Disease Control and Prevention. Participants' demographic data were obtained by face-to-face interviews and by using a standard questionnaire. Blood samples with K2 EDTA were separated by centrifugation immediately, aliquoted, and stored at −80°C.
HIV-1 RNA was isolated from a 200 μl plasma sample by using the MagNA Pure 2.0 system in combination with MagNA 2.0 instruments (Roche Diagnostics, United Kingdom). The partial HIV-1 pol gene fragment (protease 1–99 amino acids and part of reverse transcriptase 1–300 amino acids) was amplified through One-Step reverse transcription polymerase chain reaction (PCR) kits (TaKaRa, Dalian, China) with outer primer pair MAW 26 (5′- TTGGAAATGTGGAAAGGAAGGAC-3′, 2028–2050 nt, HXB2) and RT21 (5′- CTGTATTTCTGCTATTAAGTCTTTTGATGGG-3′, 3509–3539 nt, HXB2) in a 25 μl reaction volume, and the volume of template RNA was 7.5 μl. The amplifications were carried out in a thermal cycler (C1000; Bio-Rad), and the cycling conditions were as follows: reverse transcript PCR (RT-PCR) (50°C for 30 min and 94°C for 2 min), followed by 35 cycles (94°C for 30 s, 55°C for 30 s, 72°C for 2 min), and a final extension for 10 min at 72°C.
Nested PCR was implemented through Takara Ex Taq PCR kit with inner primer pair PRO-1 (5′-CAGAGCCAACAGCCCCACCA-3′, 2147–2166 nt, HXB2) and RT20 (5′- CTGCCAGTTCTAGCTCTGCTTC-3′, 3441–3462 nt, HXB2) in a 50 μl reaction volume, and the volume of the template was 5 μl. The amplifications were carried out in a thermal cycler (C1000; Bio-Rad) and the cycling conditions were 94°C for 5 min, followed by 35 cycles (94°C for 30 s, 55°C for 30 s, 72°C for 2 min), and a final extension for 10 min at 72°C.
The final PCR products were directly sequenced with the pyrosequencing method by Sinogenomax Genomics Company (China). Sequences obtained were assembled and edited by Sequencher DNA sequence analysis software (Gene Codes Corporation, USA), and they were aligned by using the BioEdit program. TDR mutations to protease inhibitors (PIs) and nucleoside reverse transcriptase inhibitor (NRTIs)/nonnucleoside reverse transcriptase inhibitors (NNRTIs) were determined by submitting sequences to the Calibrated Population Resistance (CPR) tool, which is available on the Stanford University HIV Drug Resistance Database (
Demographic data of 237 students are listed in Table 1. They were all male, and the mean age was 23 years (range 16–34). Most of them (76.8%, 182/237) were diagnosed in the recent 3 years (2014–2016). All of them were infected through sexual contact (100%, 237/237), among whom 88.2% (209/237) were MSM and 11.8% (28/237) were infected through heterosexual contact. They were diagnosed and had received free ART in Beijing. Although they lived and studied in Beijing, the data had shown that their census register was distributed among 27 provinces in China, 33.8% of their census register was in Beijing, 9.3% in Hebei province, 5.1% in Shandong province, and 4.2% in Jilin province. As we can see, 50% of cases came from the four northern provinces just mentioned. Beijing, as a pilot city for HIV early treatment, has been pushing the measure since 2013. The Beijing Municipal Commission of Health and Family Planning has made a great effort in establishing the “green channel” to ensure that the patients who are newly diagnosed can benefit from ART more conveniently and timely. It was reported that the minimal time interval between diagnosis and the receiving of free ART is reduced from 100 days in 2011 to 7 days in 2016. 14 All participants in this study had received free ART from 2014 to 2016; the median time interval for them was 22 days in 2016 compared with 41 days in 2015 and 101 days in 2014.
TDR, transmitted drug resistance; URFs, unique recombinant forms.
