
Abstract
Despite the difficulties to follow and retain patients for a long time in the public health service, special programs may bring about increased chances of survival and better quality of life, as well as higher rates of retention in care; this is also true for middle-income developing countries such as Brazil. Our relatively small outpatient service (∼500 HIV-infected patients) may not mirror the reality encountered in other settings, including São Paulo city, but retention and high quality of care may improve rates of virological success, even in poorer settings. Furthermore, prevention of depression or anxiety, with discussion in groups of patients with the presence of a therapist, regular HIV RNA viral and CD4 cells counts, genotyping tests pre-HAART, and vigilance for drug failure, may explain this successful experience. We should also take into consideration that our cohort consists mostly of asymptomatic at-entry patients referred by the Blood Bank of São Paulo, located at the same hospital, implying that they had a better immunological status at start than the more usual HIV population. Besides that, the degree of adherence to treatment in our service, in general, is quite high and the patients have a higher mean educational level: >90% of the patients a high school or college education. Such features make this cohort a very specific and differentiated sample. To extend our findings, we intend to conduct similar studies in other HIV treatment centers, enabling comparisons of populations with different profiles.
S
Our group started an open clinic aimed to pick up immune deficient patients as early as 1983. We still follow a patient enrolled in 1989, which is the longest follow-up time of our service. This pioneer outpatient service was established as a branch of the Clinical Immunology Service of Hospital das Clínicas de São Paulo, a university hospital associated with the São Paulo University Medical School. At first, most of the patients were homosexual men, but soon the number of cases increased, and so we created a specific outpatient service to provide care for patients with secondary immune deficiencies, HIV/AIDS constituting the vast majority. More recently, the number of heterosexual men and women increased, indicating an epidemiological change in the profile of this cohort.
Since its inception, we included and followed 548 HIV-1 positive patients on this service, 500 of whom remaining under active follow-up. Ten patients died during follow-up and no information is available for the remaining 38 as on September 30, 2016. Assuming that 30% of the participants lost to follow-up are dead, an assumption adopted by a recent Canadian study, 6 we estimate that an additional 12 of our patients would have died.
As of September 2016, the mean follow-up time of the cohort was 11.6 years. Thirty-one percent of the asymptomatic at-entry progressed to AIDS, with an incidence rate of 20.3/1000 person-years; the death rate was 6.7 per 1000 person-years, meaning that one-third of the AIDS patients (8% of the cohort) died over this 20-year period. A Kaplan–Meier survival analysis showed that the probability of remaining AIDS-free was 50% at 20 years, whereas that of surviving was higher than 75% (Figs. 1 and 2). According to current Brazilian guidelines for HIV treatment, almost all subjects are currently under treatment with ART, with few exceptions (poor adherence, refusal to take medications, and other reasons). We also usually perform the resistance genotyping test before ART and for viral load rebound, with active drug failure vigilance; only 26 (5.2%) patients on active follow-up have a detectable viral load (>50 copies/ml), compared with an average of 20% for Brazil as a whole.
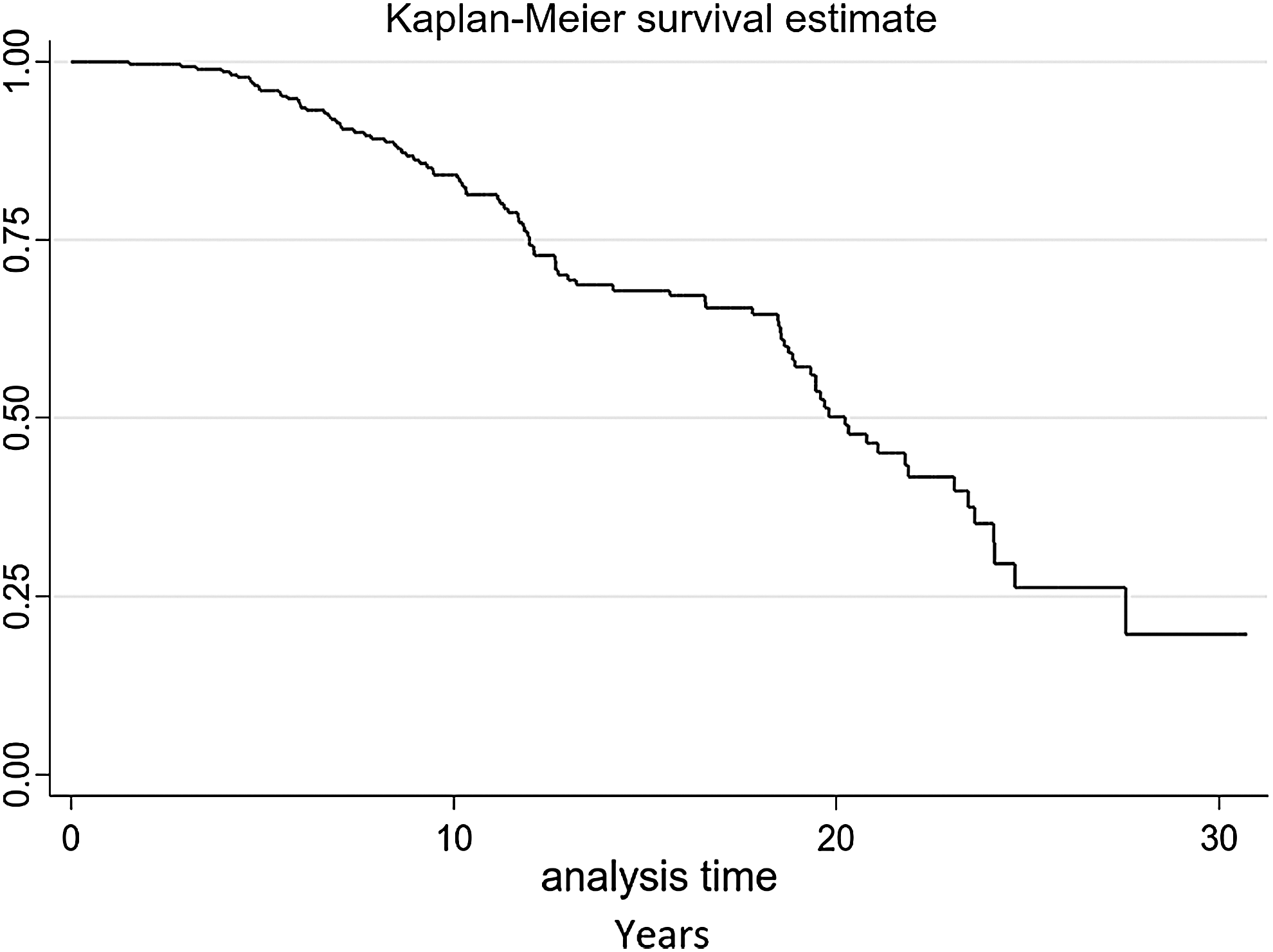
Progression to AIDS from 465 patients for 30 years of follow-up.
