
Abstract

E
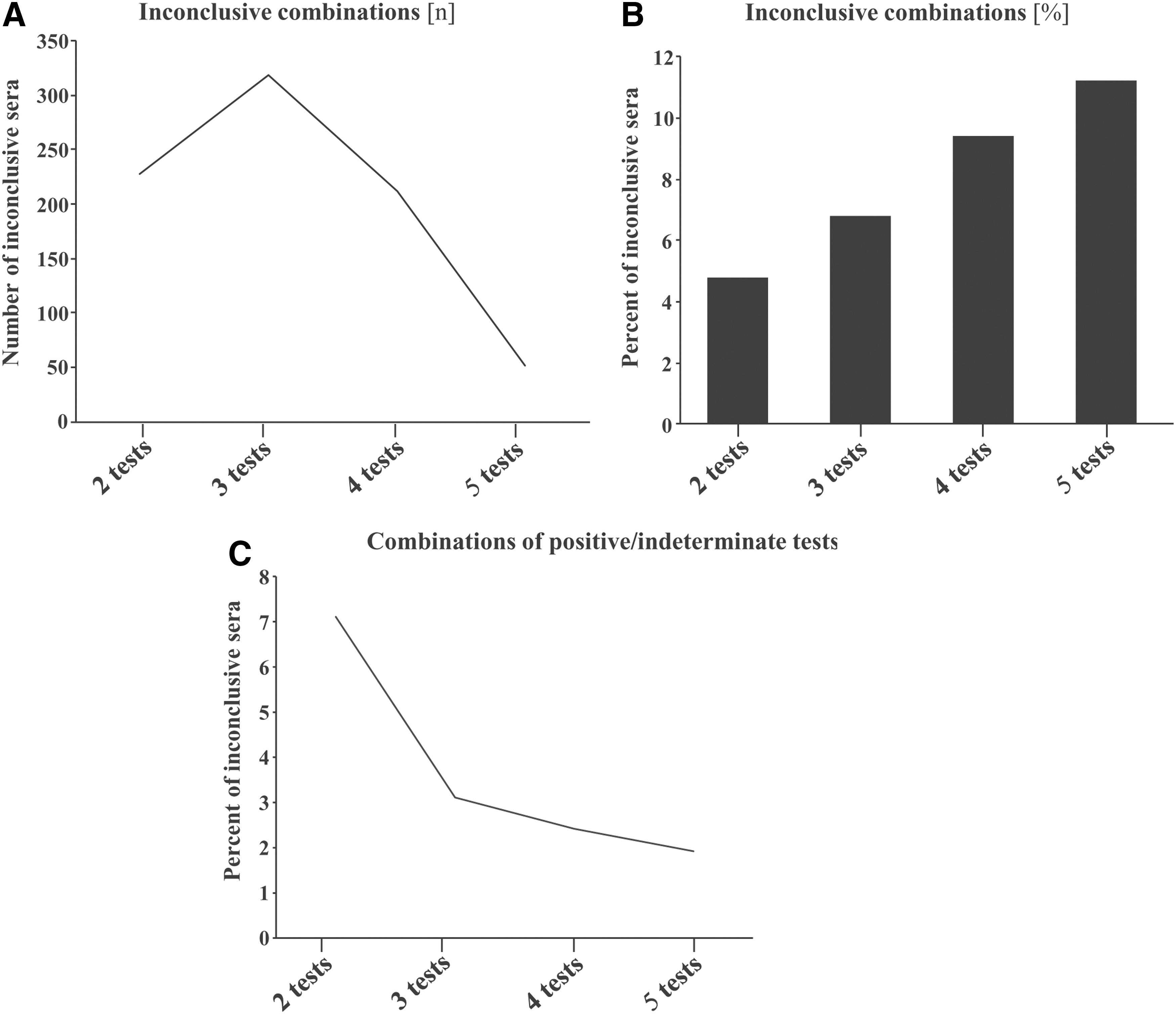
A total of 464 sera from HIV-negative individuals were prospectively collected in Cameroon and were further tested in parallel by two to five HIV serological assays, as previously reported. 2 The number and proportions of sera classified as “inconclusive” (neither positive nor negative), that is, giving discrepant tests results by a given combination of 2, 3, 4, or 5 HIV tests, 2 carried out in parallel, are shown in Figure 1. The total number of “inconclusive” combinations was 227 with the two-test combination, 319 with the three-test combination, 211 with the four-test combination, and 52 with the five-test combination (Fig. 1A). The percentage of individuals with discordant test results increased significantly and proportionally as more tests were used, ranging from an average of 4.8% of individuals when two tests were used, 6.8% of individuals when three tests were used, 9.4% of individuals when four tests were used, and 11.2% of individuals when five tests were combined (p < .001) (Fig. 1B). Finally, the number of “inconclusive” combinations with all tests of the combination being either all positive or inconclusive decreased significantly with the number of tests in the combination: 16 (7.1%) with the two-test combination, 10 (3.1%) with the three-test combination, 5 (2.4) with the four-test combination, and 1 (1.9%) with the five-test combination (Fig. 1C) (p < .04). All blood samples from individuals with inclusive results (whatever the combination) were all negative for HIV-1 LTR PCR in dried blood spot collected on using Whatman 903 filter paper.
Absolute number (n)
We further applied the sequential 2015 consolidated WHO testing algorithm in high prevalence settings (>5%) to the three tests providing the lowest number of inconclusive sera when tested in parallel, 3 including the following HIV serological assays: Alere Determine™ HIV-1/2 [T1], SD Bioline HIV 1/2 3.0 [T2], and Genscreen Plus HIVAg-Ab [T3]. The latter combination provided 10 inconclusive sera, none of which being positive or indeterminate by all three tests. The results are shown in Table 1. The number of inconclusive (I) sera was less important when the tests are used in series (I: 1–9) than in parallel (I = 10). Certain combinations gave rise to higher numbers of inconclusive sera than others. Finally, it was possible to find and validate with field sera serological combination of three tests used sequentially giving rise to very low numbers of inconclusive sera, and harboring 100% sensitivity and very high specificity, such as T2 → T5 → T1 or T5 → T2 → T1 (Table 1).