Through an analysis of “COMET HIV-1” and the Neighbor-Joining phylogenetic tree built by MEGA(v7.0.21) (Fig. 1), subtypes of 237 HIV-1 pol sequences were confirmed. CRF01_AE was the most dominant subtype, accounting for 49.8% (118/237), followed by CRF07_BC (32.5%, 77/237), Subtype B (11.4%, 27/237), URFs (3.4%, 8/237), CRF68_01B (1.3%, 3/237), CRF55_01B (0.8%, 2/237), CRF65_cpx (0.4%, 1/237), and Subtype A1 (0.4%, 1/237) (Table 1). Then, we identified the recombination forms of URFs by using the tool of jpHMM. Among eight URFs, four of them were classified as new recombination forms of CRF01_AE and Subtype B; two of them were a recombination of CRF01_AE and Subtype C; one of them was a recombination of CRF01_AE, Subtype B, and Subtype C; and the remaining one was a new recombination form of Subtype B and Subtype C.
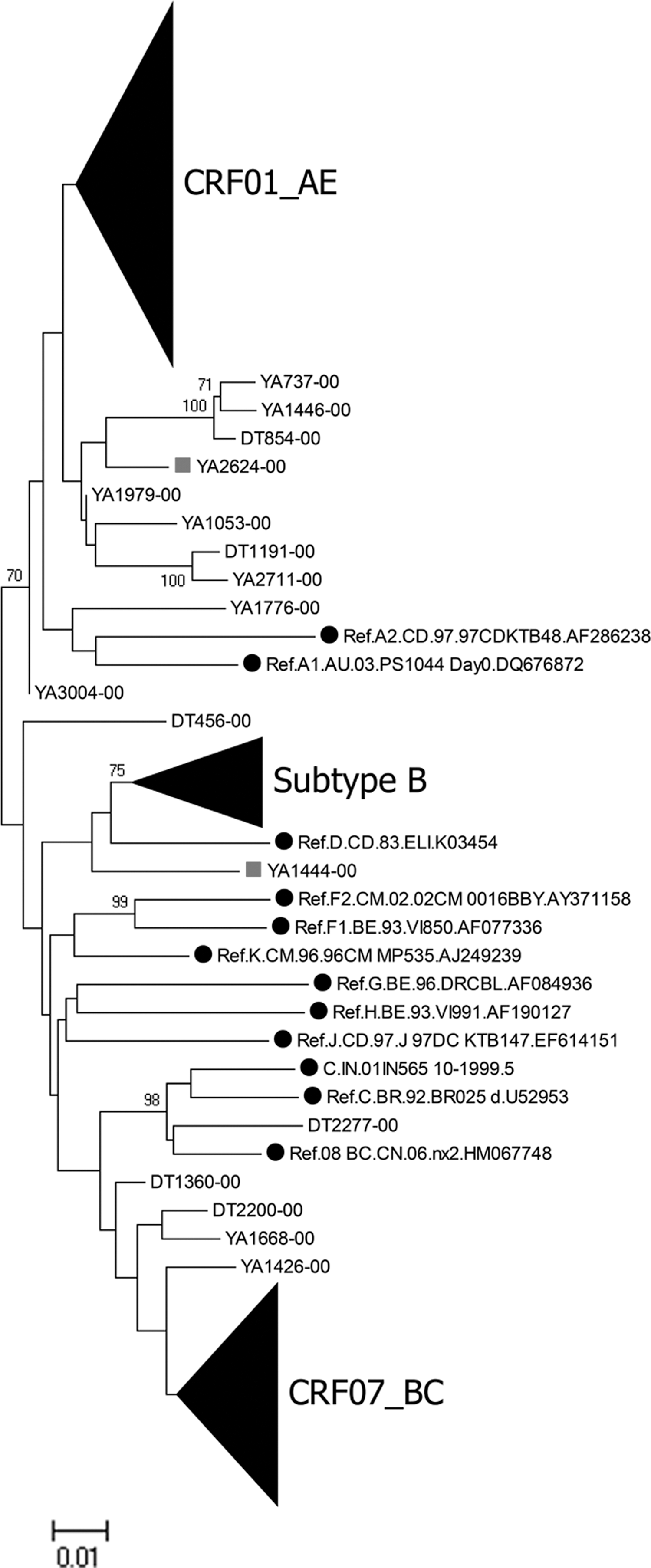
The neighbor-joining phylogenetic tree was built by using 237 HIV-1 pol sequences from treatment-naive HIV-1-infected students in Beijing. The reference gene sequences of subtypes A–D, F–H, J, K, CRF01_AE, CRF07_BC, CRF08_BC, and group O were downloaded from the HIV database. The scale length indicated 1% nucleotide sequence divergence. Black dot denoted reference sequences, triangle denoted the sequences containing TDR, square denoted the patients infected through heterosexual contact, and the TDR mutations were illustrated in the tree. TDR, transmitted drug resistance.
