
Abstract
The men who have sex with men (MSM) population infected with HIV is poorly studied in Russia because of stigma and discrimination. In the first years of the HIV epidemic, the only HIV genetic variant that circulated among MSM was subtype B, usually acquired abroad. Meanwhile, the massive epidemic of HIV in Russia was caused by a highly homogenic subtype A variant, AFSU (A6), and spread mainly among drug users. In this study, 155 HIV pol sequences from MSM collected during the 2006–2016 period were analyzed. Phylogenetic analysis found that 19.4% of the viral sequences from MSM clustered with HIV genetic variants A6 and BFSU, which were previously identified only among drug users and their heterosexual partners. These data show that the MSM population in Russia is gradually becoming less isolated from the general epidemic process. Urgent measures should be taken to prevent the spread of HIV among the MSM population.
T
The unique HIV-1 variant that caused the HIV explosion in the mid-90s belonged to subtype A and was named AFSU (IDU-A). 1 This virus is quite distinct from other subtype A viruses, and according to recent nomenclature revision, the virus is now called subsubtype A6. 2 The AFSU/A6 variant (subsequently referred to as A6) continues to be the predominant type in Russia, maintaining relative genetic homogeneity, although the infected population now includes HSXs with no increased risk of infection from traditional risk factors. 3 Another HIV variant, BFSU (IDU-B), that originated in Ukraine 4 was typical for drug users and is quite rare in Russia.
The role of men who have sex with men (MSM) in the development of HIV infection epidemic in Russia has not been determined because of the absence of systemic information. 5 According to internal estimates of 2012 to 2013, there were from 0.75 to 1.5 million MSM living in Russia, with 1%–1.3% of them being HIV infected. 6 The UNAIDS report estimates this number to be four times higher, with a rate of 6% HIV infection in this group. 7 Independent experts say the prevalence of the epidemic among MSM is between 5% and 25% of the population, depending on the region. 8 In 2015, the Russian Federal AIDS Center (RFAC) reported 210 new HIV cases among 2,781 MSM patients studied (7.6%). 9 These differences can be explained by the existence of the traditional society stigma and discrimination of MSM in Russia that, in particular, makes it difficult or impossible to obtain reliable HIV statistics. Therefore, the existing data do not allow for assessing the full extent of the HIV epidemic among MSM, which, in turn, hinders treatment and prevention programs. According to the RFAC data (personal communication), to date, only 4% of MSM living in Russia are included in HIV prevention programs.
Meanwhile, studies among the gay community and MSM groups were carried out in the late 1990s in Russia, mainly with the participation of foreign partners. These studies described sex for money, as well as the use of alcohol and drugs as typical features of behavior in the Russian MSM community. 10,11 In addition, the considerable number (up to 70%–80%) of persons who did not identify themselves with the MSM community were bisexuals, with many of them being married. 11
The observations of HIV genetic variants spread in MSM in Russia were not systematic. In the years 1987–1996, before the massive epidemic in IDUs started, MSM constituted the majority of registered HIV cases. In those years, only subtype B (pandemic Western variant) was detected in this group. In the following years (1997–2006), MSM amounted to only a very small portion of the HIV samples subjected to genotyping, with a huge number of infected cases being drug users, but 100% of viruses genotyped in MSM belonged to subtype B. 3
The first reports about HIV-1 non-B subtypes in MSM in Russia were published in the mid-2000s. 12,13 Such observations were made through molecular studies in relatively small groups of patients in St. Petersburg and Krasnoyarsk; the cases were very rare and represented mainly by the strain A6. Since then, the authors of this article have repeatedly gained information about cases of non-B subtypes in MSM, but no data have been published.
In this study, the analysis of HIV genetic variants in MSM was performed using a set of samples collected in our laboratory between 2006 and 2016 in the course of molecular monitoring of the HIV infection epidemic in Russia. Each participant provided informed consent and this study was conducted after approval from local ethical committees.
The collection of 1,388 samples included 147 (10.6%) HIV genotypes from therapy naive individuals referred to MSM contacts as the main route of infection with HIV in St. Petersburg, Moscow region, Krasnodar, Noyabrsk, Krasnoyarsk, Arkhangelsk, and several other Russian cities. HIV-1 sequences from 12 male IDUs and 12 HSXs infected in Noyabrsk were obtained for supplementary analysis. In addition, eight HIV protease and reverse transcriptase (PR-RT) genotypes belonging to Russian MSM were obtained from GenBank. The HIV-1 sequences (pol gene, full PR, and partial RT regions; sequence lengths, 876–1302 nucleotides) were obtained using Viroseq or in-house method. Epidemiological information for the study individuals is presented in Table 1. The alignment and phylogenetic analyses of the sequences were conducted using MEGA6 software.