T1: Alere Determine™ HIV-1/2; T2: SD Bioline HIV 1/2 3.0; T3: Genscreen Plus HIVAg-Ab.
The sensitivity and specificity of a given sequential combination of the three tests T1, T2, and T3 according to the 2015 consolidated WHO testing algorithm in high-prevalence settings (>5% 3 ) were estimated by taking into account for calculation N′, corresponding to the size of the study population (N) deleted of the number of inconclusive sera according to the combination used.
CI, confidence interval; I, number of inclusive sera with a given sequential combination; N, effective of the study population (N = 464); N′: N − I; Youden's J index = sensitivity + specificity – 1.
Inconclusive serological diagnosis of HIV infection is particularly frequent in Central Equatorial Africa, 2 especially for some HIV tests and HIV test combinations. 1 Our observations demonstrate that the frequency of inconclusive sera depends on the nature of the serological tests used in a given combination and that it is also directly proportional to the number of HIV tests used in parallel: the more the serological tests used, the higher the frequency of inconclusive sera. The decline in inconclusive results is the reason behind the WHO recommendation of using a series of tests. The 2015 consolidated WHO alternative strategy suggests using highly sensitive first-line assays, followed by highly specific second- and third-line assays. 3 Our results show that even with three tests used in combination, as proposed in the 2015 WHO recommendations, 3 the risk of false HIV-positive reactions may persist, even with the use of fourth generation combo enzyme-linked immune assay. However, the risk may be very limited by certain combinations of HIV tests. Taken together, these findings confirm that the best tests and test combinations must absolutely be carefully validated on the field with local sera panel corresponding to given environmental and human biotopes.
Footnotes
Acknowledgment
M.-A.J. is the holder of the Canada research chair tier 2 in immunovirology.
Author Disclosure Statement
No competing financial interests exist. C.T.C is a FRQ-S Junior 1 awardee.