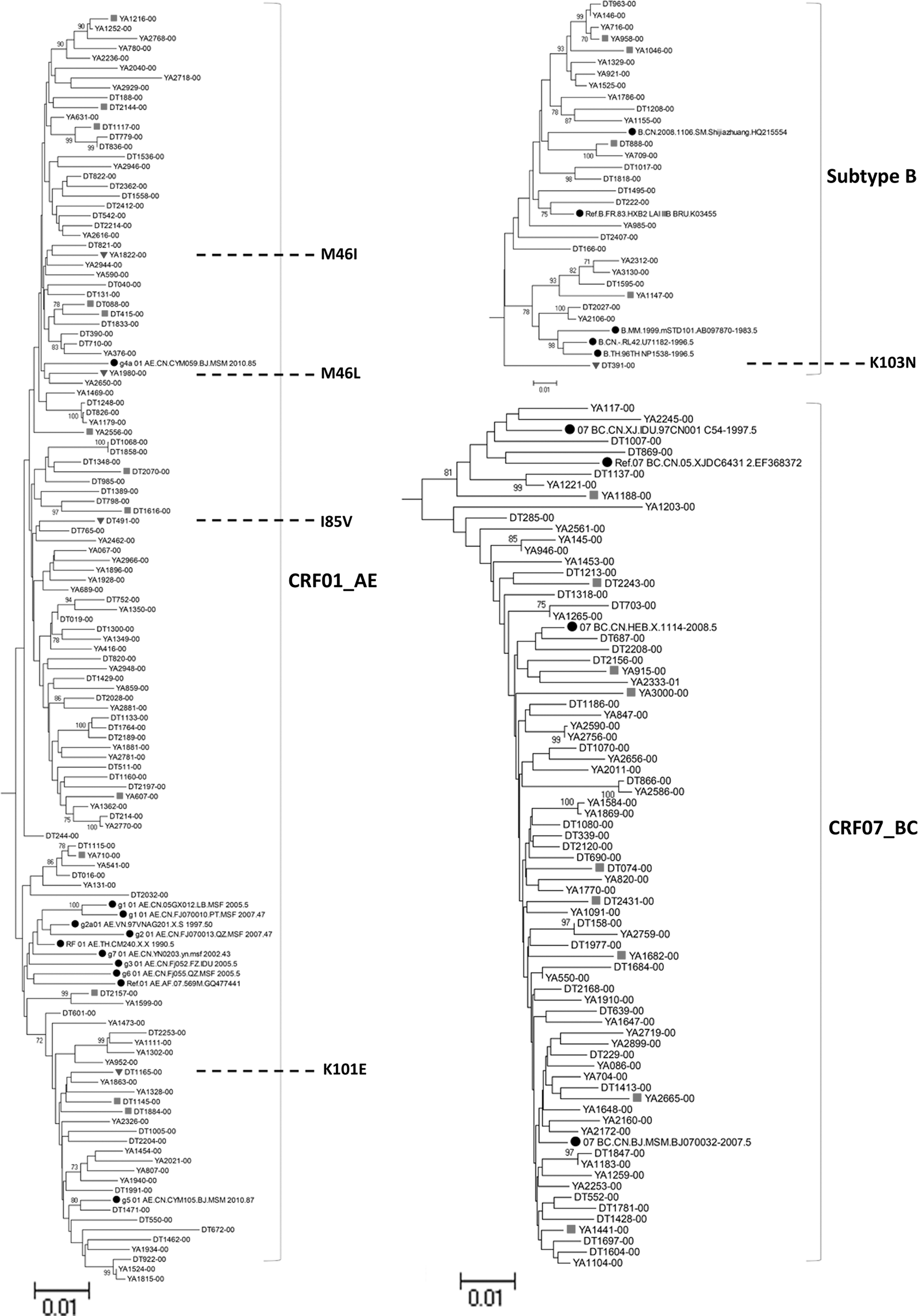
TDR mutations analysis of the 237 pol sequences showed that drug resistance mutations were identified in five samples, leading to an overall prevalence of TDR of 2.1% (5/237). TDR to PIs were detected in 1.3% (3/237) of the patients. Mutations were I85 (0.4%, 1/237), M46I (0.4%, 1/237), and M46L (0.4%, 1/237), respectively. TDR mutations to NNRTIs were detected in 0.8% (2/237) of the students. K103N (0.4%, 1/237) and K101E (0.4%, 1/237) were harbored by two patients, respectively. TDR mutations to NRTIs were not detected. No sample with dual or triple TDR mutations was found in the study. Depending on the WHO threshold survey guidelines, the rate (2.1%, 5/237) indicated a low-level prevalence of TDR among students in Beijing.