14
Genotyping was carried out using the online programs COMET HIV-1/2 and HCV v.0.2 (
IDUs, intravenous drug users; MSM, men who have sex with men.
Preliminary data on the HIV-1 subtype distribution were obtained using the COMET and Rega tools, and the same results were obtained using each. According to these results, most of the PR-RT sequences belonged to HIV-1 subtype B (127/155; 82.0%), whereas the HIV-1 subtype A1 was found in 16.1% (25/155) of samples, and the remaining two viruses were interpreted as subtype G and one was interpreted to be a unique B/A recombinant.
For a more advanced analysis, a phylogenetic tree was constructed, which included the reference strains typical for the Russian HIV infection epidemic, namely, A6 and BFSU (Fig. 1).
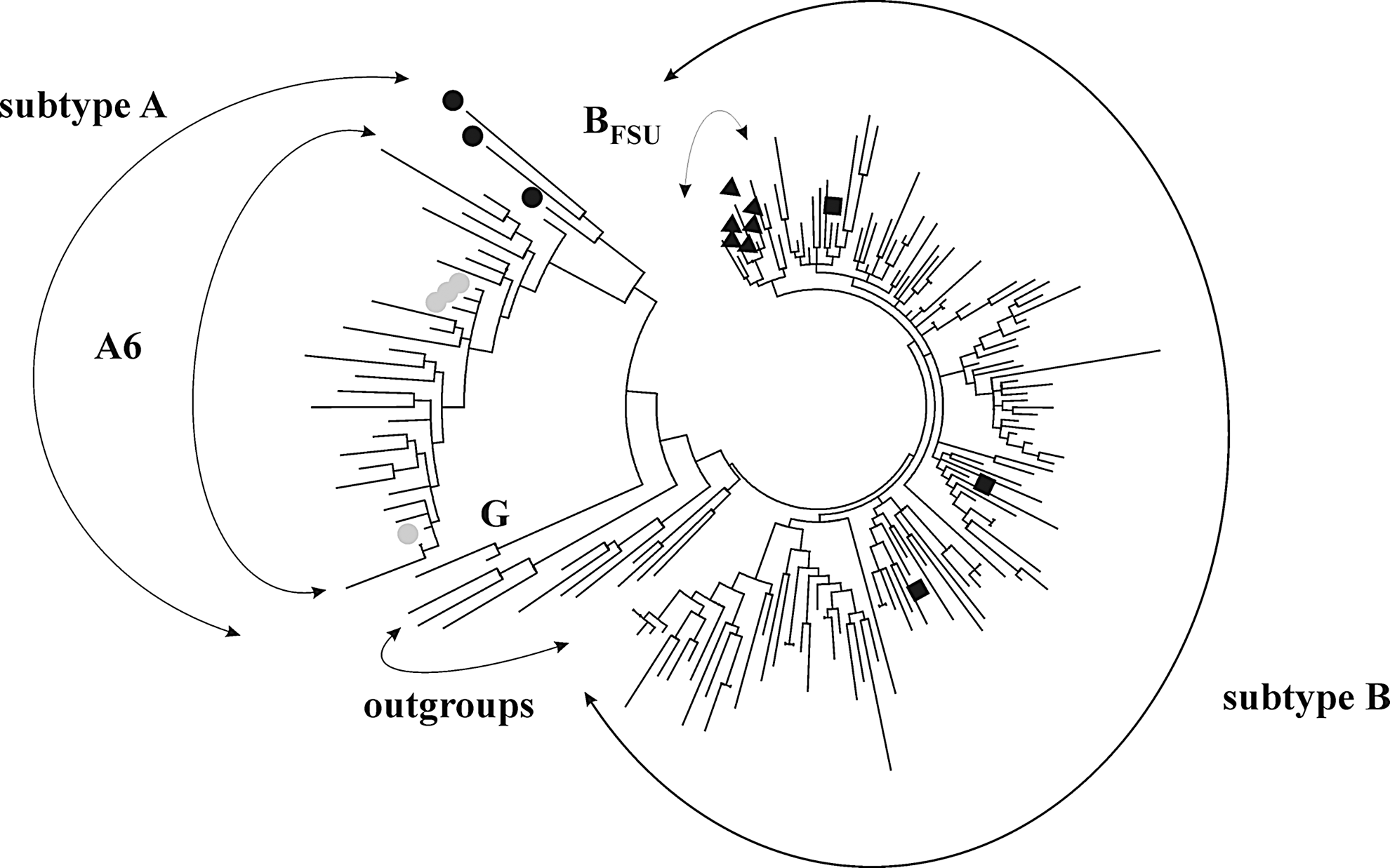
Maximum likelihood phylogenetic tree of HIV-1 pol genomic sequences from the Russian MSM, Tamura-Nei model, nearest-neighbor-interchange heuristic method, 500 bootstrap replications. Subtype A1 references (AF069670, AF484509, and U51190) are marked by black circles; A6 references (AY500393, HQ161930, HQ449397, and EF589043) are marked by gray circles; subtype B references (AY173951, AY423387, and JA806687) are marked by black rectangles; BFSU references (KF971921, KF205383, KC254614, HQ115066, KC701380, and KF971924) are marked by black triangles. Subtype C (AF067155, U46016, and U52953) and F sequences (AF005494, AF075703, FV536593, and AJ249238) were used as outgroups. IDUs, intravenous drug users; MSM, men who have sex with men.