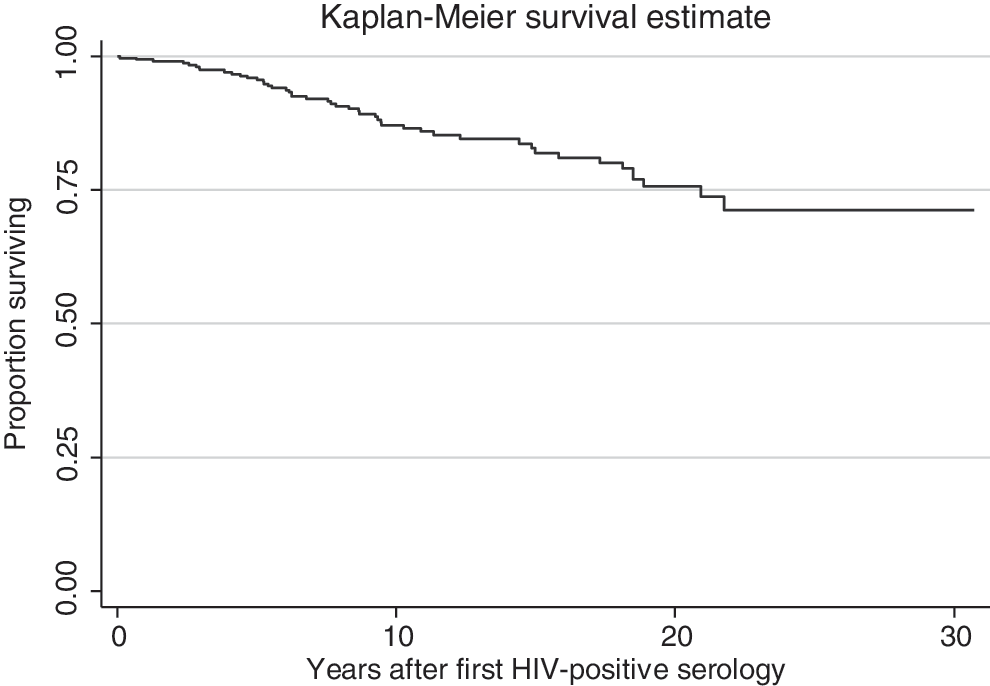
Probability of survival after first known HIV-positive serology from 465 asymptomatic-at-entry patients.
Despite the difficulties to follow and retain patients for a long time in the public health service, special programs may bring about increased chances of survival and better quality of life, as well as higher rates of retention in care; this is also true for middle-income developing countries such as Brazil. Our relatively small outpatient service (∼500 HIV-infected patients) may not mirror the reality encountered in other settings, including São Paulo city, but retention and high quality of care may improve rates of virological success, even in poorer settings. Furthermore, prevention of depression or anxiety, with discussion in groups of patients with the presence of a therapist, regular HIV RNA viral and CD4 cells counts, genotyping tests pre-HAART, and vigilance for drug failure, may explain this successful experience.
We should also take into consideration that our cohort consists mostly of asymptomatic at-entry patients referred by the Blood Bank of São Paulo, located at the same hospital, implying that they had a better immunological status at start than the more usual HIV population. Besides that, the degree of adherence to treatment in our service, in general, is quite high and the patients have a higher mean educational level: >90% of the patients a high school or college education. 7 Such features make this cohort a very specific and differentiated sample. To extend our findings, we intend to conduct similar studies in other HIV treatment centers, enabling comparisons of populations with different profiles.
Footnotes
Acknowledgments
The authors thank the following members of ADEE3002 group: Arthur Paiva, Francini Correia, Leopoldo Trevelin, Livia M.C. B. V. da Costa, Mariana A. Monteiro, Maira C. Lima, Mauricio D. Ferreira, Riccardo Moraes, Rosa A. dos Santos, Thiago E. Sabino, Wagner Alves. For patients assistance: M. Olimpia R. Freitas, M. Theresa Figueiredo, M. Cristina Renzo, Noemia Orii, Rosangela Araujo, Eduardo Martins, Gabriela Prates, Rosa Stellin.
This study was supported by Ministério da Saúde do Brasil, Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP), Fundação Faculdade de Medicina, Conselho Nacional de Pesquisa (CNPq).
Author Disclosure Statement
The authors declare that they do not have any conflict of interest related to this paper.