All the five students harboring TDR mutations were male and got infected through MSM (Table 2). We found an unequal distribution of mutations in the census register and subtype. The rates of TDR associated with the census register were 1.25%, 10%, 14.5%, 14.3%, and 33.3% for Beijing, Jilin, Inner Mongolia, Heilongjiang, and Tianjin, respectively. The rate of TDR among Subtype B was the highest (3.7%, 1/27), followed by CRF01_AE (3.4%, 4/118). No mutations of TDR were detected in CRF07_BC and other subtypes.
MSM, men who have sex with men; NNRTIs, nonnucleoside reverse transcriptase inhibitors; PIs, protease inhibitors.
Previous studies have found that the prevalence of TDR was 6.7% in China. 15 Studies in Beijing have shown that the prevalence of TDR in treatment-naive patients was 6.7% from 2006 to 2007 and 5.3% from 2007 to 2010, indicating a middle-level prevalence in Beijing. 4,16
Our study demonstrated that the rate of TDR was only 2.1% among students, which indicated a low-level prevalence of TDR among students in Beijing. The result also reflected a relatively low prevalence of drug-resistant strains of HIV among students. A survey of MSM students in Beijing reported that when talking about making friends, 44% of MSM students preferred to choose students. The proportion for those who only choose students as sexual partners accounted for 10%. 17 Due to the differences in terms of economic capability, educational level, and individual interest between students and people outside the campus, social network among students is relatively independent and students may communicate relatively less with others outside the school. The limited social network may restrict the spread of TDR among the students.
In our study, four patterns of TDR mutations were detected in CRF01_AE and one pattern was detected in Subtype B. Non-repeated resistance mutations in five students indicated that TDR mutations were independent events that occurred, respectively, rather than were transmitted from one student to another. A more persuasive proof was that five students harboring TDR mutations dispersed from each other rather than converged at one cluster in the N-J tree (Fig. 1, TDR mutations were labeled in the tree). The consequence could further explain the low prevalence of TDR mutations among students.
We found a relatively high prevalence of CRF07_BC in students. This phenomenon was also found among MSM in Beijing in another study. 18 It was reported that the proportion of CRF07_BC among MSM in Beijing was 12.6% from 2007 to 2010, followed by 27.80% from 2011 to 2013. 4,18 In 2016, the province of Hebei, Beijing's neighbor in geography, reported a distribution of 26.3% for CRF07_BC among 16–25 year-old HIV-infected youth in 2016, of whom 78.9% were MSM. 19 The proportion of CRF07_BC had witnessed a rise since 2007 among MSM in Beijing. In our study, the prevalence of CRF07_BC among MSM students was 32.5% (68/209). CRF07_BC was primarily reported among intravenous drug user (IDU) populations in China. A survey conducted in Beijing in 2013–2014 reported that about 26.8% (961/3588) of MSM had ever used a kind of popular and new drug named rush poppers (a kind of nitrite derivative) in the past 3 months, and 53 participants confessed the experience of using heroin voluntarily. Poppers were inhaled, which leads to a low risk of HIV infection, whereas heroin may be either smoked or injected, so heroin could increase the risk of HIV infection. The study also pointed out that there was a correlation between the use of drugs and HIV infection. 20
Data revealed that the rate of receiving ART was 74.6% among all the diagnosed populations in Beijing by the end of 2016, with the rates of 80.0% in MSM and 26.8% in IDU. According to the data only in 2016, the rate of ART among all diagnosed people in 2016 was 64.7%, with 67.0% in MSM. When it came to the IDU population, the ratio fell to 14%. The prevalence of CRF01_AE, which was dominated in MSM, might have been under controlled conditions for the high rate of ART among MSM. However, CRF07_BC, which was primarily found in IDU and was the dominating subtype among IDU in Beijing, 21 might be out of control. On the contrary, IDU only accounted for 5.2% (1134/21886) of all HIV-positive people reported in Beijing (data till the end of October 2016). 3 The virus in their bodies could spread through both intravenous injection and sexual contact. A survey on HIV-related behavior among IDU in Beijing revealed that 31.5% of them shared syringes and needles with other IDU; 31.8% of the IDU had high-risk sexual behaviors for drug dealings. 22 The uncontrolled viral load and high-risk behaviors among IDU were sufficient to have an impact on the entire HIV epidemic in Beijing. These may be the possible reasons for the ever-increasing prevalence of CRF07_BC among MSM and students in Beijing.