The phylogenetic analysis of the PR-RT sequences (876 nucleotides) revealed that the strains subtyped as A1 formed a large cluster with the A6 variants from Russia, Ukraine, and Kazakhstan, which was expected. The less predictable outcome was the detection of five MSM sequences clustering with BFSU (bootstrap support 61%, not shown on the tree). Most of the sequences belonging to subtype B formed several low supported clusters with no signs of geographical relationships. Two subtype G sequences were distinctly distinguished on the tree and the recombinant B/A was included in one of the B clusters. Hence, among MSM patients, 19.4% of viral sequences clustered with HIV genetic variants A6 and BFSU, which were previously identified only among drug users and their HSX partners. Non-Western B variants (including subtype G and B/A recombinant) accounted for 21.3% of the total number of samples.
The same tendency was found in the group of 37 patients from Noyabrsk (a small city in North Russia), in which almost equal number of randomly chosen drug users, HSXs, and MSM were included (Table 1). According to phylogenetic analysis (Fig. 2), all IDUs and HSX patients were infected with the A6 HIV variant. Among MSM, 10/13 clustered with both the BFSU and “Western B” variants (bootstrap support more than 95%, not shown on the tree), and the remaining three samples belonged to the highly supported (99%) cluster of A6 together with HSXs and IDUs. Among them, 100% support was found between MSM and IDU patients, which attracted our attention (depicted by black arrow).
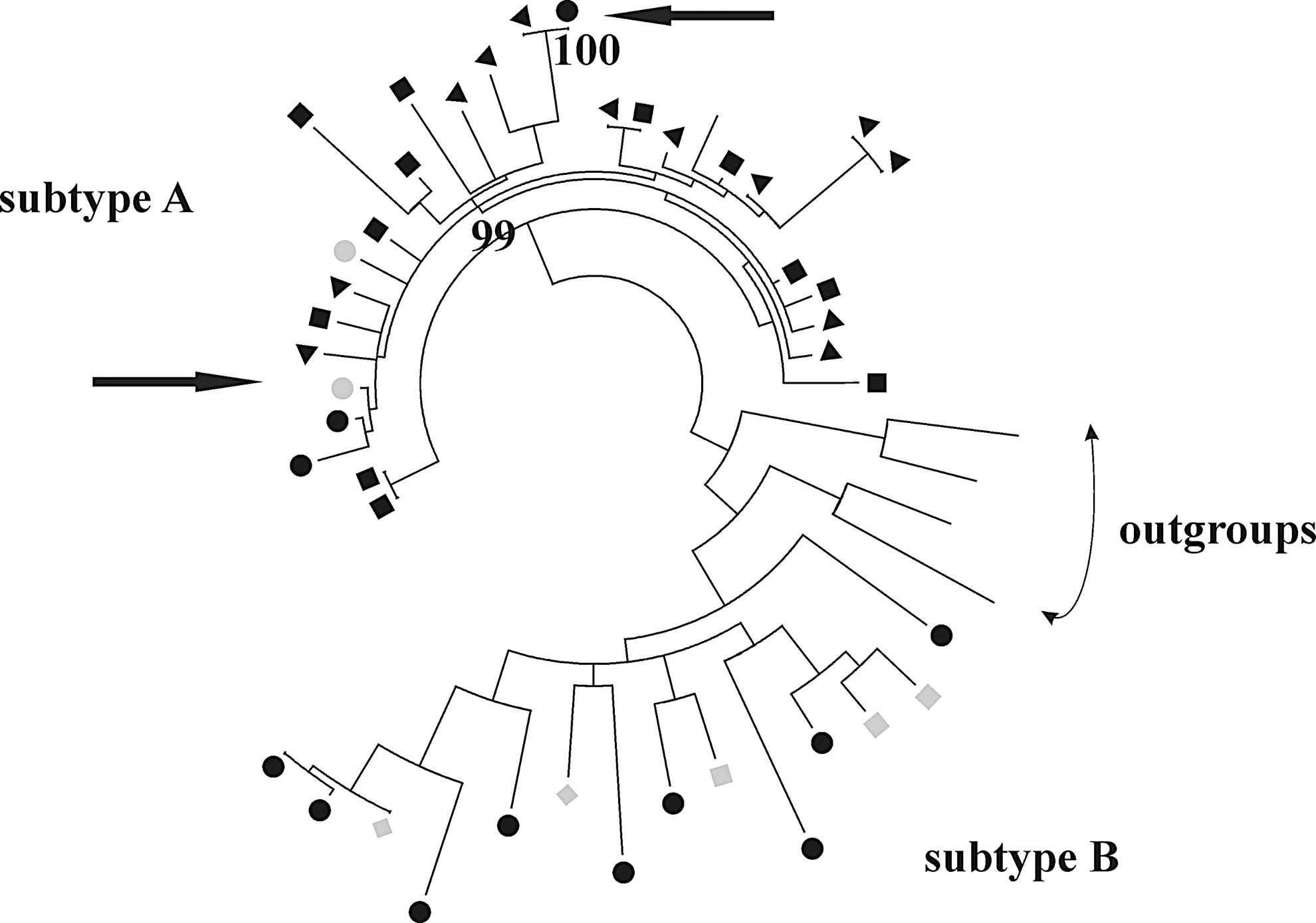
Maximum likelyhood phylogenetic tree of HIV-1 pol sequences from MSM, IDU, and HSX patients from Noyabrsk, Russia, model same as in Figure 1. MSM sequences are marked by black circles, IDU sequences are marked by black triangles, HSX sequences are marked by black rectangles. Reference sequences are marked by gray circles (A6; AY500393, and AF413987), gray rectangles (BFSU; DQ207943, HQ115066, and DQ207942), and gray diamonds (“Western B”; HM586190 and KJ771697). The arrows point to the HIV-1 sequences clusters mentioned in the text. HSXs, heterosexuals.
In summary, the results obtained in this work confirm the hypothesis that the MSM population in Russia is gradually becoming less isolated from the general epidemic process. During the initial studies of HIV infection epidemic in Russia in the early 90s, all cases of MSM infection were associated with travel abroad, mainly to Europe and other countries where HIV subtype B was most prevalent. Thus, such an isolated situation could not last for long in a country where the massive epidemic was caused by non-B viral variants. Indeed, as can be seen, the MSM HIV-infected population in Russia has become heterogeneous with respect to HIV genetic variants.
Today, one-fifth of MSM with HIV are infected with the non-B subtypes, which have traditionally been attributed to the high-risk group of IDUs. This is indirect evidence of the existence of rather intense relationships between MSM and other population groups, possibly through the shared use of drugs and sexual contacts. In addition, the results obtained in this study indicate a drawback of current epidemiological investigations: MSM patients are likely to indicate incorrect route of transmission and so probably have additional possible risk factors for HIV infection. Taken together, these HIV genetic data serve as a strong indication for the need to review the existing prevention strategies for the MSM group, which may be significantly larger in terms of both the number of individuals and the degree of involvement in the HIV epidemic process in Russia.
Sequence Data
The GenBank accession numbers for the sequences described in this article are KU645850, KU933330, KU645855, KU557645, KF692175, KF257883, KP090071, KT121457, HQ449396, KR233369, KX517445–KX517449, KR233386, KX446869–KX446888, KX517381–KX517408, KX517413–KX517444, KX530764–KX530767, KX517450–KX517457, JQ292895, KF692175, AY682547, HM345567, DQ207942, DQ205269, AY819715, AY751407, AY682547, FJ822104, FJ822105, FJ822114, FJ822112, KP090095, KX788813–KX788816, and KY857892–KY857922.
Footnotes
Acknowledgment
The research leading to these results has received partial funding from the Russian science foundation, agreement N 15-15-00050 (2015–2017).
Author Disclosure Statement
No competing financial interests exist.