Drug use is not allowed in China. Most of IDU are reluctant to apply for antiviral treatment because they are afraid to be punished by the law. In most cases, they are unwilling to provide their own contact information. It is difficult to maintain any regular contact with them for providing HIV treatment and prevention services. Therefore, the low rate of treatment among IDU may be a challenge for us to stop the increasing prevalence of CRF07_BC in Beijing.
Among 237 HIV-infected students, 88.2% of them were MSM. Students who were infected through heterosexual contact had only 28 (11.8%) cases. Previous research about the epidemic of CRF 01_AE revealed that the clusters 1 and 3 mainly spread in heterosexuals and IDU in mostly southern provinces. 23 No clusters gathered with heterosexuals in the CRF01_AE subtree (Fig. 1) were observed in our study. By the analysis of N-J tree of 237 students, most heterosexuals were surrounded by several MSM. The result suggested that some students who were recorded as heterosexuals probably also had sexual contact with MSM.
Beijing has made great efforts to respond to the HIV epidemic. The government is active in exploring different ways in fighting against HIV, such as popularizing oral fluid HIV testing and anonymous urine HIV detection, expanded testing, and early treatment. Publicity and education of HIV is carried out at schools every year, such as providing free condoms, safe sex education, and peer education. 14
Overall seroprevalence in the Beijing population had revealed a low-level prevalence of the HIV epidemic. Although data about MSM in Beijing had shown a high-level prevalence and an increasing proportion (from 61.7% in 2011 to 73.9% by the end of October 2016) in the recent 5 years, we had not seen an obvious increase in either the number or the percentage of HIV-infected MSM in Beijing from 2015 to 2016. It had been kept stable during the recent 2 years, with 74% (2354/3181) cases reported from January to October in 2015 and 73.9% (2317/3135) cases reported in the same period in 2016. 3,5
It is worth noting that Beijing has been pushing the measure of HIV early treatment since 2013. The rate of ART among MSM in 2016 was 80.0%. With the maintenance of a high rate of receiving ART and the implementation of several prevention efforts such as expanded testing and early treatment, we will probably see a decline in the HIV epidemic among MSM in Beijing in the future. However, the number of HIV-infected cases in 15- to 24 year-old young people increased from 624 in 2015 (from January to October) to 647 in 2016 (from January to October). The dynamic changes of the HIV epidemic in Beijing require more attention and more effective measures of preventing AIDS need to be carried out in the future, especially among youth.
Our study is the first investigation of the molecular epidemiology of HIV-1 among HIV-infected students in Beijing. Genotype subtype distribution and the rate of TDR among HIV-infected students in Beijing were illustrated for the first time. These findings will enhance our understanding of the biological features of HIV among students and will be beneficial in issuing guidelines for the treatment of HIV-infected students and the control of the HIV epidemic among schools in Beijing.
Sequence Data
All sequences have been deposited in GenBank under accession numbers KY713346 to KY713582.
Footnotes
Acknowledgments
The authors thank the staff of 16 local districts, the CDC in Beijing, and the students who participated in this study. They are also very appreciative to the doctors and nurses in Youan hospital and Ditan hospital for their admirable treatment and patient care. This study is supported by the Beijing Science and Technology Planning Project of Beijing Science and Technology Commission (D161100000416002).
Authors' Contributions
The study was conceived and designed by Y.W., X.H., C.H., and H.L. M.H. carried out the study and analyzed the experimental data. M.H. wrote the article. J.W. and J.C. contributed to the acquisition and analysis of epidemiological data. X.L., Y.H., R.X., and J.Y. edited and assembled sequences. All the authors have read and approved the final article.
Author Disclosure Statement
No competing financial interests exist.